
Abstract
Human parainfluenza viruses (HPIVs) are among the major causes of respiratory infections in children, worldwide, including in Korea. There are four types of HPIVs, each with different epidemiological characteristics. HPIV3 is the most frequently circulating HPIV type, while the epidemiology of HPIV4 remains unclear. The aim of this study was to investigate the age-stratified seropositivity rates of HPIV types 1–4 among children in Korea. These data will be useful to determine vaccine requirements. This study included 245 participants categorized into four age groups: 6–11 months, 1 year, 2 years, and 3–5 years. Hemagglutination inhibition (HAI) assay was used to measure the antibody titers in the serum samples of the subjects. Overall, a significantly higher seropositivity rate (68%) was observed for HPIV3 (p < 0.001), indicating the predominant circulation of this type. In the 3- to 5-year-old group, 97% of the participants displayed seropositivity for HPIV3, suggesting that most Korean children acquire HPIV3 infection by the age of 5 years. The seropositivity rate for HPIV3 increased with age (p < 0.001); a prompt rise was observed between the 6–11 months age group and the 1-year age group. The seropositivity rates of HPIV1, HPIV2, and HPIV4 were found to increase with age (p < 0.001), with a marked increase recorded after the age of 2 years. HPIV1, HPIV2, and HPIV4 tended to infect children later than HPIV3. Older children showed high antibody titer ranges for HPIV3 (p < 0.001), suggesting that children experience multiple HPIV3 infections. An increasing trend of HPIV4 seropositivity rates with age was observed and this was comparable to theHPIV1 and HPIV2 seropositivity rates, indicating that its incidence may have been underestimated. To reduce HPIV infection, the administration of a HPIV3 vaccine to children 1 year of age is likely to be the most effective option.
Introduction
H
Noninfluenza RNA respiratory viruses (NIRVs) represent a public health concern globally. Along with influenza viruses, NIRVs are the leading cause of pediatric hospital attendances in industrialized countries and the leading cause of death among children in underdeveloped countries (24). The World Health Organization's Battle against Respiratory Viruses initiative aims to prioritize research and promote the development of antiviral agents and vaccines against these viruses (26). While the burden of HPIVs is not as high as that of respiratory syncytial virus (RSV), HPIVs have emerged as major pathogens causing respiratory infections in children younger than 5 years of age, particularly in Europe, the eastern Mediterranean region, the United States, Brazil, China, Japan, and Korea (1,4,5,7,10 –12,14,15,18,19,25). HPIVs were reported to account for 2–18% of pediatric hospitalizations due to respiratory diseases in the United States (1,25). In 2009, the Korea Centers for Disease Control and Prevention (KCDC) implemented a nationwide respiratory virus surveillance system, targeted at HPIV types 1–3, and reported an increasing trend of infections caused by these HPIV types. Infections caused by HPIV types 1–3 contributed to 5–15% of all pediatric hospitalizations, as well as visits to emergency departments and outpatient clinics, in Korea (11). Despite the substantial burden of HPIV infections, no specific antiviral agents or vaccines are available for protection against these viruses (3,9,22).
The seroprevalence among the healthy population acts as a record of prior infection and present immunity in healthy individuals and is useful in determining the necessity and optimal age of vaccination. The reported HPIV seroprevalence study was conducted in Japan among children with presumed respiratory tract infection (28). To the best of our knowledge, there are no reported studies on HPIV seroprevalence among healthy children. Moreover, differences in HPIV circulation prevalence may result in different seroprevalence rates according to geographical regions. The aim of this study was to investigate the seropositivity rates of HPIV types 1–4, stratified by age, among healthy children in Korea. The results will be useful in establishing strategies for vaccine development against HPIVs.
Materials and Methods
Study participants and sample collection
This cross-sectional study was conducted from November 2016 to June 2017 in St. Paul's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. The participants were recruited among healthy children attending the pediatric outpatient department for blood tests. Blood tests were required either as part of the preoperative assessment for children undergoing elective surgery, such as tonsillectomy and strabismus surgery, or as a part of a health examination, for anemia screening, lead level screening, hepatitis B viral marker testing, allergy testing by parental request, and health assessments required by kindergartens for new admissions. Residual blood following the blood test was collected. Parents or the legal representatives of children were informed that the amount of blood sampling volume would not be increased due to purpose of study. The participants were not offered any remuneration. The following exclusion criteria were applied, with symptoms assessed over the preceding 5 days or at the time of hospital attendance: (1) body temperature ≥37.5°C, measured by tympanic thermometer; (2) febrile sensation or headache reported by the child or a caregiver; (3) respiratory symptoms, such as cough, coryza, and nasal congestion; and (4) gastrointestinal symptoms, such as vomiting, diarrhea, and abdominal pain. Immunocompromised children were also excluded. While the particular age at which the passively acquired maternal antibodies against HPIVs decay has not been documented, maternal antibodies against most respiratory viruses decay within the first 6 months of life (17). Therefore, this study included children 6 months to 5 years of age, and they were categorized into four groups: 6–11 months, 1 year, 2 years, and 3–5 years of age.
The parents or legal representatives of 245 children provided consent for their children to participate in the study and permitted the use of residual blood following blood testing. Demographic data for all participants were collected. The residual venous blood samples (2–5 mL) were collected and were subject to centrifugation. To measure the antibodies against the four types of HPIV, each participant's serum sample was aliquoted and stored at −70°C. The study protocol was approved by the Institutional Review Board of the study site (PC16TISI0009). Written informed consent was obtained from the parents or legal representatives of all the participants before commencing the study.
HAI assay
The antibodies against HPIVs were assessed using HAI assay (21). The frozen serum samples were incubated overnight at 37°C with a receptor-destroying enzyme (Denka Seiken Co., Ltd., Tokyo, Japan) to eliminate nonspecific inhibitors during HAI testing. After this step, to inactivate the receptor-destroying enzyme, the serum samples were incubated at 56°C for 30 min. The serum was serially diluted twofold from 1:10 to the final dilution of 1:640 and placed in 96-well plates. The serum was incubated with an antigenic suspension (four hemagglutination units of HPIV1, HPIV2, HPIV3, or HPIV4) for 15 min at room temperature, followed by the addition of a guinea pig erythrocyte suspension. The antigenic reagent was provided by Denka Seiken Co., Ltd. Hemagglutination was interpreted after 1 h by two people using the naked eye. The antibodies to HPIV block hemagglutination, preventing the attachment of the virus to the erythrocytes, and the jagged shield of the erythrocyte will not appear. The highest dilution of serum that inhibited hemagglutination was regarded as the antibody titer of the serum. Serum samples with an antibody titer ≥1:10 were considered seropositive (21,28). Serum exhibiting hemagglutination with all dilutions (from 1:10 to 1:640) was considered seronegative. All the samples were tested consistently by well-trained personnel.
Statistical analyses
All statistical analyses were performed using the MedCalc statistical software (version 17.6; MedCalc Software, Ostend, Belgium). Descriptive statistics were used to summarize data. Chi-square tests were used in the calculation of the seropositivity rates with 95% confidence intervals (CIs) and comparison of the seropositivity rates between age groups. For all statistical analyses, p-values <0.05 were considered statistically significant.
Results
This study included 245 participants, and their age and sex distributions are presented in Table 1. The overall seropositivity rate of the participants was 17% (95% CI 16–26%) for HPIV1, 13% (95% CI 12–24%) for HPIV2, 68% (95% CI 62–71%) for HPIV3, and 11% (95% CI 8–15%) for HPIV4 (Fig. 1). The seropositivity rate of HPIV3 was significantly higher than that of HPIV1, HPIV2, and HPIV4 (p < 0.001).
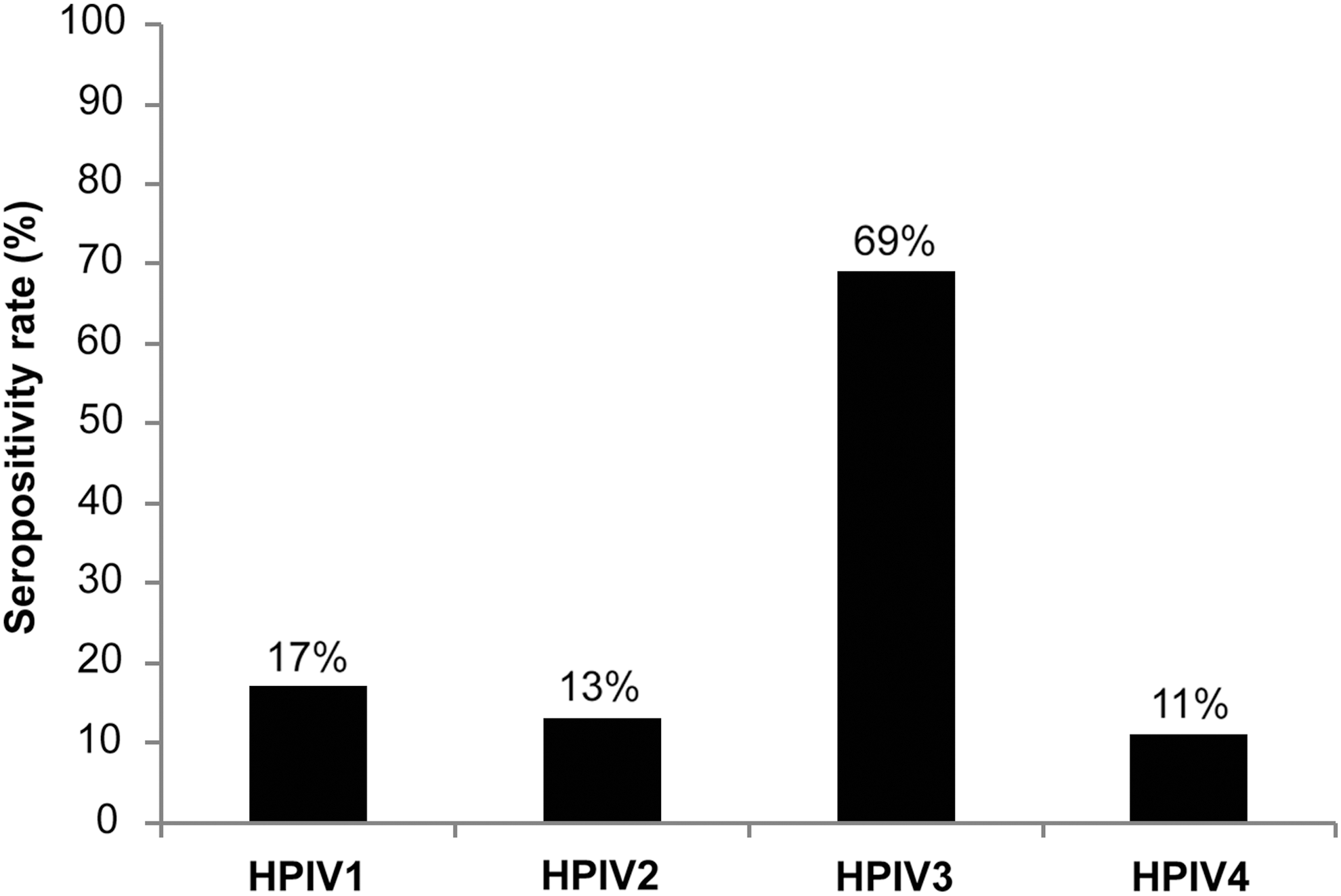
Overall seropositivity rates for HPIV types 1–4. HPIV, human parainfluenza virus.
The seropositivity rates of the HPIV types 1–4, stratified by age group, are shown in Figure 2. For HPIV3, the seropositivity rate was 10% (95% CI 7–15%; age 6–11 months), 66% (95% CI 52–74%; age 1 year), 82% (95% CI 76–89%; age 2 years), and 97% (95% CI 91–100%; age 3–5 years). The seropositivity rate increased with age (p < 0.001), and a marked increase was observed between the 6–11 months and 1-year age groups. For HPIV1, the seropositivity rate was 0% (95% CI 0–0.02%; age of 6–11 months), 9% (95% CI 4–15%; age 1 year), 14% (95% CI 10–26%; age 2 years), and 38% (95% CI 34–50%; age 3–5 years). The seropositivity rates for HPIV2 were as follows: 0% (95% CI 0–0.01%; age 6–11 months), 7% (95% CI 2–16%; age 1 year), 11% (95% CI 5–19%; age 2 years), and 30% (95% CI 26–38%; age 3–5 years). The seropositivity rates for HPIV4 were 0% (95% CI 0–0.01%; age 6–11 months), 5% (95% CI 1–11%; age 1 year), 9% (95% CI 3–14%; age 2 years), and 27% (95% CI 23–36%; age 3–5 years). For HPIV1, HPIV2, and HPIV4, the seropositivity rates increased with age (p < 0.001), and sharp increases were observed between 2 years and 3–5 years.
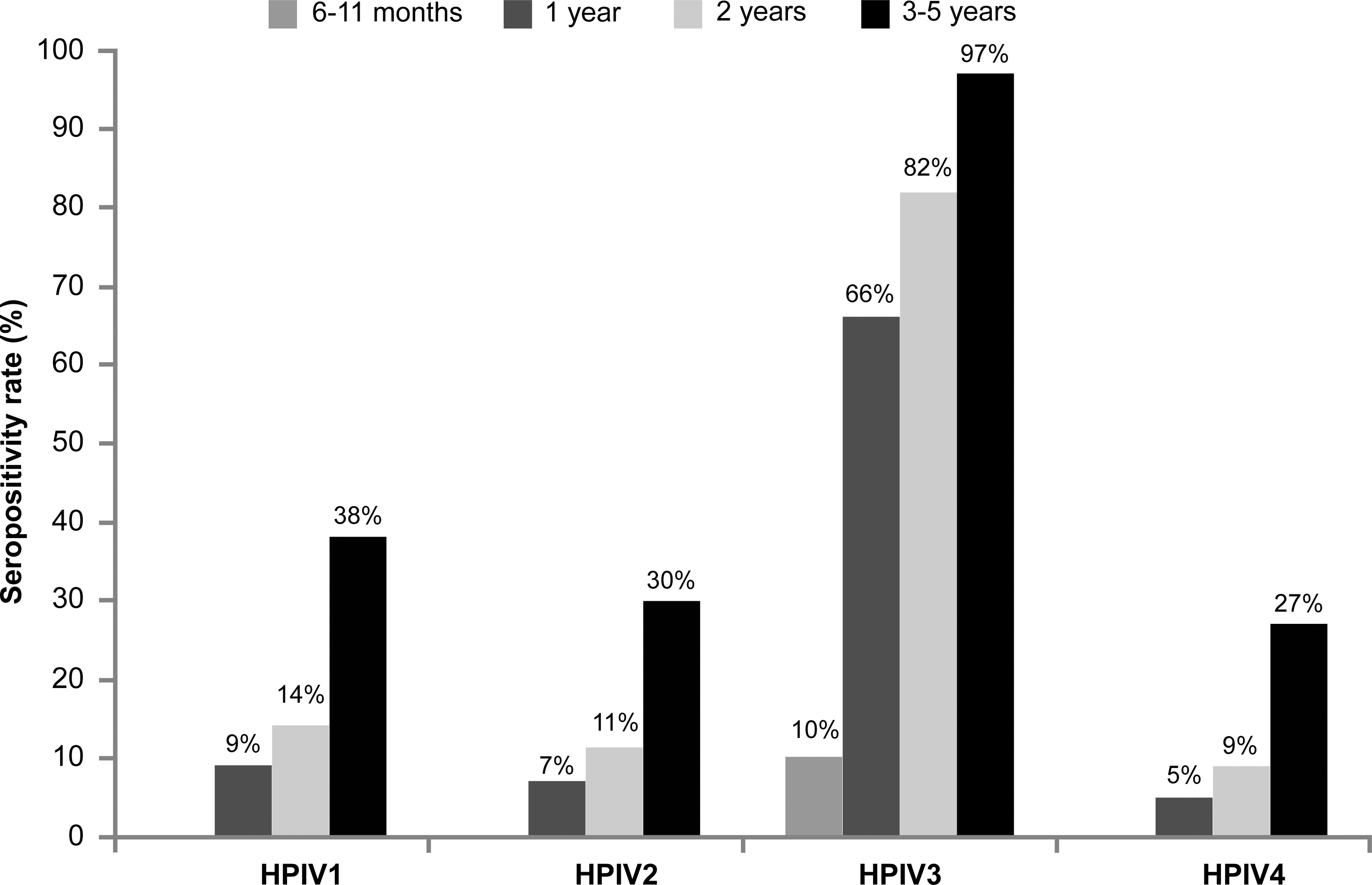
Seropositivity rates for HPIV types 1–4 stratified by each age group. None of the participants younger than 1 year of age showed seropositivity for HPIV1, HPIV2, and HPIV4.
The distributions of the antibody titers are shown in Table 2. For HPIV3, the number of participants with high antibody titers increased with age (p < 0.001). In the seropositive cases of HPIV1, HPIV2, and HPIV4, all the participants demonstrated low antibody titers, 1:10 (Table 2).
HPIV, human parainfluenza virus.
Discussion
Serological studies of HPIV have been conducted among children in the United States and Japan, although there are limited data on healthy pediatric populations (3,28). In this study, we examined the seroprevalence of antibodies against the HPIV types 1–4, among healthy children in Korea below 5 years of age. These findings will be useful in establishing a vaccine development strategy. The survival of HPIVs is influenced by environmental factors and while the optimal conditions for each type of HPIV have not been determined to date, HPIVs are relatively labile at temperatures above 37°C and lose infectivity if frozen, or exposed to heat or low humidity (9). The differences in climate may account for differences in HPIV epidemics by region and there may be regional variations in the serological status against HPIVs. Korea has a temperate climate with a hot summer and 3 to 4 months of very cold and dry winter, and usually experiences less humidity and lower temperatures than regions in which previous serological studies were conducted. However, patterns of seroprevalence were similar in United States, Japan, and Korea. It is important to generate data on the serological status of children across the world.
In this study, the overall seropositivity rate of HPIV3 was 68%, which was the highest among all the serotypes assessed. This indicates that HPIV3 is the most predominantly circulating serotype in Korea. HPIV3 has been most frequently detected in epidemiological studies conducted in the United States, Brazil, Europe, southern China, and Japan, and its circulation was found to peak between spring and summer in temperate climates, and during the dry season in tropical climates (5,7,10,12,15,18,19,28). In the United States, the incidence of HPIV1 peaks in autumn, biennially, whereas HPIV2 circulates in autumn, annually (1,19). The seasonal patterns of HPIVs may vary by geographical region. However, the surveillance in Korea, undertaken by the KCDC, demonstrated similar patterns of seasonal distribution. Among the serotypes detectable in the surveillance, HPIV3 was the most prevalent, and outbreaks were observed from late spring to the beginning of summer (April–July) every year. Incidences of HPIV1 and HPIV2 infections were observed from autumn to winter, every year, but the incidence was not as high as that of HPIV3 (11). These epidemiological findings correlate with the serological status of children in Korea. HPIV3 is the serotype children are most commonly exposed to, and notably, the highest overall seropositivity rate was observed for HPIV3.
According to a seroprevalence study performed in Mie Prefecture—a southern coastal city of Japan—children 3–4 years of age presented with seropositivity rates of 96.5%, 49.1%, 40.4%, and 59.6% to HPIV3, HPIV1, HPIV2, and HPIV4, respectively (28). In a study conducted in the United States, by 5 years, 90–100% of children have antibodies against HPIV3, 60–75% have antibodies against HPIV1 and HPIV2, and more than half have antibodies against HPIV4 (3). In the present study, those aged 3–5 years demonstrated a 97% seropositivity rate for HPIV3, whereas the seropositivity rates for HPIV1, HPIV2, and HPIV4 were 38%, 30% and 27%, respectively. This result emphasizes the prominent circulation of HPIV3 in Korea. The finding that most children encounter HPIV3 infection by the age of 5 years coincides with the results of studies conducted in the United States and Japan (3,28). The seropositivity rates of children in Korea 3–5 years of age to HPIV1, HPIV2, and HPIV4 are lower than those observed in children in the United States and Japan (3,28); this could be attributed to the relatively lower incidence of HPIV1, HPIV2, and HPIV4 in Korea. Korea has extremely cold and dry winters, from December to February, and the incidence of HPIV1 and HPIV2 decreases abruptly during the transition from autumn to winter (11). Further investigation of the seasonal patterns of HPIV4 is required.
The distribution of the HPIV types are known to differ based on age, among infected patients. HPIV3 infections are common in children younger than 12 months of age, whereas HPIV1 and HPIV2 usually affect children after infancy; it is not yet clear which age group is most targeted by HPIV4 (3,9). The current study presented similar patterns of age distribution. The seropositivity rate for HPIV3 rose rapidly from 10% at 6–11 months of age to 66% at 1 year. This finding indicates that children in Korea usually encounter an HPIV3 infection at 1 year of age. A sharp increase of seropositivity rates were observed between 2 and 3–5 years, for HPIV1, HPIV2, and HPIV4, suggesting that children in Korea, HPIV1, HPIV2, and HPIV 4 infections occur after the age of 2 years. Children in Korea may acquire HPIV3 infection first at the age of 1 year, and HPIV1, HPIV2, and HPIV4 infections after the age of 2 years.
The participants demonstrated higher antibody titers for HPIV3 with increasing age. All the seropositive participants 6–11 months of age presented with antibody titers of 1:10, more than one-third of seropositive children 1 year of age presented with antibody titers of 1:20 or 1:40, more than one-third of seropositive children 2 years of age presented with antibody titers of 1:40 or 1:80, and more than one-third of seropositive children 3–5 years of age presented with antibody titers of 1:160 or 1:320. A study conducted in Japan also showed higher antibody titers in the higher age groups, for HPIV3 (28). The results suggest HPIV3 reinfection. Antibodies against these viruses are generated 2 weeks after the onset of symptoms, but the antibody titers are low; therefore, immunity wanes quickly, and reinfection cannot be prevented (4,9). Children encounter multiple infections of HPIV3 and their antibody titers increase. Many clinical observations report that HPIV3 reinfections induce milder symptoms than primary infections (9). All the participants who were seropositive for HPIV1, HPIV2, and HPIV4 exhibited antibody titers of 1:10. HPIV1, HPIV2, and HPIV4 are not as prevalent as HPIV3, and children do not experience HPIV1, HPIV2, and HPIV4 infections as frequently as HPIV3 infections.
HPIV4 is difficult to grow in tissue culture and is associated with mild symptoms; therefore, HPIV4 testing is not included among commercially available respiratory virus detection tests and even publicly in many countries (6,13,20). HPIV4 has two subtypes, HPIV4a and HPIV4b, based on the results of HAI assays and neutralization tests, although the differences in the clinical manifestation of infection caused by the two subtypes are unknown (13). The contribution of HPIV4 to respiratory disease has not been recognized. However, studies published in China and the United States reported that HPIV4 is an important etiology in lower respiratory infections in children (6,13,20), often causes severe symptoms, and is similar to HPIV3 in clinical manifestation (6). According to a study conducted in Japan, children 3–4 years of age showed higher seropositivity rates for HPIV4 than for HPIV1 or HPIV2 (28). In this study, the seropositivity rates and the increasing trend of seropositivity rates for HPIV4 were similar to those for HPIV1 and HPIV2. HPIV4 may be more prevalent than previously thought, in Korea, and its incidence may be similar to that of HPIV1 and HPIV2. Studies on the seasonal patterns, age distribution of infected patients, and clinical features of HPIV4a and HPIV4b are required.
The results of this study suggest that the administration of the HPIV3 vaccine during the first year of life is the most effective strategy to reduce HPIV infection in Korea. Despite advances in vaccine development, vaccines to some major human pathogens, including HPIVs, remain unavailable (27). Intranasal vaccines that induce local antibodies at the mucosal surface of infection sites have been investigated for seasonal respiratory viruses, such as influenza, RSV, and HPIVs (2,8,16,22,23). Intranasal vaccines against HPIV3, including the HPIV3 cold passage mutant 45 vaccine and bovine HPIV3 vaccine, have been developed in the United States, and underwent phases I or II clinical trials, but did not proceed to phase III due to insufficient immunogenicity (8,16,22). The development of vaccines against HPIV3 should be continued.
This is the first study assessing the seroprevalence of HPIV types 1–4 among healthy children. However, some limitations need to be addressed, specifically, the small number of participants, the relative short study period, and the fact that the study was conducted in a single region in Korea. Further studies are required, involving a greater number of healthy subjects in different regions over several years. The accumulation of data on the serological status of healthy children in different regions is important to confirm the necessity of vaccines against HPIVs and is crucial for vaccine development.
Conclusion
This study aimed to assess the seroprevalence of HPIV types 1–4 among healthy children in Korea. Despite the small number of participants, several important findings were observed. HPIV3 was the most predominant type of circulating HPIV, and our results indicate that most children in Korea develop antibodies against HPIV3 by 5 years of age. Furthermore, children usually acquire a primary HPIV3 infection at 1 year of age and experience reinfection thereafter. HPIV1, HPIV2, and HPIV4 infections tend to occur later than HPIV3 infections, after 2 years of age. The results of this study suggest there is a need for HPIV3 vaccination in Korea among children 1 year of age. Research on serological HPIV status of children by region is required and the development of HPIV3 vaccines should be continued. The contribution of HPIV4 to respiratory disease may have been previously underestimated, and public sectors, including the KCDC, need to incorporate HPIV4 in the respiratory virus surveillance system, to investigate the epidemiological features of HPIV4.
Footnotes
Acknowledgments
The authors thank the study participants. This study received no specific grant, and was financially supported by the corresponding author, U.Y.C.
Ethical Statement
The study protocol was approved by the Institutional Review Board of St. Paul's Hospital, College of Medicine, The Catholic University of Korea (PC16TISI0009). Signed informed consent was obtained from the parents or legal representatives of all the participants.
Author Disclosure Statement
No competing financial interests exist.