
Abstract
In Pakistan, around 11 million people are infected with, at least, six circulating genotypes and subtypes of hepatitis C virus (HCV). The viral burden is still on rise. HCV genotype determination is necessary to devise appropriate antiviral therapy. Previous reports highlight the prevalence circulating untypable (in diagnostic perspectives) HCV subtype in local Pakistani patients. Present study was designed to investigate the epidemiological distribution of genotypes in different districts of Punjab, Pakistan and focuses on prevalence of diagnostically untypable subtype and its possible antiviral therapy. A total of 8,353 HCV patients were included through 2011 to 2016 for determination of HCV prevalent genotypes in the local community. HCV genotyping was carried out using Ohno et al. method, and five cases of diagnostically untypable patients were treated with interferon-based antiviral regimen to find the possible treatment strategy. Of the 8,353 patients, the genotype 3a (n = 6,650, 79.6%) was most significantly prevalent throughout the study period followed by undetermined genotype that is, untypable (n = 1,377, 16.5%). The presence of untypable variants suggested that there are some novel or quasi species prevailing among HCV patients in local community. Five HCV patients infected with untypable genotype had been treated effectively with interferon alpha plus ribavirin therapy for 24 weeks at standard doses and achieved sustained virological response. This study highlighted an important aspect of HCV treatment for local Pakistani HCV patients. Untypable HCV variants could be treated with interferon-based antiviral regimens such as 3a genotype. The study raises the need of characterization of diagnostically untypable HCV variant. On the basis of these results, it can be proposed that until the availability of pangenotypic direct-acting antiviral for HCV treatment in Pakistan, interferon-based antiviral regimens will be of choice for majority of patients infected with 3a or untypable genotypes.
Background
Hepatitis C virus (HCV) is a major health concern in Pakistan. Accurate viral genotyping is very critical for proper treatment of the infected individuals as the sustained virological response (SVR) of the standard antiviral therapies is genotype dependent. Genotypes that are not detectable by the current diagnostic methods are considered untypable. According to this large scale study, untypable HCV variants are prevalent in large number of patients in the country, that is, n = 1,377 (16.5%) after 3a. It is evident from case studies that interferon plus ribavirin therapy is helpful in clearing the disease in individuals infected with HCV untypable genotype. This may be a solution to the problem of untypable variants, until this mystery be solved.
Introduction
P
HCV is a plus stranded RNA virus (8). The genome is translated in the form of a polyprotein, which is then cleaved by host and viral peptidases into ten different proteins (16). The viral proteins are divided into structural and nonstructural proteins–core, E1, and E2 are classified as structural proteins, whereas NS2 and NS5 are classified as nonstructural proteins (14). The virus has an error prone polymerase with an error rate of polymerase 10−3 per nucleotides per replication (1). Due to this error prone nature, the virus results into different genotypes and subtypes. Mainly the virus is classified into seven different genotypes (15). Viral genotyping is done from a conserved region of 5′ untranslated region (5′ UTR), core, envelope glycoprotein, and viral polymerase. Different gene sequences in these regions resulted into emergence of different genotypes. The diversity in these regions leads to the identification of different viral genotypes.
In Pakistan, the most widely used method for HCV diagnosis is of Ohno et al., which is designed on the basis of conserved region of 5′ UTR (21). Mutations in this conserved region results into loss of genotyping efficiency and those viral variants are classified as diagnostically untypable (6,7).
Pakistan is a country with low socioeconomic status, and there is no health insurance system in the country. The government budget for health department is also very low. Previously the major antiviral treatment option for HCV was interferon based (22) and may be a choice for majority in the near future as well. The major reason may be that direct-acting antivirals (DAA) are very costly and that only sofosbuvir is available in Pakistan on discounted rate. In current scenario, it seems very difficult to treat all 11 million patients with DAA. The major prevalent genotype in Pakistan is 3a that could easily be treated with the cost-effective cheaper interferon-based antiviral therapy. Proper diagnosis of viral genotyping is a requirement for clinicians to start the antiviral therapy because the duration and efficacy of both interferon-based regimes and DAA are genotype dependent (4). The course and fate of interferon-based antiviral therapy also vary considerably. If a prevalent viral strain is classified as untypable, it will be very difficult for healthcare providers to properly treat the patient (10), which will not only result in loss of treatment efficiency but also create enormous social and economic burden on society. Keeping in mind the current scenario, the study was aimed to evaluate the presence of diagnostically untypable HCV variants in different districts of Punjab, Pakistan. Furthermore, few cases infected with untypable HCV were also treated to propose a suitable therapy for patients infected with untypable HCV variants.
Methodology
Sampling
The study was conducted from January 2011 to June 2016. Total of 9,261 ELISA positive samples were included in this study from different districts of Punjab province, including Lahore, Sahiwal, Okara, Hafizabad, Faisalabad, Gujarat, Toba Tek Singh, and Multan (Fig. 1). The study was approved by the Ethics Committee of Lahore Clinical Laboratory and Research Center, Lahore, Pakistan and by the Institutional Bioethics Review Committee (IBRC) of Department of Life sciences, University of Management and Technology, Lahore.
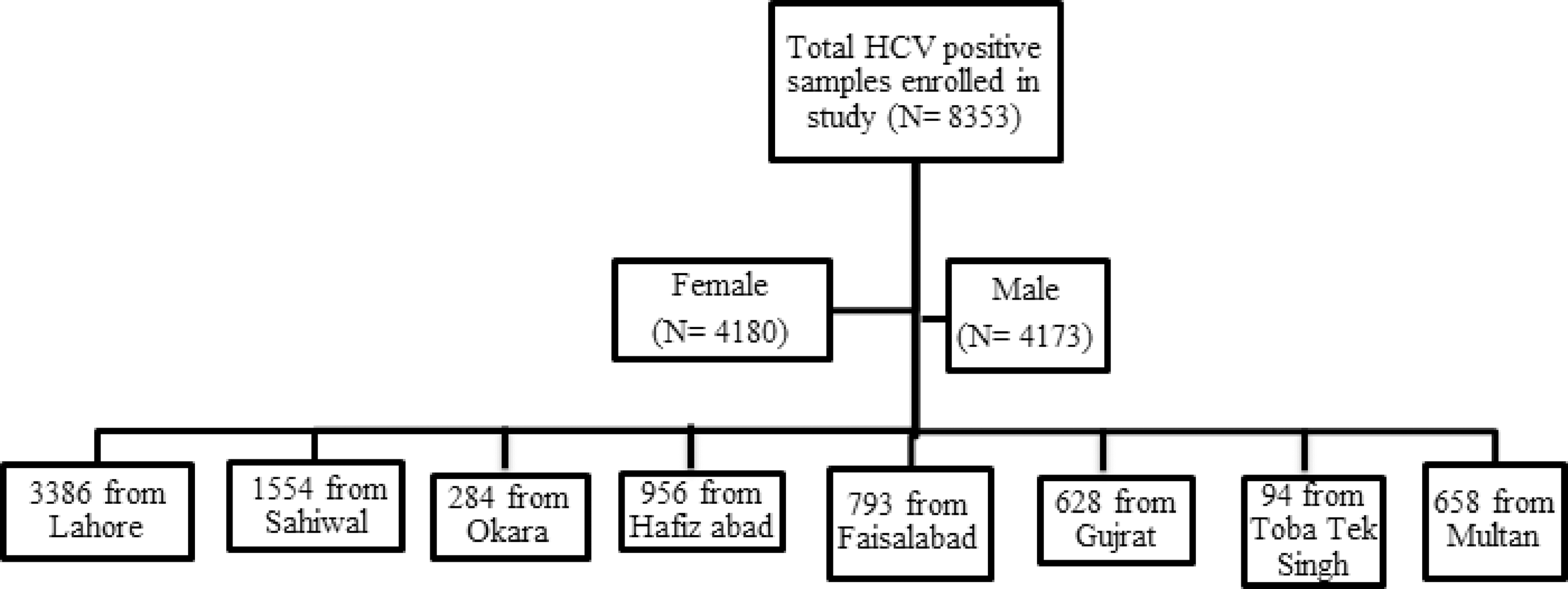
Distribution of patients enrolled in study in eight districts of Punjab (Pakistan).
HCV qualitative test
Serum collection of 9,261 patients was done from blood, and then RNA was extracted from serum using QIA amp Viral RNA MINI kit (Qiagen-Germany). According to the manufacturer's protocol 10 μL Viral RNA was used. 5′ UTR was reverse transcribed using Moloney Murine Leukemia Virus Reverse Transcriptase (M-m LVRTase- Invitrogen) in a reaction volume of 20 μL for 60 min at 37°C. The amplified cDNA of 5′ UTR was used as template DNA for first round PCR. The first round PCR reaction was made by using sequence-specific primers and then a second round nested PCR was performed using internal-primers (21). The PCR product of first round (1 μL) was used as template for the second round of PCR (nested). Both the first and second round PCR were done with Taq DNA polymerase (Invitrogen) for 40 cycles. Amplified DNA products of the second round were run on 2% agarose gel electrophoresis and visualized by using a gel documentation system (Fig. 2). All PCR positive samples were reconfirmed by using HCV RG-RT PCR kit on real-time Rotor gene equipment (Qiagen).

Representative image of gel electrophoresis showing results of HCV qualitative test. Lane 1 showed PC; lanes 2–9 and 12–18 showed HCV-positive samples with band size 210 bp; lanes 10–11 showed negative results of suspected individuals. HCV, hepatitis C virus; PC, positive control.
HCV genotyping
All HCV positive samples were then subjected for genotyping. Typically six different genotypes were detected using the method of Ohno et al. (21) Viral RNA (10 μL) was used to synthesize cDNA through reverse transcription using 200 U of M-mLVirus RT at 37°C for 60 min. The first round PCR was carried out using 5 μL of the synthesized cDNA using 5′GGGAGGTCTCGTAGACCGTGCACCATG-3′ as forward primer and 5′-GAGACGGGTATAGTACCCCATGAGAGTCGGC-3′ as reverse primer. The product from the first round (1 μL) was then taken to perform a second round PCR by forming Mix 1 and Mix 2. Mix 1 contained primers for genotype 1b, 2a, 2b, and 3b, while genotypes 3a, 4, 5a, 1a, and 6a were in Mix 2. Amplification enzyme used for all PCR amplification reactions was Taq DNA Polymerase (Invitrogen). The second round PCR amplified product (10 μL) was then electrophoresed on 2% agarose gel with DNA marker of 100 bp and visualized using gel documentation system. HCV genotype was confirmed on the basis of specific PCR band size (Fig. 3).
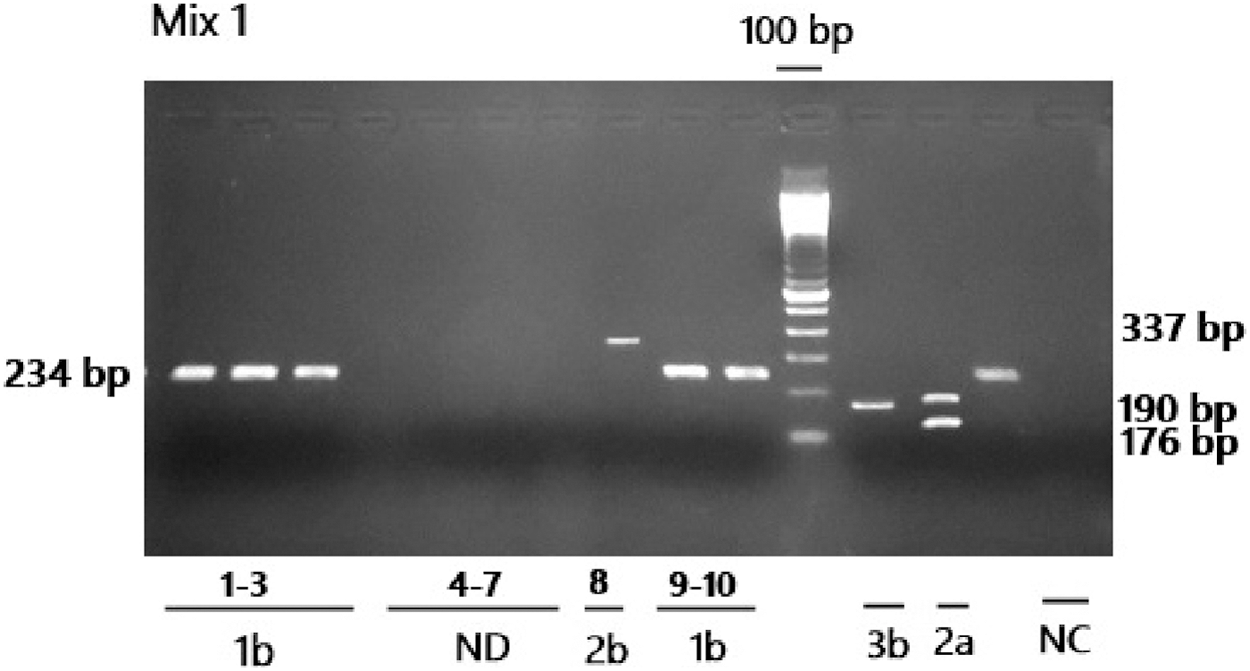
Representative image of gel electrophoresis showing results of HCV genotyping for mix 1. Mix 1 contained primers for genotype 1b, 2a, 2b, and 3b; ND: Not Determinant (untypable) lanes 4–7; NC: Negative control lane 15.
Five cases of HCV patients infected with untypable HCV variant were also included in study, which may facilitate the treatment strategy for undetermined genotype. All these cases followed the same diagnostic procedures similar to other study participants.
Results
Out of 9,261 ELISA positive samples, 8,353 (90.1%) samples were PCR positive. The genotyped samples were further analyzed on the basis of gender, age, and city/district. Out of total, 4,180 (50.1%) patients were female, while 4,173 (49.9%) were male. HCV-positive individuals were distributed in various districts of Punjab, such as 3,386 (40.5%) from Lahore (fairly big and capital city of Punjab), 1,554 (18.6%) from Sahiwal, 956 (11.4%) from Hafizabad, 793 (9.4%) from Faisalabad, 658 (7.8%) from Multan, 628 (7.5%) from Gujarat, 284 (3.3%) from Okara, and 94 (1.1%) from Toba Tek Singh (Fig. 1).
The distribution frequency of different genotype and subtypes was determined and evaluated. Among the 8,353 patients, the genotype 3a (n = 6,650, 79.6%) was most significantly prevalent throughout the study followed by undetermined genotype that is, untypable (n = 1,377, 16.5%) (Table 1). The frequency of diagnostically untypable HCV variants varies over the study period. The frequency of individuals infected with untypable HCV genotypes ranged from 12% to 19% through 2011 to 2016 (Fig. 4).
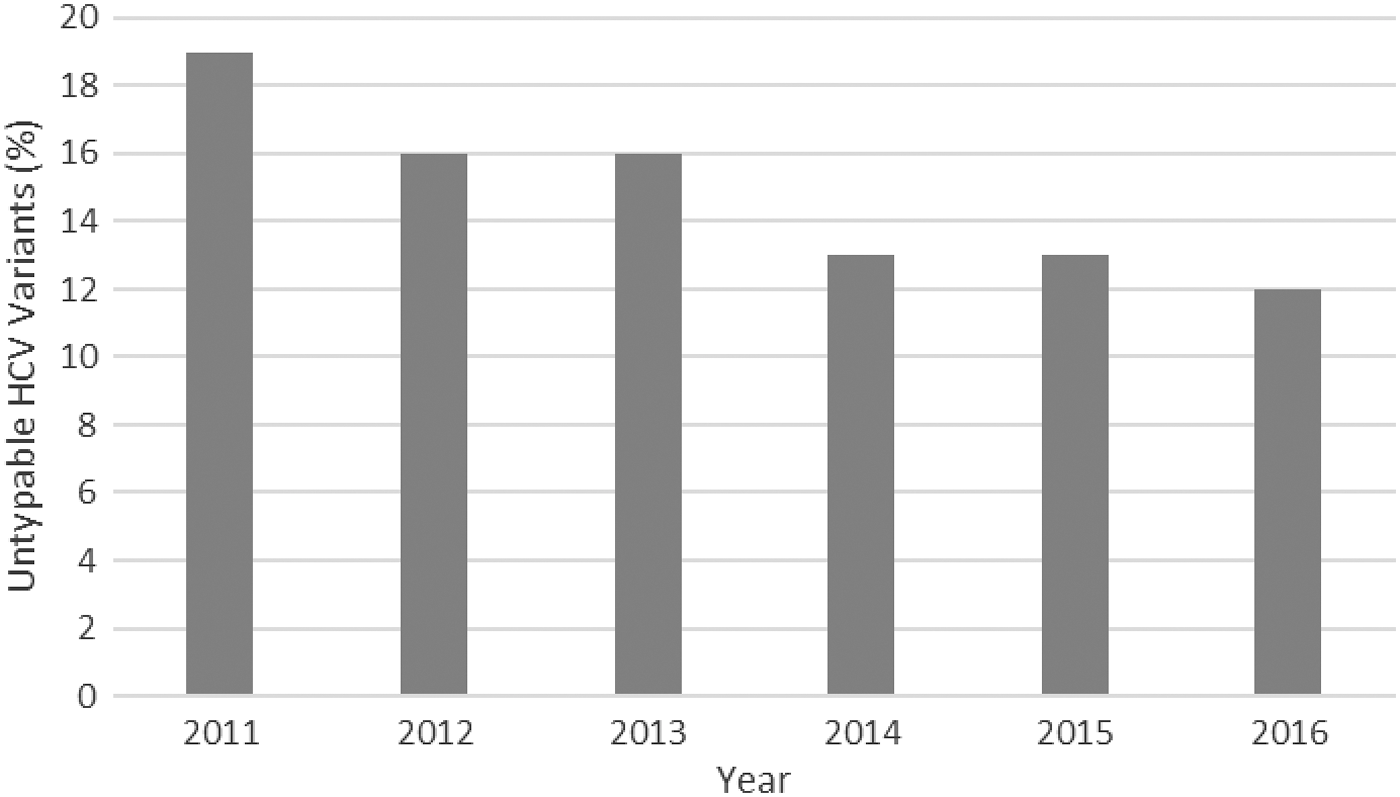
Year-wise prevalence of diagnostically untypable HCV variants in Punjab, Pakistan.
HCV, hepatitis C virus.
Case studies
In March 2015, a 40-year-old male presented to the hospital with anti-HCV-positive result (the patient value was 2.80 and reference range was 0.45). Anti-HCV was performed by an immunochromatographic screening method. Hepatitis virological report was positively reconfirmed quantitatively by Real-Time PCR (“PIKO REAL” Thermo Scientific). The viral load detected was 8.4 × 104 copies/mL.
According to the medical history, the patient was taking alcohol for the last 7 years before presentation and had developed Hepatitis C. He was also presented with moderately elevated liver enzymes that correlate clinically with enlarged fatty liver and sludge seen in gall bladder. The symptoms were headache, irritability, feeling lethargic, and numbness of mind, dizziness, low mood, and weeping spells (Table 2). HCV genotyping was carried out by Ohno et al. method, but the genotype was undetectable (infected with untypable HCV variant). Three other male (aged 35, 37, and 40 years) and a female (aged 32 years) patients infected with HCV untypable genotype were also included in the analysis. These patients were also included in March 2015 in this study. Their demographic and clinical characteristics are mentioned in Table 2.
ALP, alkaline phosphatase; ALT, alanine transaminase; GGT, gamma-glutamyltransferase.
We have recently characterized an untypable HCV variant by sequence and phylogenetic analysis (unpublished data). The results showed the greatest homology of untypable HCV variant with 3a genotype from Pakistan. So keeping in mind, the antiviral therapy with peg interferon-α and ribavirin at standard doses was started for 24 weeks just as 3a. A standard dose of 3 million units three times per week was injected for 24 weeks and patient had detected with normalized alanine aminotransferase (ALT) levels. All studied patients had undetectable viral load after 24 weeks of antiviral therapy and achieved SVR. The patients were followed for next 1 year (by qualitative PCR every 6 months) and were found negative. These cases highlighted the importance of effective antiviral therapy for untypable HCV genotype, that is, interferon-α plus ribavirin.
Discussion
HCV, a blood born ailment, may lead to the development of chronic hepatitis. It may also develop hepatocellular carcinoma if infection is persistent (20). HCV burden is continuously increasing with six circulating genotypes and subtypes in Pakistan. About 11 million individuals are infected with HCV in the country, mainly due to the lack of awareness, healthcare, and educational facilities. To combat with this elevated burden, there is a need to educate the community regarding preventive measures and also to monitor the antiviral therapies coverage and efficacy. HCV genotype determination is necessary to help the healthcare facilitators for recommending the appropriate antiviral therapy. This large scale study was carried out to investigate the prevalence of different genotypes in Punjab and especially the diagnostically untypable one. The current study is a single hospital-based retrospective analysis, and in this analysis, female HCV-positive patients are higher compared with male HCV patients. However, this trend may not reflect the HCV incidence in general population because in a culture such as Pakistan, males are more prone to acquire HCV infection than females.
Knowledge about HCV genotype is a useful practice before initiating antiviral therapies. High genetic diversity has been noted in case of HCV due to nucleotide substitutions and leads to the phenomenon of genotype shift. This phenomenon leads to the diversification and the evolution of many new subgenotypes in the population that are undetectable by the old methods. It is evident that patients infected with different genotypes differ with the severity of disease and response to specific antiviral therapy. The method described by Ohno et al. is most widely used diagnostic assay in Pakistan. In this method, 5′ UTR region is used for HCV genotyping. A previous report (18) also highlighted that diagnostic test based on the 5′ UTR may result in the substantial discordance at the subtype level and in case of mixed HCV genotypic infections. Diagnostic methods such as the restriction fragment mass polymorphism and the Abbott Real-Time HCV genotype II (GT II) assay (Abbott Molecular, Inc., Des Plaines, IL), which target the 5′ UTR and NS5B region, also cannot successfully genotype all HCV variants and resulted in untypable HCV genotypes. Alternatively, by sequence analysis, untypable genotypes can be detected, thereby indicating that certain considerations are needed when applying 5′ UTR-based genotyping assays in a clinical setting. Keeping in view the current scenario of Pakistan, it is also proposed that in case of undetermined HCV genotype sequencing and molecular cloning, techniques are needed to solve the diagnostic problem.
Over the past few years, many improvements have been made in treating the disease with the introduction of DAA, but due to high cost and genotype dependence, DAA are not widely used in the developing country such as Pakistan. From last two decades, a comparable cheaper therapy, peginterferon-α plus ribavirin (RBV) is mostly recommended in Pakistan by the clinicians for the management of disease. There is increasing evidence that patient infected with different HCV genotypes may have different clinical profiles and response to alpha-interferon therapy. Genotype 3a, highly prevalent in the country, showed effective SVR to combined α-interferon therapy (19). Interferon therapy is recommended in case of genotype 3 for 24 weeks. Recent reports showed that peginterferon plus ribavirin showed SVR rate of 70–97% for genotype 3a (9 –12).
According to previous reports, genotype 3a is the most prevalent viral subtype in Pakistan (17,23,24). In accordance with the previous report, we have also observed that 3a (79%) is most abundant viral genotype in Punjab, Pakistan. Similarly, genotypes 1, 2, and subtypes are less reported in the country, and these results are comparable with other reports from the country (13,17,23 –25), while no case was found for genotype 4 and 6. The genotype 3a is followed by variants that are untypable/undetectable by current diagnostic methods used. We previously highlighted that there is continuous and significant increase in untypable variants (6). The results of current study showed the prevalence of a significant number of undetermined genotype in Punjab, that is a highly populated and well-studied province of Pakistan. The distribution frequency of untypable variants in current study is slightly different from previous studies in the country. All previously published studies were based on small number of study participants (reviewed in Refs. 4,6,8) (prevalence of HCV untypable genotype ranged from 2% to 37.8%). The current study is based on very large number of subjects (n = 8,353) and included the data of 5 years. The analysis showed that prevalence of untypable HCV variants is 16%. Due to large number of study participants, these results are more reliable compared with previous reports carried out on smaller number of individuals.
The presence of untypable variants suggested that there are some novel or quasi species prevailing among HCV patients and are not detectable by most commonly used diagnostic method (Ohno et al.) in the country. The significant number of these quasi species is consistent throughout the study period, which highlights the management and need of effective therapy for undetermined HCV variants. It is also necessary to solve the mystery to help clinicians for determining appropriate regimens in case of untypable quasi species. Therefore, the limitations of the genotype assays need to be thoroughly evaluated, and sequencing-based approaches may be needed to complement the methods in clinical settings.
Conclusion
The study was aimed to suggest a treatment option for untypable genotype that is being strengthened by case studies. Disease management is the priority in case of chronic hepatitis. Unfortunately, there is no proper treatment option for untypable genotype, but still benefit can be taken from genotype-specific treatment options. Since DAA are not widely used for untypable genotypes due to unavailability, very high cost, and genotype dependence. It has been demonstrated by case reports that the patient with untypable genotype is being treated as the most common prevalent genotype (3a) in the country. Successful treatment of untypable HCV genotypes reduces the chronic disease progression. Pakistan is a country with low socioeconomic status and a low budget for healthcare facilities. Thus, this might be great deal for significant number of untypable genotype HCV patients to be treated with a comparable cheaper therapy. This may be a solution in temporary compensation to the problem of untypable variants until this mystery has been solved. Also, a great need to make the current diagnostic methods up to the mark to recognize viral strains to help combat the HCV burden in the country effectively.
Declarations section
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Lahore Clinical Laboratory and Research Center, Lahore, Pakistan and by the IBRC of Department of Life sciences, University of Management and Technology, Lahore. For infants, informed consent to participate in the study was obtained from their parents or legal guardians before enrolling the infants in the study.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions
A.Z., M.I. and Z.H.S. handled patient enrollment and consent to participate. A.Z. and M.I. did the molecular genotyping of HCV. M.S.A. conceived of the study and participated in its design and coordination. A.Z., M.A., and M.S.A. wrote the article. All authors read and approved the final article.
Acknowledgments
We sincerely acknowledge the efforts of Ms. Mahvish Kabir for her help in English Language editing of the article.
Author Disclosure Statement
No competing financial interests exist.