
Abstract
Total or partial inactivation of the chemokine 5 (CC5) pathway, as caused by the CC5 receptor Δ32 deletion (CCR5Δ32), may result in a profound manipulation of immune surveillance with significant consequences on the course and response to therapy of diverse human infections, including HIV. It has been postulated that in chronic hepatitis C (CHC), such a deregulation of CC5 pathway may compromise T cell-dependent antiviral immune responses, which in turn may favor viral persistence. To test this hypothesis, we investigated a cohort of 100 patients with CHC in whom 12 heterozygous and 1 homozygous CCR5Δ32 mutations were detected compared to 8 and none in 98 healthy controls (13% vs. 8.2%, p = 0.36). As patients with and without CCR5Δ32 mutations were similar in terms of histological activity (p = 0.84) and fibrosis stage (p = 0.20) as well as CCR5 tissue expression, we reasonably exclude that this CCR5 mutation is significantly involved in the pathogenesis of CHC and may be a potential therapeutic target. However, deleted patients showed a significantly higher response to pegylated interferon-alfa (PEG-IFN), suggesting that a dormant immune system is more readily primed by immunostimulation.
Introduction
I
Indeed, chemokine–CCR5 interactions are important components of the immune response to viral infections where they are instrumental in recruiting effector T cells to the affected sites to mediate clearance of virus-infected cells (21). The main inflammatory chemokines, including Macrophage Inflammatory Protein (MIP)-1a, MIP-1b, and Regulated upon Activation Normal T cell Expressed and Secreted (RANTES), bind the CCR5 and have been found to regulate the trafficking of immune cells into the liver where its presence on hepatic stellate cells causes their activation to a myofibroblastic phenotype and increase matrix deposition with progressive fibrosis (1,7,19). Since the inflammatory processes underlying dysregulation of these immune cell systems may eventually lead to cirrhosis and end-stage liver disease, CCR5 pathway modulation may represent a potential therapeutic target.
Indeed, the CCR5 pathway has been investigated as relevant to the pathogenesis of hepatitis C virus (HCV)-related liver damage and also as a potential target of receptor modulation by specific antagonists (3,17,15). The interaction between HCV structural and nonstructural proteins and the hepatocytes CD81 coreceptor as well as with endothelial cells have been shown to upregulate secretion of CCR5 ligands and induce fibrogenesis (7,20). CCR5Δ32 was found to prevail in those HCV cohorts where the CCR5 pathway inactivation was associated with a persistent infection with mild inflammatory changes of the liver and a slow disease progression (3,10,11,13). However, these were not the findings of other studies in similar patients rendering the role of CCR5Δ32 in HCV infection unclear and worth to be elucidated, as it might help discovering new therapeutic interventions for hepatitis C (9).
In the present study, we analyzed the prevalence of CCR5Δ32 in a well-characterized cohort of patients with chronic hepatitis C (CHC) and assessed its possible association with liver damage.
Materials and Methods
Samples from 100 CHC patients were obtained from a single-center, published cohort characterized by well-defined length of HCV infection (12) and from 98 healthy blood donors who served as controls.
Clinical parameters
The most important demographic and clinical variables were recorded for all patients, including liver fibrosis progression rate (FPR) that was calculated as previously described (12,18), as date of infection was known for all patients (Table 1). Patients were treated with pegylated interferon-alfa (PEG-IFN) and ribavirin (weight-based doses) for 24 or 48 weeks according to genotype (8).
FPR, fibrosis progression rate; HCV, hepatitis C virus; SVR, sustained virological response; WT, wild type.
CCR 5 genotyping
Genomic DNA was extracted from whole blood using the Extraction Kit from QIAGEN (Hilden, Germany). Evaluation of CCRΔ32 was performed by polymerase chain reaction (PCR) with specific primers (Fw 5′-cttcattacacctgcagctctca-3′ and Rv 5′-cgagtagcagatgaccatgaca-3′) and PCR products were separated by standard electrophoresis on 2% agarose gels containing ethidium bromide. Interleukin 28B (IFNL4) genotype, rs12979860, was available for all HCV patients by real-time PCR.
Histology and immunohistochemistry studies
Liver biopsies were performed in all patients with a 16-gauge Tru-Cut needle and read by two independent pathologists (RDA, MM) who were unaware of patients CCR5Δ32 genotype. Histological grade and stage were semiquantitatively evaluated according to the Ishak score. Tissue sections were immunostained for CCR5 with anti-human CD195 (CCR5) antibodies (1:500; clone T21/8, eBioscience), after antigen retrieval in ph 6 citrate (Fig. 1). Positive cells were individually counted.
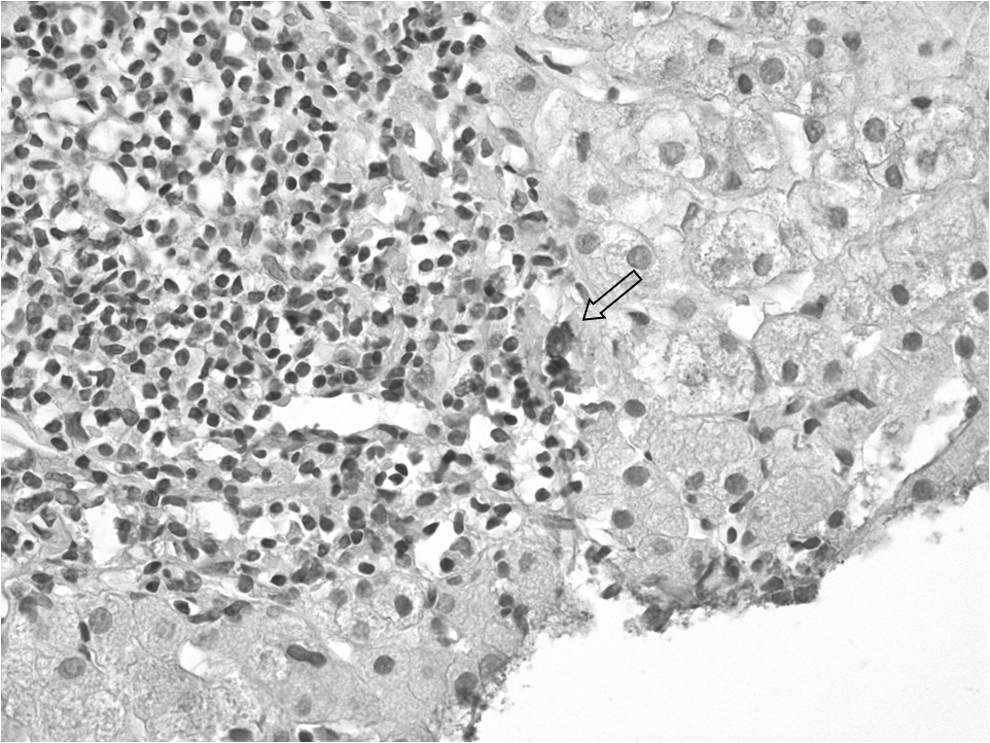
Immunohistochemistry of CCR5 using anti-human CD195 with a two-step immunoperoxidase technique. Positive lymphocytes (arrow) detected among a portal tract mononuclear cells infiltrate (20×). CCR5, chemokine receptor 5.
Statistical analyses
Statistical analyses were conducted using the Mann–Whitney U-test or the Student's t-test for continuous variables and the χ2 or Fisher's exact probability test for categorical data. A probability value of p < 0.05 was considered statistically significant. All variables with statistical significance in the univariate analysis were included in the final model and odds ratios and corresponding 95% confidence interval were computed. Calculations were done with Stata 10.0 statistical package.
Results
Among 100 patients with chronic HCV infection, 51 (51%) were males, with a median age of 47 (18–69) years. HCV genotype was 1 in 77%, 2 in 14%, 3 in 8%, and 4 in 1%. The IFNL4 rs12979860 genotype was CC in 36%, CT in 56%, and TT in 8%. Cirrhosis was histologically documented in 23% of the patients (Table 1).
When we compare the prevalence of CCR5Δ32 in our patients with a 98 healthy blood donors population of the same ethnicity, the CCR5 deletion was found in 13 patients (12 heterozygous and 1 homozygous) and in 8 healthy controls (all heterozygous) (13% vs. 8.2%, p = 0.36), with minor allelic frequencies of 0.07 and 0.04, respectively. Although not statistically significant, this difference indicates a suggestive trend. No deviation from Hardy–Weinberg equilibrium (p-value >0.05) was observed in both patients and controls.
Patients with or without CCR5Δ32 were similar in terms of clinical features (Table 1). They had similar FPR rates (p = 0.41) during a median period of 27 (7–56) months (28 vs. 27 months, p = 0.93). At histology, they also displayed similar grading (p = 0.84) and staging (p = 0.20). Interestingly, among patients carrying the CCR5Δ32 allele, none had severe necroinflammatory activity (histological grade >12). Most of them showed persistent mild liver damage and fast response to treatment after a course of PEG-IFN and ribavirin. Indeed, in the patients with available data, the sustained virological response (SVR) rate of CCR5Δ32 patients was significantly higher than that of wild-type patients, 84 versus 47% (p < 0.05), independent on IFN4L polymorphism.
The prevalence of cirrhosis was the same in the 2 groups (wt vs. mut: 23% vs. 23%, p = 1.0). In 28 patients, whose liver tissue was still available for staining, we also assessed the prevalence of positive CD195 cells (20 CCR5 wt/wt and 8 Δ32/wt). Using monoclonal anti-CD195 (CCR5) clone T21/8, only a few positive cells were found scattered throughout portal tracts, but without any significant differences in number and distribution between wild-type patients and deleted genotype. No CCR5 expressing cells were observed in the liver of the homozygous Δ32/Δ32 patient.
Discussion
The CCR5 pathway plays a major role in driving immunosurveillance of virus infections, inducing recruitment and activation of effector cells to the site of the affected tissues (16). In HIV infection, CCR5 has also been found to act as the virus coreceptor whose blockade by specific agonists are currently part of antiviral therapy protocols. Although the inactivation of the CCR5 ligands' interactions is expected to decrease immune-mediated liver injury and fibrogenesis, the role of CCR5 in CHC is only partially elucidated and remains somewhat controversial (5,6). To obtain insights on this, we studied the possible clinical impact of CCR5 on a selected cohort of patients where a nonsignificant higher prevalence of the Δ32 mutation in HCV patients compared with healthy controls was observed. Our findings are consistent with the reported Δ32 allele frequency ranging from 5% to 12% in Europe with a North–South gradient, while homozygous account for 0.7–1.6% (11,13). Indeed, we found a single homozygous individual in our patient population. At variance with HIV where the Δ32 mutation is protective in a recessive model, in our HCV cohort both CCR5Δ32 heterozygous and homozygous showed a mild liver damage, suggesting a dominant effect of the Δ32 deletion. A higher Δ32 allele prevalence rate was reported in a cohort of hemophiliacs where it could reflect the selection of individuals with HIV resistance (23). In this as well as in larger cohorts of HCV patients, a trend toward a higher prevalence of the Δ32 deletion was reported to be associated with mild hepatic inflammation and reduce clearance of HCV (10,14). On the contrary, other authors reported on a similar distribution of the Δ32 allele frequency in patients with CHC and controls, but in association with an increased spontaneous viral clearance (9). However, the deleted genotype may favor HCV persistence or associate with aggressive cell-mediated immune reactions, as observed in a hepatitis mouse model (6). When assessing the potential role of CCR5 genotypes on disease grade and stage, we did not observe any significant difference between patients with or without CCR5D32, as shown also in previous studies on larger patient populations (5). However, none of them was in the highest grade category in keeping with the hypothesis of a decreased immune-mediated liver injury. In our cohort, this seems to be associated with a SVR to PEG-IFN-ribavirin combination therapy, which was significantly higher in patients carrying the CCR5D32 genotype than in wild type, as if a dormant immune response was more readily activated by exogenous inducers. No association of carriage of the CCR5 allele with response to IFN-based therapies has been observed in another study where CCR5 genotype did not add to IFN4L polymorphism predictive value (15).
Indeed, only a few, sparse isolated CCR5 positive cells were detectable in the liver both in wild-type and deleted patients, either in the portal tract or in the parenchyma, but without any specific pattern. This appears to be consistent with the expected decrease in liver inflammation induced by the CCR5 deletion. On the contrary, Morad et al. observed an increased liver inflammation in their patients and explained this apparent discrepancy by the recruitment of cytotoxic T-cells following the activation of CXCR3 and CXCR6 during CHC (15).
This as well as the lack of an association with host and viral genotypes seems to rule out a relevant role of this pathway in CHC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.