
Abstract
Hepatitis B is a clinically important public health issue. Infection leads to hepatocellular carcinoma. Therefore, patients need antiviral therapy for prolonged period to prevent the complication of the disease. Data concerning chronic hepatitis B (CHB) patients with high hepatitis B virus (HBV) DNA are limited. The aim of the study was to check the efficacy of the nucleoside reverse transcriptase inhibitors (tenofovir) in terms of suppression of HBV DNA. The secondary end point in the study is to evaluate trends of predictive variables that predict outcome of treatment. In this specific study, we evaluated 140 CHB male and female patients, of these 110 completed 48 weeks of treatment. On the basis of hepatitis B e antigen (HBeAg), patients were stratified; HBV DNA and hepatitis B surface antigen (HBsAg) levels were measured along with liver function tests. All enrolled patients were given tenofovir disoproxil fumarate 300 mg daily before breakfast. Overall, 69.1% of patients showed virologic response. HBeAg-negative patient group showed 68% viral suppression and HBeAg-positive patient group showed 45.9% over 24 months of treatment, while at 48 months it was shown to be 76.7% and 54.1%, respectively. None of the patients suffered HBsAg loss during the 48 months. Baseline high HBV DNA level was found as a significant predictor of response (OR, 1.9; 95% CI = 1.23–3.9, p = 0.005). None of the patients observed had serious adverse events. Mutations in the RT region of polymerase gene are shown to be associated with resistance to antiviral drugs. Among patients suffering with chronic HBV infection, HBeAg-negative patient group have better virologic response as compared with HBeAg-positive group. Higher concentration of HBV DNA at baseline has negative prediction for sustained viral suppression. The A-B motif interdomain rtL122F mutation was found in nonresponder patients in our study. Another mutation rtN248H observed in E motif considered to have effect on DNA primer grip, which forms part of binding pocket.
Introduction
C
HBV when untreated for a long time causes severe liver infection ranging from mild to severe; that is, from few weeks to lifelong illness (21). Antiviral therapies are used to suppress liver complication and are of significant importance in determining the outcome of CHB. With current available medications, suppression of the virus replication, ALT normalization, hepatitis B e antigen (HBeAg) seroconversion, and hepatitis B surface antigen (HBsAg) loss can be achieved in most patients (12 –14,19). Studies have shown that the main goal of antiviral therapy is to continuously suppress HBV replication (9,23,24,41), which helps attain improved liver histology and delay in liver disease progression. Treatment regimens used for HBV suppression are pegylated interferon for a period of ∼48 weeks and oral nucleos(t)ide analogs for indefinite duration. Nucleotide analogs (NAs) are well tolerated, safe to use, and showed significant efficacy. Tenofivir disproxit fumarate (TDF) is a potent NA used for HBV. Targeting of HBV reverse transcription by administration of NA has become the cornerstone in the treatment of HBV in the last few years. Management of CHB patients is evolving rapidly due to the availability of wide treatment options and significantly improved the ability to predict therapeutic response in CHB patients (20,22). Till now, three oral nucleosides (lamivudine, telbivudine, and entecavir) and two NAs (adefovir and tenofovir) have been approved for CHB patients' treatment (43). However, administration of nucleos(t)ide for long time may be associated with histological aggravation, resulting in the development of antiviral resistance (42,45).
Current guidelines recommend that a single agent holding potent antiviral activity and high genetic barrier, such as of tenofovir or entecavir, be initiated as first-line antiviral agents for chronic hepatitis B patients (1). TDF treatment has been recommended as a first-line therapy for the treatment of CHB patients, as well as among those who were resistant to lamivudine, telbivudine, adefovir, and entecavir (22,32).
HBV has a DNA genome, and its life cycle depends upon transcription catalyzed by reverse transcriptase, a type of HBV DNA polymerase that consists of 344 amino acids. Mutations have been identified throughout the HBV genome (structural and nonstructural genes) due to low fidelity of polymerase, high replication rates, and overlapping reading frames across the genome (5). Mutations within the reverse transcriptase might alter the antigenicity, encapsidation, and virulence of virus, resulting in resistance to drug during antiviral treatment (40).
The aim of the study was to check the efficacy of the nucleotide reverse transcriptase inhibitors (tenofiver) in terms of HBV DNA, and second to analyze variables that predict treatment outcomes, and also mutational substitutions are assessed in light of therapeutic response in the patient.
Method
Study design
This study was carried out at Maroof International Hospital, Islamabad, from May 2014 to June 2016. The prospective study was designed by digestive disease study group of Maroof International Hospital and approved by ethical committee of the hospital. One hundred seventy patients were accessed. Of these, 140 CHB patients were enrolled in the study, per the given criteria: HBsAg positive for at least 6 months and positive polymerase chain reaction for HBV DNA detection; moreover, patients who did not suffer from any disease such as decompensate liver disease and autoimmune disorders, or have any history of cardiac diseases and depression. In addition, patients who presented with coinfection by hepatitis C virus, hepatitis D virus, or human immunodeficiency virus (HIV) and those with previous or concurrent use of oral NAs were excluded. Before the commencement of treatment, patients' complete blood count, prothrombin time, ALT, HBV serologic markers (HBeAg and HBsAg), and quantitative HBV DNA were determined. HBV DNA was >20,000 IU/mL for all the patients in the study. Commercial immunoassays (Abbott Laboratories, Abbott Park) were used to measure the levels of serologic markers, including HBsAg and HBeAg. Patients were administered 300 mg TDF before breakfast. The duration of treatment was 48 weeks, while the patients were observed in outpatient department every 4 weeks for determining HBV serologic markers (HBeAg and HBsAg).
Measurement of HBV DNA
Blood samples were collected in Vacutainer tubes without anticoagulant. They were incubated for 30–45 min for clotting, after which centrifugation was done at a speed of 4,000 rpm for 15 min for removal of clot, and serum was collected in fresh Eppendorf tube and stored at −20°C until further analysis. Serum viral DNA levels were evaluated by an automated real-time PCR test based on a dual-labeled hybridization probe targeting the precore and core regions. HBV DNA extraction from a serum sample of 500 μL was performed on COBAS Ampli-prep instrument (Roche Diagnostics, Pleasanton, CA). COBAS TaqMan 48 was used for quantification of viral load. Sensitivity was set at 20 IU/mL with a dynamic range from ∼54 to 1.1 × 108 IU/mL (25,31). Serum HBV DNA levels were evaluated quantitatively at 4-week intervals till 48 weeks Fig. 1).
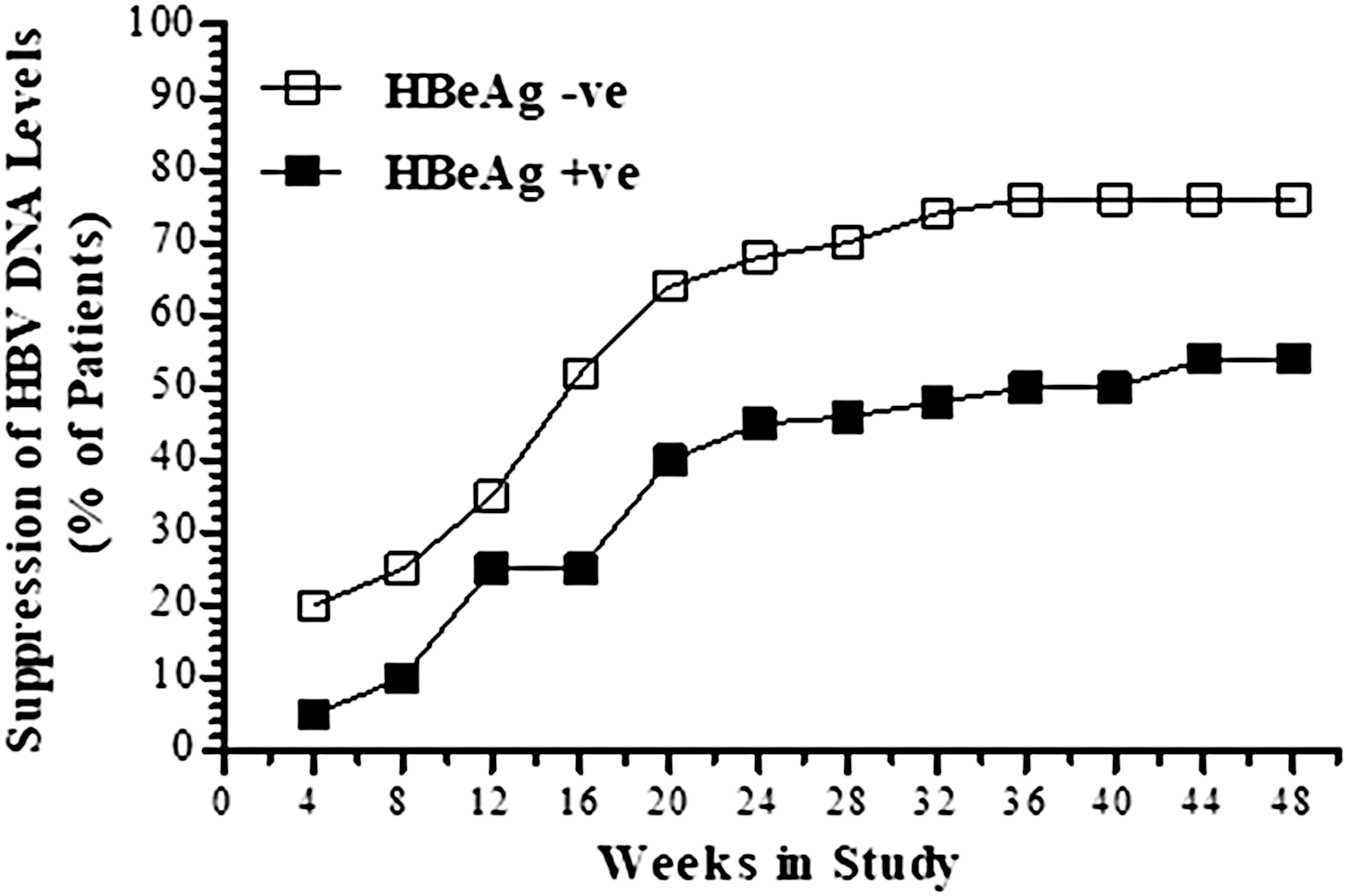
Proportion of patients achieving virologic response in HBV patients. HBeAg, hepatitis B e antigen.
Assessment of efficacy
The primary end point for efficacy was defined as HBV DNA level or HBV DNA not detected below the detection limit of the assay (i.e., 20 IU/mL) until the last follow-up visit. Secondary end point for efficacy was the detection of HbsAg loss, seroconversion of HBeAg, and normalization of alanine aminotransferase.
Sequencing
Sequencing of the sample was performed using primer set, which amplified 1143–1860 bp of pol/RT region. The sequences obtained were compared with HBV sequence in NCBI nucleotide database using the Basic Local Alignment Search Tool
Statistical analysis
SPSS version 16 for windows was used for data analysis. The result for all variables was reported in rates (%). Pearson's chi-square method was used to measure variable association with response. A two-sided p-value below 0.05 was considered significant. To identify factors associated with response to antiviral therapy, multivariable logistic regression stepwise procedure was performed. Significant predictors of therapy response according to univariable analysis were further analyzed using multivariable logistic regression to identify the independent predictors of treatment outcome. A subanalysis was done by adding pol/RT region sequence analysis of responder and nonresponder patients.
Result
Baseline characteristics of patients
One hundred forty patients were enrolled in this study. Patients' characteristics are mentioned in Table 1. Mean age was 35 ± 7 years; 49 (44.5%) were female and 61 (55.45%) were male. Patients were divided into two groups at baseline HBeAg level. Serologic profile showed that 61 (55.5%) patients were HBeAg negative and 49 (44.5%) were HBeAg positive (Table 1). Higher HBV DNA level was found in HBeAg-positive patients than in HBeAg-negative patients. However, median HBV DNA level was 8.0 × 105 IU/mL.
ALT, alanine aminotransferase; BMI, body mass index; HBV, hepatitis B virus; HBeAg, hepatitis B e antigen.
Virologic response
The level of HBV DNA was progressively reduced, and viral load suppression was found higher over week 24. After 48 weeks of treatment, overall 69.1% (76/110) virologic response was achieved in HBV-infected patients. A proportion of virologic response was calculated in HBeAg-negative and HBeAg-positive patients. It was found to be 76.7% (56/73) in HBeAg-negative patients and 54.1% (20/37) in HBeAg-positive patients. A statistically significant (p = 0.015) difference in virologic response was reported between HBeAg-negative and HBeAg-positive patients. HBeAg-negative patient group showed a response rate of 68% and HBeAg-positive patient group showed 45.9% over 24 months of treatment, while at 48 months it was shown to be 76.7% and 54.1%, respectively, as shown in Figure 1.
Biochemical response
Variation in ALT levels was widely observed among study groups. Subjects undergoing treatment were divided into two groups mainly on the basis of serum ALT levels; that is, raised ALT level group (male ≥41 U/L, female ≥31 U/L) and normal ALT level group (male <41 U/L, female <31 U/L). ALT normalization was observed among HBeAg negative and positive patients with higher ALT levels at baseline. ALT normalization was 75% vs. 65% at week 24 and 74% vs. 73% at week 48. This difference was not statistically significant (p = 0.07) (Fig. 2).

ALT normalization in HBV patients over time. HBV, hepatitis B virus; ALT, alanine aminotransferase.
Serologic response
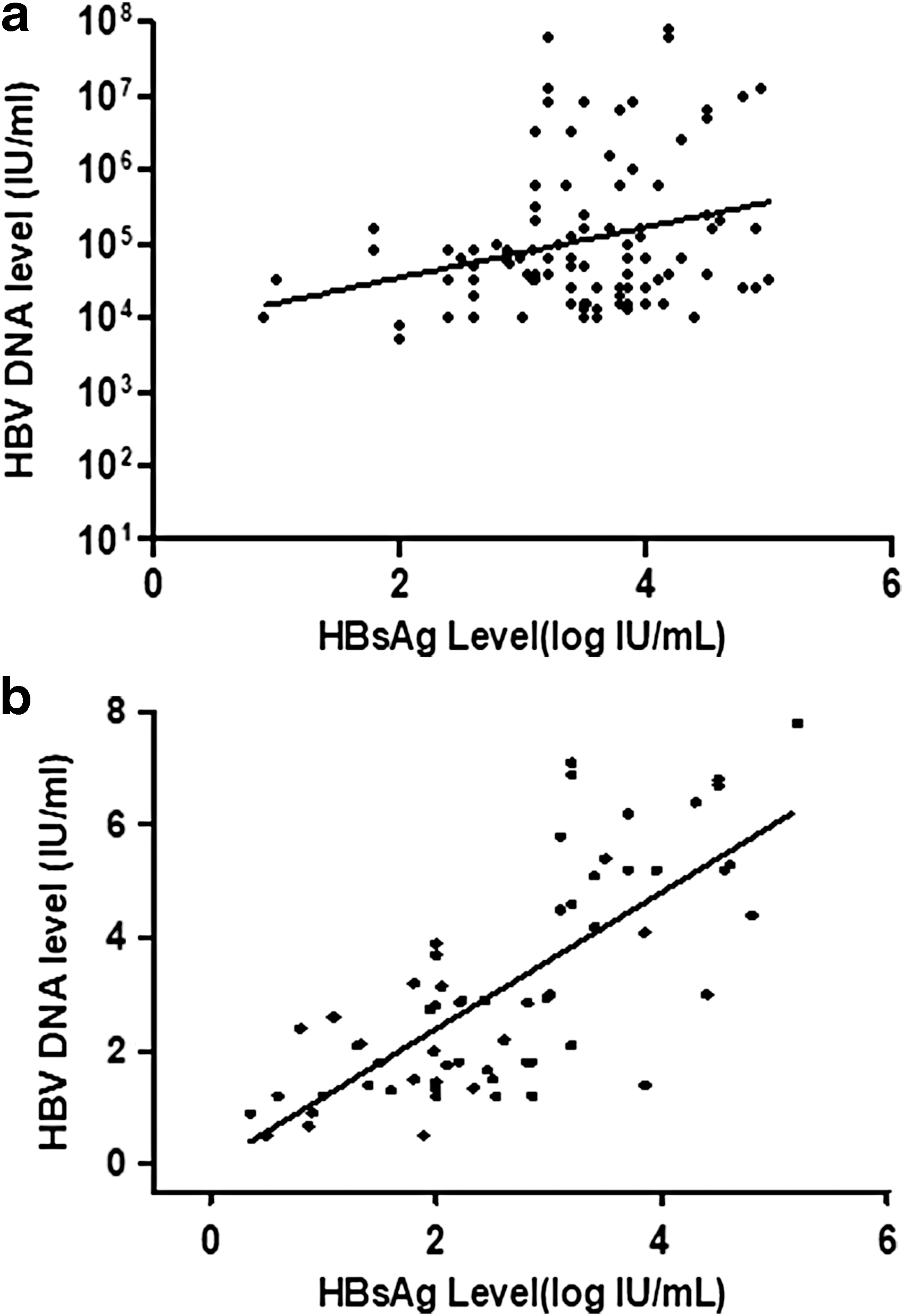
Serologic analysis confirmed that none of the patients lost HBsAg and reported HBeAg seroconversion during the 48-week treatment of the study. Before treatment, the median HBsAg level was 4.8 log10 IU/mL (range, 2.11–6.2). This level was detected considerably higher in HBeAg-positive patients as compared with HBeAg-negative patients (4.8 vs. 3.7, p = 0.002) log IU/mL. To find the correlation in HbsAg levels and HBV DNA, patients were grouped separately; one group showed virologic response (undetectable HBV DNA) and other group showed detectable HBV DNA after treatment for 48 weeks. Fifty percent of HBV patients showed HBsAg levels >3 log 10 IU/mL at baseline Figure 1. In addition, HBsAg values were significantly found higher in patients with high HBV DNA than in those with low HBV DNA before treatment. However, these changes in HBV surface antigen and viral DNA were not observed after treatment in each patient (Fig. 3a, b).
Detection of Nucleotide Substitution in pol/RT Region
Sequence region from nucleotide 1143–1860 bp of pol/RT region was amplified, and sequences were aligned using CLC Main Workbench version 6.0. The amino acid alignment of motif E (rt246-260 nt) from nonresponder patients showed specific patterns as compared with responder patients to tenofovir. Nonresponder patients showed a replacement of leucine to phenylalanine at amino acid position rt122 (rtL122F mutation; nucleotide substitution C to T at 1380 bp). We noted that nonresponder patients showed substitution asparagine to histidine in E motif at rt248 amino acid positions (rtN248H mutation; nucleotide substitution from A to C at 1758 bp position) (Fig. 4). Furthermore, the substitution difference between responder and nonresponder patients is not significant.
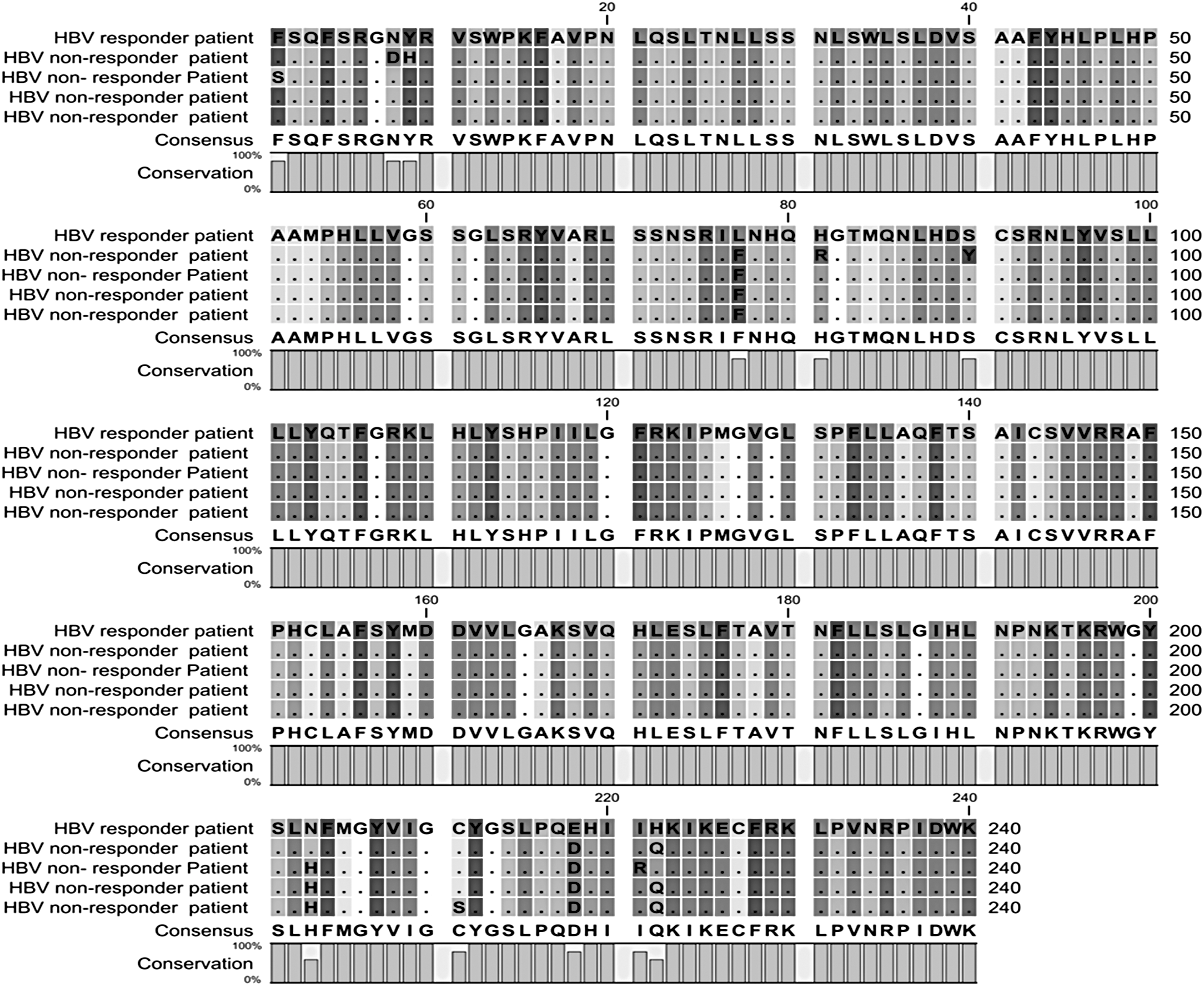
The amino acid alignment of pol/RT region of responder and nonresponder patients using CLC sequence viewer. The conserved amino acid sequences are shown as dots. Consensus sequence of amino acid is presented at the bottom, and the number above the sequence is amino acid number. Mutation RtL122F has position of amino acid at 77 and rtN248H has position of amino acid at 203.
Factors contributing to response
The strongest factor predicting antiviral therapy response was baseline viral load, which was considerably lower in the responder as compared with the nonresponder group.
Univariable logistic regression analysis
Factors associated with viremia suppression identified by univariable logistic regression analysis were age, sex, baseline HBV DNA, HBeAg at baseline and baseline ALT. Variables associated with response are patients with HBV DNA ≤ 106 IU/mL and > 106 IU/mL(OR, 1.9; 95% CI = 1.23–3.9, p = 0.005). Patients ≤ 40 years had higher rates of virological response compared to patients >40 years (OR,1.6: 95% CI = 1.06-2.55, p = 0.03). Baseline ALT >3-times ULN (upper limit of normal serum level) (OR, 2.1; 95% CI = 4.34−7.13, p = 0.001) and baseline HBeAg negative status (OR, 1.3;95% CI = 0.15-0.97, p = 0.04) (Table 2).
VR, virologic response.
Multivariate logistic regression analysis
Factors associated significantly with virologic response found by univariable logistic regression (HBV DNA ≤106 IU/mL, baseline ALT >3 times ULN, baseline HBsAg-negative status) were analyzed using multivariable logistic regression, and baseline HBV viral load (OR, 1.8; 95% CI = 1.6–5.5, p = 0.006) and baseline HBeAg-negative status (OR, 1.5; 95% CI = 5.5–6.7, p = 0.04) were found as significant predictors (Table 2).
Discussion
The main aim of CHB treatment is suppression of HBV viral replication, to induce diminution of liver disease leading to hepatocellular carcinoma and cirrhosis, and of passing the infection to others. Six therapeutic agents were used widely for CHB treatment. Less side effects were observed by using NAs compared with interferon therapy (15).
Data analysis showed that none of the patients with HBsAg loss during the follow-up were found. However, data from the prospective study have shown overall decline in median HBsAg levels from baseline to the completion of treatment (Figs. 2 and 3). Decline in serum HBsAg levels during and after completion of therapy indicates improved level of host immune control against the virus, and it may associate better with lessened amounts of cccDNA (4,7,38). It was observed that viral load of HBV DNA fluctuates, but serum HBsAg level remains relatively stable (33,34). Previous studies reported superior antiviral efficacy of tenofovir to adefovir dipivoxil.
In agreement with earlier studies, tenofovir showed effective virologic response (76/110) 69.1% in hepatitis B patients. This can be compared with the response rate (67%) predicted by Bakhshizadeh et al. (2). In another study, Bilge et al. reported 71.3% suppression at 48th week of treatment (3). Treatment with TDF resulted in virologic suppression in HBeAg-negative and positive patients. Several studies reported (17,23) that effective viral suppression was caused by TDF in both HBeAg-negative and positive patients. Marcellin et al. reported undetectable HBV DNA level at 76% in HBeAg-positive and 93% in HBeAg-negative naïve patients (23). However, noticeably higher virologic response rates were observed in HBeAg-negative patients as compared with HbeAg-positive patients (Fig. 1).
In this study, HBeAg clearance rate observed was 28% in HBeAg-positive patients, which was different from that reported by Van Bömmel et al.; that is, 24% (35). In addition, we observed that HBeAg clearance rate did not predict virologic response rate. In another study, Ceylan et al. reported that HBeAg levels did not affect virologic response (6). HBeAg-negative and positive patients showed different biochemical response rates; however, difference was not significant. Gordon et al. (16) reported that extended treatment with tenofovir directly related with higher HBV DNA negativization rates (98–99%), and higher HBeAg and HBsAg negativization and seroconversion rates.
DNA level is considered as an independent predictor of therapeutic response. It also acts as a signal for active replication of virus, which is considered as a driving force for disease progression (9,18). Patients were stratified on the basis of viral load at baseline. Higher viral load was found in HBeAg-positive patients. Effect of treatment was determined, and rapid viral suppression was found in all patient groups. In agreement with previous report, we found that patients with higher viral load take longer period to reach the targets at which the level becomes undetectable. In all, 49.3% of HBeAg-negative patients have baseline viral load >107 IU/mL compared with 56.8% of the HBeAg-positive patients. Decline in HBV DNA level is higher in patients at week 12. Patients with high viral load showed higher level of viral replication and predicted to take longer period to reach undetectable target (Fig. 3a, b).
Previous studies reported 3% HbsAg loss in tenofiver-treated hepatitis B patients who were resistant to other antiviral therapeutic agents (34). But Chang et al. reported HbsAg loss in 1.4% of hepatitis B patients treated in their study group. Contrary to the reports of previous studies, no HbsAg loss was observed. Several studies have demonstrated a correlation between HBV DNA and HBeAg levels (8,10,27). In our study, the results of HBsAg quantification were analyzed for correlation with quantification of HBV DNA. HBsAg values were found significantly higher in patients with elevated HBV DNA levels than in those with low HBV DNA levels before treatment. The correlation between HBsAg and HBV DNA levels in treated group was generally lower than that in the baseline group due to rapid reduction of HBV DNA level than HBsAg titer after tenofiver treatment (Fig. 2). This inconsistency in HBV DNA and HBeAg may vary due to variation status of disease, such as presence of HBeAg and anti-HBe antibodies (37).
A number of drug resistance mutations of HBV located in RT/pol region have been identified. Mutations in this region are shown to be associated with resistance to antiviral drugs and almost all the oral antiviral regimens targeting RT region of polymerase gene. The RT region of HBV contains highly conserved motifs (A, B, C, D, and E). The A-B motif interdomain rtL122F mutation was found in nonresponder patients in our study. In a previous study, Zheng et al. concluded that mutations in A-B interdomain may be associated with necroinflammation and immune response (44). However, Singla et al. who found rt122 mutation in their study state such mutations as naturally occurring mutations with no biological significance (30). They found rtN248H mutation, also observed in our study. Our reported rtN248H mutation lies in E motif within this region. E motif is considered as DNA primer grip that forms part of the binding pocket. Mutations in this region impart consequence on polymerase activity and RNase H activity (36). In another study, Qin et al. report the novel rtN248H mutation in E motif, and found an increase in resistance toward adefovir by 5.7-folds (28). Stanford University database specifies that the mutation is found in 33.3% of chronic HBV treatment naïve patients with genotype D (30).
Conclusion
Patients with HBeAg-negative profile show better virologic response than HBeAg-positive patients within the same time period. Higher concentration of HBV DNA at baseline has negative prediction for viral suppression. The A-B motif interdomain rtL122F mutation was found in nonresponder patients in our study. Another mutation rtN248H observed in E motif considered to have effect on DNA primer grip, which fors part of binding pocket.
Footnotes
Author Disclosure Statement
No competing financial interests exist.