
Abstract
Japanese encephalitis (JE) is a vector-borne viral disease with clinical manifestations ranging from asymptomatic to severe neurological symptoms and even leading to death. The exact pathophysiology for diverse clinical spectrum of the disease is complex and has not yet been defined. Studies have postulated that during JE infection, inflammatory cytokines and chemokines are produced after the initial recognition of viral antigens through the engagement of toll-like receptors (TLR) pathways. However, there is paucity of knowledge on the expression levels of chemokines and TLRs among mild and severely affected JE patients. Hence, to better understand disease pathogenesis, we examined the mRNA expression of chemokines, CCL2 and CCL5, and their respective receptors CCR2 and CCR5 along with TLRs viz. TLR3, TLR7, TLR8, and TLR9 in context of mild and severely Japanese encephalitis virus (JEV)-infected (n = 19) and healthy (n = 19) individuals. Our study showed significant downregulation of CCL2, CCL5, CCR2, CCR5, and TLR3 by log 0.87, 1.02, 0.82, 0.68, and 0.37-fold respectively, among mild cases compared with controls. Significant difference of gene expression among mild and severe JE cases for CCL2 (p < 0.001), CCL5 (p < 0.01), and TLR7 (p < 0.05) was observed. In conclusion, our results proposes that chemokines viz. CCL2 and CCL5 along with TLR7 may be associated with degree of pathogenesis of JE and could be putative therapeutic targets for preventing severe inflammation during viral encephalitis.
Introduction
J
JE-associated morbidity confers two distinct phenotypes viz. mild, where patients usually suffer from brief febrile illness, headache, and irritability; and severe, where patients suffer from encephalitis and possible death (23). The involvement of multiple factors, including host immune response may be hypothesized for differential phenotypic spectra of JE. Replicative documentation on altered homeostatsis of cytokines viz. tumor necrosis factor-alpha and interleukin-6 has been associated with JE severity in mice, but studies are extremely limited on chemokines (8). It has been shown through in vitro and in vivo experiments that JE infection activates the antiviral mechanism leading to the production of chemokines (2,10,29). However, the knowledge of chemokine response in humans as a result of natural JE infection is still inadequate. In this regard, only chemokine CCL5 protein has been explored earlier with respect to JE mortality in humans (3,27). It needs to be mentioned here that protein level is not always directly correlated with the expression of their respective genes (6). Although the functions of chemokines are intricately dependant on its corresponding receptors, no studies have explored chemokine and its coreceptor expression patterns among differential phenotypes of JE patients. Therefore, we studied the gene expression profile of chemokines viz. CCL2 and CCL5 along with their cognate receptors viz. CCR2 and CCR5.
In addition to the chemokines, toll-like receptors (TLRs), which recognize the pathogens, also have a crucial role in viral pathogenesis and form a connecting link between innate and adaptive immune response. The beneficial role of TLR signaling for viral clearance via long-term adaptive immunity has been reviewed earlier (14). Conversely, it may trigger the increased release of proinflammatory cytokines and chemokines, which may ultimately exacerbate neuroinflammation (14). One of the central features of neuroinflammation caused by infectious diseases is dysregulation of immune mediators (20). However, studies are extremely lacking on the gene expression pattern of TLRs in JE-infected patients that initiates the hierarchical cascade of cytokine and chemokine release. Therefore, we also studied the expression of TLRs viz. TLR3, TLR7, TLR8, and TLR9 that are crucial for viral nucleic acid detection. This study will help in better understanding of the host immune defence mechanism and identify plausible therapeutic possibilities.
Materials and Methods
Study subjects
The study was approved by the Institutional Ethics Committee of Regional Medical Research Centre, ICMR, India and was in accordance with the Declaration of Helsinki. Informed written consent from each participant was obtained. Blood samples were collected from 19 hospital-confirmed JE cases (mild: severe = 9:10) and from 19 healthy controls. For cases, only hospitalized patients were selected for the study, and the diagnosis of JE was considered by the presence of anti-Japanese encephalitis virus (JEV) IgM antibodies in serum and/or CSF as per WHO guidelines (26). On the basis of their clinical symptoms, JE cases were further stratified as mild (with acute fever, headache, irritability, and myalgia) and severe (with paralysis and/or encephalitis). Controls were apparently healthy individuals from JE endemic region.
Peripheral blood mononuclear cells culture
Peripheral blood mononuclear cells (PBMCs) were isolated by density gradient separation (Ficoll Histopaque-1077; Sigma-Aldrich, MO). The cells were adjusted to 106 cells/mL and cultured in RPMI1640 (HiMedia, Mumbai, India) treated with 50 IU penicillin, 50 μg/mL streptomycin, and 50 μg/mL amphotericin B (Sigma-Aldrich) and supplemented with 10% fetal bovine serum (Gibco, Thermo Fisher Scientific, MA) in six-well plate. Furthermore, cells were induced with or without 1 multiplicity of infection of JEV (locally circulating JEV strain, GenBank: HQ246155) and incubated for 12 h at 37°C in 5% CO2.
RNA extraction and gene expression assay
PBMCs were lysed by QIAzol (Qiagen, Germany) and total RNA was extracted using RNeasy Mini Kit (Qiagen, Germany) according to the manufacturer's protocol. Subsequently, 1 μg of total RNA was reverse-transcribed using QuantiTect® Reverse Transcription Kit (Qiagen, Germany). Real-time polymerase chain reaction (PCR) was performed on StepOne Plus Real-Time PCR System (Applied Biosystems, CA) using gene-specific TaqMan PCR probes for CCL2 (Hs00234140_m1) and CCL5 (Hs00982282_m1). The house keeping gene, GAPDH, was used to normalize gene expression level and served as an endogenous control. For SYBR green-based assay, the primers used are given in Table 1 (11,15).
TLR, toll-like receptor.
Statistical tests
Differences in demographic characters of mild and severe JE cases were estimated with two-tailed t-test and Fisher's exact tests. Comparison of gene expression between mild JE, severe JE, and control groups was analyzed using one-way ANOVA and Tukey's multiple comparison test. All values are represented as mean ± standard error. Statistical significance was considered at p < 0.05. All statistical tests were performed using GraphPad Prism 5.0.
Results
Demographic features
Demographic and clinical characteristics of mild and severe JE patients are shown in Table 2. Severe JE cases were adults of middle age (39.60 ± 7.99 years). The male to female ratio among mild and severe JE cases were 2:1 and 2.3:1, respectively. The total leukocyte count was significantly higher in severe JE than the mild JE cases (p = 0.04). No significant difference was observed for vaccination status and clinical parameters, including hemoglobin, blood sodium, and potassium levels among mild and severe JE cases.
Statistical significance was calculated by two-tailed t-test for continuous variable and Fisher's exact test for categorical variables.
p < 0.05.
Gene expression in mild and severe JE cases
Gene expression level of CCL2 was low in all the nine mild JE cases and was found to be ≤1-fold when compared to healthy controls. Among the severe JE cases, five of them showed higher expression levels (>1-fold) of CCL2. When the expression level of chemokine CCL5 was analyzed with controls, it was observed that seven of the nine mild JE cases had low (≤1-fold) mRNA expression. Among the severe JE cases, the CCL5 expression level was higher in four of ten cases, while two showed lower levels (≤1-fold) than the controls. For the chemokine receptor CCR2, gene expression was found to be low (≤1-fold) in six of the mild JE cases. Of note, in three of the severe JE cases, CCR2 expression was higher (>1-fold) than the controls. Similar trend was observed for chemokine receptor CCR5 mRNA expression. In mild JE cases, CCR5 gene expression was lower (≤1-fold), whereas three of the severe JE cases showed increased expression (>1-fold) when compared with controls. The gene expression in TLR3 and TLR7 was lower (≤1-fold) in all the mild JE cases compared with controls. The gene expression of TLR8 and TLR9 was lower (≤1-fold) in five and seven mild JE cases, respectively, than the controls. On the contrary, higher (>1-fold) expression of TLR3 and TLR7 was observed among four and five severe cases, respectively, compared with controls. Similarly, the gene expression in TLR8 and TLR9 was higher (>1-fold) in six and five severe JE cases, respectively, than the controls.
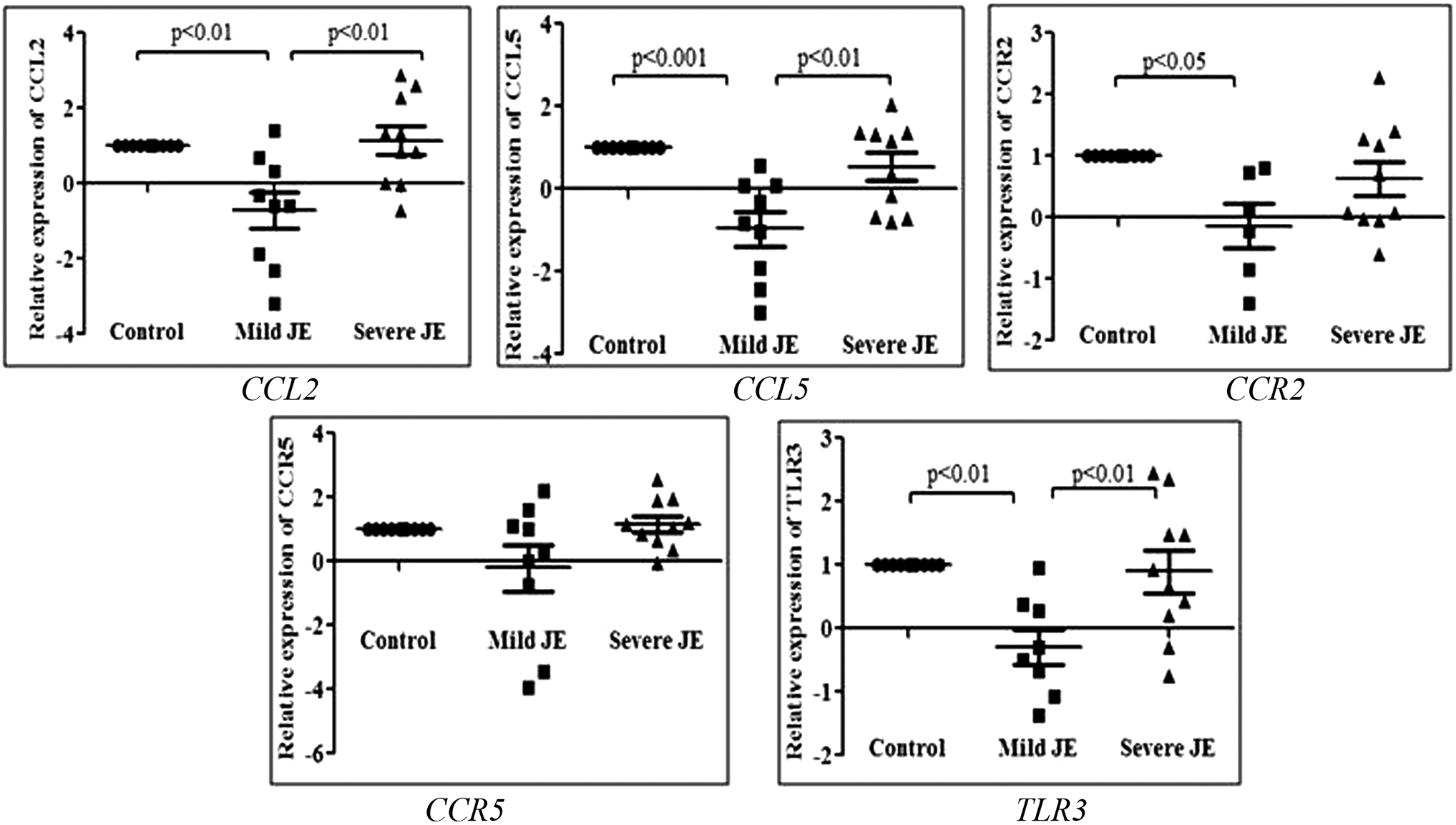
To understand the diverse intensity of gene expression values, data were normalized by log transformation, and comparison of the gene expression levels between mild and severe JE cases was performed. It was observed that gene expression of CCL2, CCL5, CCR2, and CCR5 was significantly downregulated by log 0.87, 1.02, 0.82, and 0.68-fold, respectively, among mild JE cases compared with controls (Fig. 1). In contrast, among severe JE cases, the gene expression of CCL2, CCL5, CCR2, and CCR5 was log 1.24, 0.97, 0.57, and 0.62-fold, respectively, higher than the controls. When mild cases were compared with severe JE cases, significant difference of gene expression for CCL2 (p < 0.001) and CCL5 (p < 0.01) was observed (Fig. 1). For chemokine receptors viz. CCR2 and CCR5 genes, the difference in mRNA expression level between mild and severe JE cases was not found to be significant. On analyzing the fold change pattern of TLRs, only TLR3 was significantly downregulated by 0.37-fold among mild cases compared with the controls (p < 0.05). In addition, TLR7 gene expression was significantly upregulated in severe JE cases than the mild JE cases (p < 0.05). However, no significant difference in TLR8 and TLR9 gene expression was observed between mild and severe JE cases and controls (Fig. 1). The relative gene expression level for all the studied genes between total JE cases and controls did not show any significant difference.

Gene expression pattern of chemokines (CCL2 and CCL5), their coreceptors (CCR2 and CCR5), and TLRs (TLR3, TLR7, TLR8, and TLR9) among mild and severe JE cases compared with controls. Data are represented as mean ± SEM. JE, Japanese encephalitis; SEM, standard error of the mean; TLRs, toll-like receptors.
As the expressions of genes viz. CCL2, CCL5, CCR2, CCR5, and TLR3 were significantly downregulated in mild JE cases, we further designed an ex vivo experiment by stimulating the PBMCs of the studied groups with JEV to validate our observation. On stimulation with JEV, our study revealed significant downregulation of CCL2 (p < 0.01), CCL5 (p < 0.01), and CCR2 (p < 0.05) among mild cases compared with the controls (Fig. 2). Similar pattern of gene expression was also observed for TLR3 gene upon JEV stimulation where significant difference was observed between mild JE cases and controls (p < 0.01). Significant difference was also observed between mild and severe JE cases for CCL2 (p < 0.01), CCL5 (p < 0.01), and TLR3 (p < 0.01) post-JEV stimulation.
Gene expression pattern of chemokines (CCL2 and CCL5), their coreceptors (CCR2 and CCR5), and TLR3 among mild and severe JE cases compared with controls after JEV stimulation. Data are represented as mean ± SEM. JEV, Japanese encephalitis virus; SEM, standard error of mean.
Discussion
The unavailability of antiviral therapy for JE till date calls for new therapeutic options. The aggravation of central nervous system (CNS) inflammation during JE severity also poses as a serious challenge. It is extremely crucial to know the molecular mechanism of the disease pathogenesis as well as host immune response for development of an intervention strategy for JE treatment. Although high chemokine levels during infection are implicit, there is paucity of substantive studies of gene expression levels for the differential pathogenesis of JE in humans. Therefore, in this pilot study, we evaluated the expression levels of inflammatory chemokines (CCL2 and CCL5), their coreceptors (CCR2 and CCR5) along with the upstream signaling TLRs (TLR3, TLR7, TLR8, and TLR9) in PBMCs of mild and severe JEV-infected individuals along with healthy controls.
During the mRNA expression study, CCL2 and CCL5 were found to be significantly upregulated among severe JE cases than the mild JE cases, which suggests a profound inflammatory response in the former. Chemokines viz. CCL2 and CCL5, which are involved in leukocyte trafficking, are key mediators of cellular immunity and antiviral host defence. Quite a few in vitro and in vivo studies have repeatedly underlined the importance of these chemokines during flaviviral infection, including JE (29), dengue (9), and West Nile (16). A previous study showed increased expression of CCL2 and CCL5 genes during acute phase of JE infection in mice (10). Another study demonstrated significant upregulation of CCL2 and CXCL10 mRNA in JEV-infected mice brain (29). These mice model studies are in compliance with our findings and may crucially suggest the importance of chemokines in the adverse prognosis of the disease. The chemokines may exacerbate the penetration of inflammatory cells and thereby, increase blood–brain permeability (4). It is to be noted that the severe JE cases presented an increased leukocyte count which is the classical manifestation of inflammation. In this context, it is important to mention that the extent of chemokine gene expression during JE infection may be dependent on disease severity and the pathogenicity of the virus as seen during other flaviviral infection (16,21).
Although chemokines are secreted in response to host protection, altered homeostasis of cellular microenvironment with the aid of chemokines and cytokines, seems crucial for progression of neuroinflammation upon flavivirus infection, including JE (24). Our study revealed that mRNA expression of the chemokine and chemokine coreceptor genes was significantly downregulated in mild JE cases. It may be hypothesized that these genes have a protective role during the initial phase of infection, but at a later stage may contribute to the adverse pathogenesis of the disease. This may be validated from similar trend of gene expression post-JEV stimulation as seen in our ex vivo experiment.
In an effort to identify the alterations in the innate immune signaling pathways that mediate chemokine production in mild and severe JEV-infected individuals, we investigated the expression pattern of the TLR genes involved in viral nucleic acid recognition. We found significantly elevated TLR7 gene expression (p < 0.05) among severe JE cases than the mild JE cases, which may indicate its importance in innate immune response against JE pathogenesis. Our findings are somewhat similar to an earlier study where differential TLR7 expression was observed between JEV-infected and uninfected human brain samples (19). A study also reported upregulation of TLR7 levels in JEV-infected BALB mice and mouse neuronal cells when compared with controls (10). The crucial involvement of TLR7 in innate immunity during other flaviviral infection has also been demonstrated earlier using knock down mice. Studies revealed that TLR7 knock down mice exhibited increased viral load and mortality when compared with control mice (25). Moreover, dysregulation of TLR7 was shown to affect the downstream T cell response in West Nile virus-infected mice (28). A previous study showed increased TLR7 expression in severely affected dengue children, which is comparable to our present findings (5). Thus, it may be hypothesized that inflammation during JE severity may be mediated by the induction of TLR7. High induction and upregulation of TLR7 as observed in severe JE cases, may suggest the activation of NFkB pathway (7). During JEV stimulation, differential TLR3 gene expression was observed among mild and severe JE cases. Our study corresponds to previous in vivo and in vitro studies that demonstrated the importance of TLR3 and its associated chemokine response during JE progression (12,13). Therefore, owing to the potential role of inflammation in inducing immunopathology, it is crucial that the expression of these immune molecules is tightly regulated so as to limit the magnitude and duration of response.
The sample size used for this study represents only a small subset of the JEV-infected individuals. Nevertheless, significant results of the present study necessitate further longitudinal studies on chemokines and its association with JE. Our study used PBMC cultures that include T cells, NK cells, and monocytes and are essential for antiviral mechanism. Monocytes from PBMC differentiate into macrophages and are suggested to play a significant role in JEV-induced neuronal damage (18). Moreover, chemokines are known to aid the polarization and trafficking of macrophages during infection (22). In conclusion, our results showed the upregulation of CCL2, CCL5, and TLR7 among severe JE than the mild JE patients, suggesting that chemokine-dependent migration and infiltration of monocytes/macrophages may be involved in encephalitis-related complication or adverse prognosis. Most importantly, our findings suggest the involvement of chemokines and TLR in regulation of the degree of pathogenicity in JE-infected patients. Thus, this study may further decipher the complex immune mechanism of JE pathogenesis and will help in developing new strategies against JE-related severe inflammation.
Footnotes
Acknowledgments
The authors thank the Director and the Arbovirology and Rickettsiology group of Regional Medical Research Centre (Indian Council of Medical Research), NE Region, India. The study's financial support was provided at Regional Medical Research Centre, NE Region, India, and supported by ICMR, New Delhi, India.
Author Disclosure Statement
No competing financial interests exist.