
Abstract
Limited data on varicella zoster virus (VZV) vaccine responses are available in HIV-positive adults, especially among those with end-stage renal disease on dialysis or undergoing kidney transplantation (KT). Serological and T cell responses were analyzed using anti-VZV IgG titers, enzyme-linked immunosorbent assay and flow cytometric intracellular cytokine staining (ICS) in two HIV-positive kidney transplant candidates undergoing dialysis and receiving VZV immunization. The results were compared with two HIV-positive and two HIV-negative VZV-seropositive patients (two kidney transplant candidates and two kidney transplant recipients), and with one HIV-negative vaccinee. HIV-positive VZV-susceptible patients received two doses of VZV vaccine 12 weeks apart. No adverse events were reported. Serological data were indicative of immunological response in one patient and corresponded to T cell responses. The second patient showed only a transient increase in anti-VZV IgG titers, but reported positive CD4+ T cell responses that were maintained after KT. Positive T cell and serological responses were detected in both HIV-positive and HIV-negative controls. VZV vaccination appeared safe and effective in HIV-positive KT candidates. VZV-specific T cell immunity was detected among transplant candidates and after KT. The assessment of VZV-specific T cell immunity using flow cytometric ICS may be more reliable compared to serology in assessing responses to VZV vaccine in this group.
Background
Varicella zoster virus (VZV) infection represents a life-threatening disease in immunocompromised patients due to potential visceral complications (20,26). Although virus-specific cellular immunity is considered critical to control viral replication (1), open questions remain on the immunogenicity of the vaccine in immunocompromised hosts (23). In HIV-infected children, VZV immunization showed satisfactory responses, also among subjects with impaired immunity (e.g., CD4+ T cell >15%, absolute count >200 cells/mm3) (14). Currently, two doses of VZV vaccine 12 weeks apart are suggested in stable HIV-positive patients with CD4 count of at least 200 cells/mm3 (22). Susceptible dialysis patients, especially if kidney transplantation (KT) is being considered, should receive VZV vaccination due to the high risk of severe posttransplant disease (3,6). Limited data on VZV vaccine responses over time, however, are available in HIV-positive adults undergoing dialysis or KT.
Objectives
Anti-VZV IgG titers and antigen-specific T cell responses to VZV immunization were analyzed in two HIV-positive KT candidates using enzyme-linked immunosorbent assay (ELISA) and flow cytometric intracellular cytokine staining (ICS) assay. The results were compared with HIV-positive and HIV-negative VZV-seropositive patients (including two kidney transplant candidates and two kidney transplant recipients), and with one HIV-negative vaccinee.
Study design
HIV-positive, VZV-seronegative patients received two doses of live attenuated Oka vaccine (Varivax®, MSD, Italy) 12 weeks apart. Immune responses were analyzed 6 weeks after the first and second dose, 6 months after immunization, and following KT in one patient. Blood was obtained after approval of the local Institutional Ethical Committee, and informed consent was collected from all study participants.
Serological tests were performed using the fully automated Liaison VZV IgG immunoassay (DiaSorin, Vercelli, Italy), based on chemiluminescence technology using partially purified extract of infected cell cultures and calibrated against WHO international preparation (W1044) (15). This assay is routinely used at our institution for assessment of VZV immunity and has shown optimal sensitivity (>97%) and specificity (100%) compared to other commonly used tests in clinical practice (2,19).
The cell-ELISA method has been previously described and was used to quantitate peripheral blood mononuclear cell (PBMC) INF-γ production (16,17). IFN-γ antibody pairs and ELISA kit were obtained from Biolegend (San Diego, CA). Results are shown as the optical density at 405 nm as picograms/milliliter (pg/mL) of cytokine, according to a standard titration curve. Phosphate-buffered saline and RPMI 1640 medium were purchased from BioWhittaker (Verviers, Belgium). RPMI 1640 medium was enriched with 10 mM L-glutamine and 5% fetal calf serum (FCS) to obtain complete medium. Antibodies for phenotyping and intracellular cytokine staining (ICS) were from Becton Dickinson (BD, San Jose', CA). VZV-infected cell lysate (VZV antigen) was purchased from Microbix (Toronto, Canada) and used as a stimulant. Other antigens included Candida albicans (Microbix) and the mitogen phytohemagglutinin (PHA) (Sigma-Aldrich, Milan, Italy). Final antigen concentration was 1 μg/mL.
Flow cytometry analysis (BD Biosciences FACSCantoII™) and ICS (Cytofix-Cytoperm, BD) were used to assess T cell subpopulations (CD3+CD4+ T-helper cells and CD3+CD8+ effector T cells), and cytokine production (interferon-γ, INF-γ) from nonstimulated (NS, incubated with medium), VZV-stimulated cells, or PBMCs stimulated with phorbol myristate acetate and ionomycin (PMA/IONO) (Sigma-Aldrich) serving as positive control antigen. For ICS, PBMCs (106 PBMCs/well) were incubated for 18 h with T cell medium, costimulatory antibodies (αCD28 and αCD3; BD), and antigens (VZV and PMA/IONO). Brefeldin-A (BD Pharmingen) was added for the final 5 h. Cells were permeabilized using the BD-FACS intracellular cytokine staining kit according to the manufacturer's instructions and stained for αCD3-FITC, αCD4–PECy7, and αIFN-γ-PE. CD3+CD4+ and CD3+CD8+ lymphocytes were assessed for IFN-γ production. IFN-γ + T cells were designated as VZV-specific CD4+ and CD8+ T cells. Data collected on the flow cytometer were compensated and analyzed with FlowJo (Treestar, Ashland, OR).
Results
We have analyzed cell-mediated responses to VZV antigens in four HIV-positive patients, including three KT candidates and one recipient, two HIV-negative VZV-seropositive patients (a kidney transplant candidate and one transplant recipient), and one HIV-negative vaccinee. Patients' characteristics are summarized in Table 1. All four HIV-positive patients were stable and receiving antiretroviral therapy. VZV-seropositive HIV-positive and HIV-negative patients reported a history of prior varicella infection. Two patients (Patient 1 and 2) with no previous history of VZV disease or immunization were found seronegative for VZV during routine pretransplant screening and received two doses of VZV vaccine. Patient 1 underwent KT 8 months after vaccination, while Patient 2 remained on the kidney transplant waiting list. No complications were detected after vaccine administration in both vaccinees, and VZVDNA measurements in blood were persistently negative. Table 2 reports IFN-γ production from PBMCs by cell-ELISA. Positive responses to Candida spp. (ranging from 74 to 244 pg/mL) and PHA (positive control) were registered in all subjects. Patient 1 had no detectable IFN-γ production (except for a slight transient increase after the first dose of VZV vaccine), while Patient 2 showed persistent response after the second dose of vaccine. Patients 3 and 4 (HIV-positive controls) and Patients 5 and 6 (HIV-negative controls) showed IFN-γ production to VZV antigen stimulation. The healthy control received two doses of VZV vaccine due to persistent VZV seronegativity. Assessment of cell-mediated immunity showed positivity after the first and second dose of VZV vaccine and weak, but positive response at the 6-month follow-up. Figure 1 reports VZV-specific cell-mediated immunity assessed by cell-ELISA compared with serological responses, showing substantial correspondence between the two tests. In particular, Patient 1 had only a transient increase of VZV IgG, while Patient 2 showed seroconversion after the second dose of VZV vaccine.
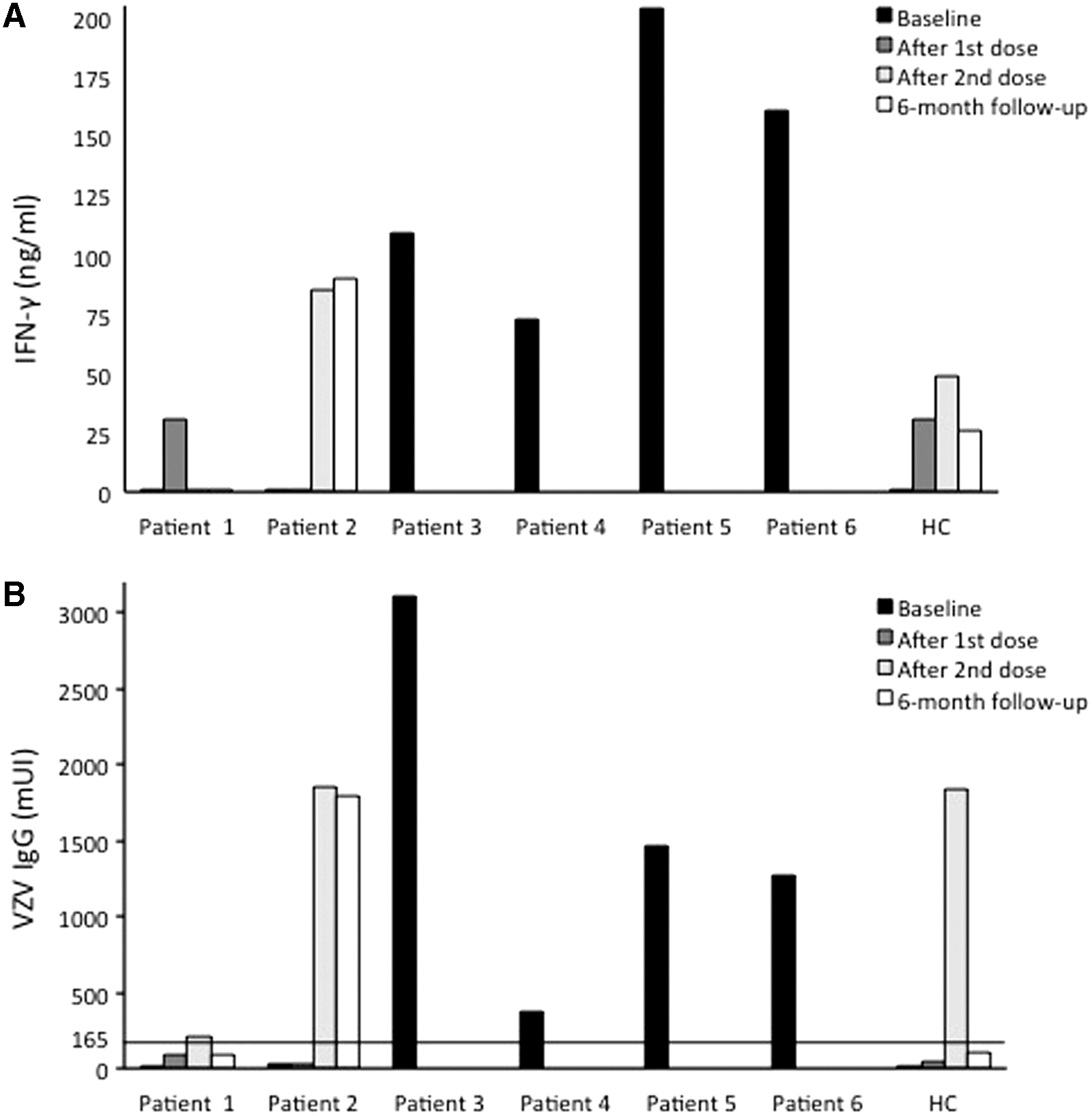
Comparison of immune responses measured by PBMC IFN-γ production by cell-ELISA and serological responses (IgG positivity) in HIV-positive patients and controls.
Characteristics of Patients Included in the Study
All patients were stable and receiving antiretroviral treatment.
At the time of the first VZV vaccine dose for immunized patients.
KT, kidney transplantation; HC, healthy control; UN, undetectable HIV viral load; VZV, varicella zoster virus.
Cellular Immune Response Assessed Through Cell-ELISA Measuring IFN-γ Production After Peripheral Blood Mononuclear Cell Stimulation with VZV and Candida spp. Antigens and Phytohemagglutinin (PHA, Mitogen)
Results were confirmed negative 5 months after kidney transplantation.
PHA, phytohemagglutinin.
VZV-specific CD4+ and CD8+ T cellular immunity were measured by ICS (Table 3). Patient 1, who did not show response to VZV vaccination at serological and cell-ELISA tests, showed a higher percentage of CD3+CD4+IFN-γ + in VZV-stimulated compared to nonstimulated cells after the second dose of VZV vaccine, at the 6-month follow-up and 5 months after KT (Fig. 2A). Figure 2B and C show that VZV-specific CD4+ T cell response was also documented among HIV-positive and HIV-negative kidney transplant recipients (Patient 4, Fig. 2B, and Patient 6, Fig. 2C). Similarly reactivity to PMA/IONO (positive control) was reported.
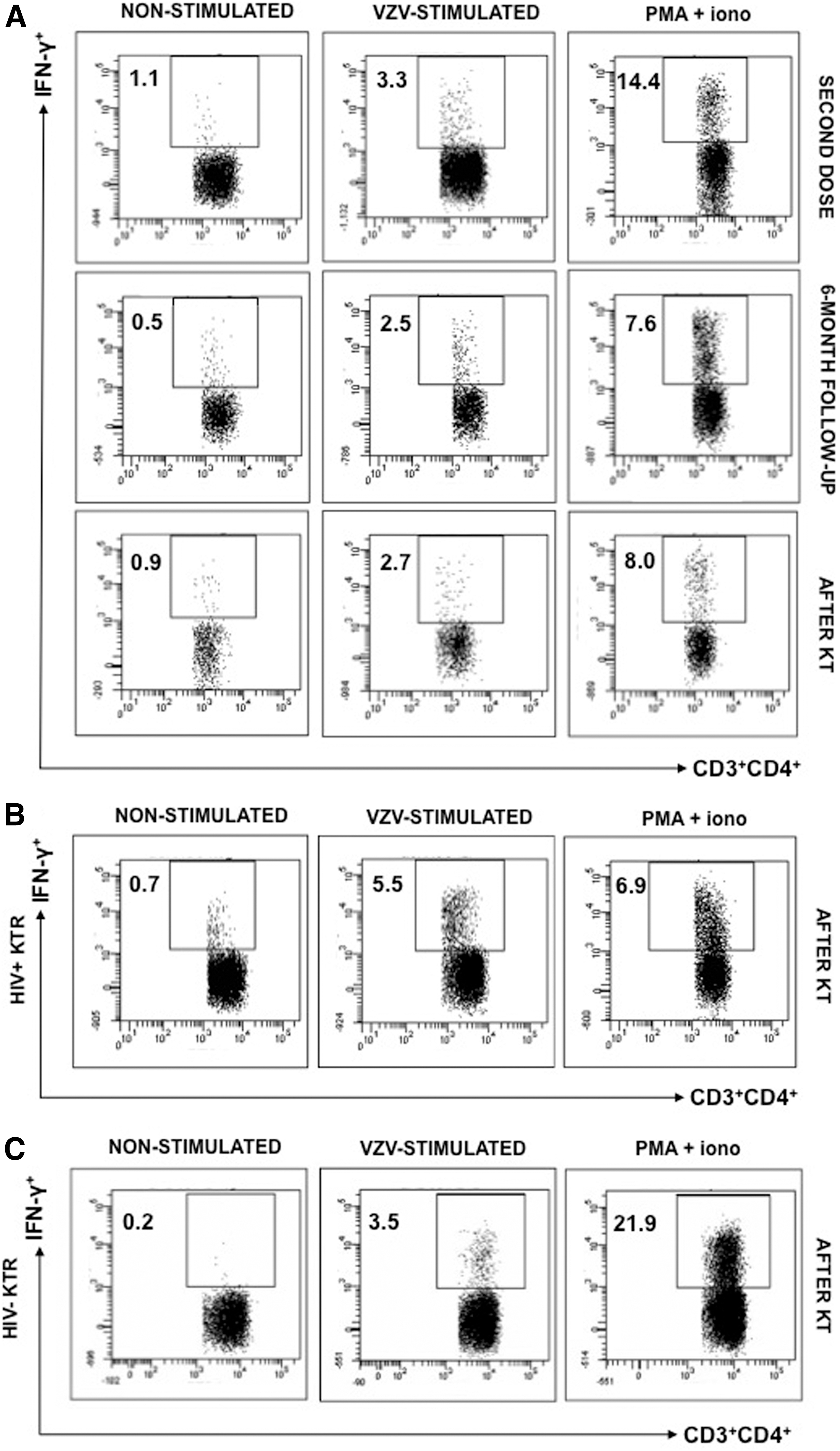
Representative dot plots showing the frequency of IFN-γ positive events in CD3+CD4+ T cells by intracellular cytokine staining in kidney transplant patients. Patient 1 (HIV-positive kidney transplant recipient vaccinee) postvaccine samples
VZV-Specific CD4+ and CD8+ T Cell Immune Response Assessed Through Flow Cytometry Measuring IFN-γ Production After Peripheral Blood Mononuclear Cell Stimulation with VZV Antigens and Phytohemagglutinin (PHA, Mitogen)
Measured after the second dose of VZV vaccine.
Table 3 shows that VZV-specific CD4+ and CD8+ T cell responses were reported by HIV-positive and HIV-negative controls. Although VZV-specific CD8+ T cell immunity was detected in Patient 1 and 2, net responses were lower compared with CD4+ T cell responses.
The healthy vaccinee displayed VZV-specific T cell responses after vaccination with reduction of IFN-γ production over time, especially for CD8+ T cells (Table 3).
Discussion
The widespread introduction of VZV vaccination has disclosed the presence of nonresponders or the loss of humoral immunity, even among healthy subjects (21). These conditions can be challenging for clinicians facing the potential threat of VZV susceptibility in high-risk subjects. In this context, the reliability of VZV serological response has been questioned (7). Although a positive IgG titer remains the “gold standard” for assessing VZV protection, VZV antibodies represent only a surrogate of the correlate of protection (7). Immunological studies report that while VZV antibodies can fade after vaccination, VZV-specific CD4+ cell response is a more reliable correlate of protection (13,18). Data supporting this hypothesis, however, are limited. A case report analyzing T cell responses in a vaccinated subject with undetectable VZV antibodies after serological reconversion showed persistently positive CD4-mediated immunity (18). In another report, a healthy subject with absence of VZV antibody titer after three doses of vaccine showed positive cellular responses measured by ICS and, despite documented contacts with infectious subjects, did not develop VZV disease (2). In our study, we observed persistent VZV-specific CD4+ T cell responses in an HIV-positive KT recipient vaccinee with only transient serological responses and CD4 count >500 cells/mm3. Other reports highlight that CD4 count and HIV-RNA may not be critical in predicting VZV-specific immunity (2,25). In our study, we detected preserved cellular immunity toward other antigens (e.g., Candida spp. and mitogens) that did not correlate with patients' CD4 cell count. A study involving 67 HIV-positive subjects with T CD4 ≥ 400 cells/mm3 demonstrated that the vaccine was safe, but only modestly immunogenic for HIV-positive subjects compared to HIV-negative vaccinees using lymphocyte proliferation assays and IFN-γ ELISPOT (26).
A factor that may explain the variability in the immunological results to VZV vaccination is the different sensitivity shown not only by commercial serological VZV tests (9,21) but also across cellular immunity assays (4). Cell-ELISA has previously demonstrated to be a reliable test for assessing antigen responses in HIV-positive patients (16,17), although VZV responses were not specifically investigated. A previous report analyzing VZV-specific T cell responses after zoster vaccination found comparable data using ELISPOT and ICS (12). The flow cytometric ICS assay, in particular, is one of the primary tests for the analysis of vaccine-induced T cells in clinical trials (8). ICS has demonstrated to be useful in measuring antigen-specific responses in HIV-positive subjects, potentially explaining Patient 1 positivity compared to cell-ELISA (3). We also observed that antigen-specific (VZV, Candida, and mitogen related) T cell responses remained preserved among HIV-positive patients after KT and were comparable with those detected in the HIV-negative kidney transplant recipient. Despite VZV-specific CD4+ T cell immunity being detected in the HIV-positive kidney transplant vaccinee, we opted to maintain the patient on VZV prophylaxis with valaciclovir due to the profound immunosuppression associated with the early posttransplant period.
Our study has several limitations. First, IgG titers were assessed using a fully automated system instead of other reference tests assessing glycoprotein-specific antibodies (e.g., fluorescent-antibody to-membrane-antigen test, FAMA) or neutralizing antibodies (10,11) that are not used in clinical practice due to the increased complexity and subjectivity in the interpretation of the results. Similar to other reference tests, however, the automated chemiluminescence assay has shown high sensitivity and specificity in detecting protection against clinical varicella (2,19). Second, VZV lysates were chosen as stimulating antigens instead of selected peptide pools. Although VZV lysates have been successful in determining T cell responses through ICC (24), their use may have limited the detection of VZV-specific CD8+ responses compared to CD4+ T cell responses (5). Finally, our results need to be validated in a larger number of vaccinated subjects and at different time points after KT. Nevertheless, the restricted number of adult subjects on dialysis or transplant waiting list requiring VZV immunization represents an intrinsic limitation for these types of studies.
In conclusion, VZV vaccination appeared safe and effective in HIV-positive KT candidates. In one patient, serological and cellular immune responses to VZV appeared suboptimal, although persistent VZV-specific CD4+ T cell responses were detected using ICS and confirmed among transplanted and nontransplanted controls.
Our report highlights the importance of investigating cell-mediated immune responses to VZV vaccination in specific patient populations. While VZV-specific T cells are known to be essential to prevent VZV disease, valid options to avoid life-threatening infections in patients with impaired cellular immunity are limited. Further data on the utility and the most reliable methods to assess VZV-specific immunity, especially among patients with absent serological response and in the clinical setting of HIV infection, are needed to help identify populations for whom interventions, such as VZV prophylaxis, may be beneficial.
Footnotes
Author Disclosure Statement
The authors have no conflict of interests.