
Abstract
As the main effector cells of innate immunity, nature killer (NK) cells play important roles in preventing hepatitis B virus (HBV) infection. This study aims to investigate the correlation between NK cells and different clinical stages of chronic HBV infection and interferon-α (IFN-α) therapy. Two hundred ninety-five patients diagnosed with chronic hepatitis B (CHB) infection and selected 50 healthy adults were enrolled in this study, the frequency of CD3−CD56+ cells in peripheral blood were measured and analyzed. The level of NK cells was decreased in hepatitis B-associated liver cirrhosis significantly and had no changes in CHB or hepatocellular carcinoma, while the frequency of NK cells gradually decreased from the baseline to week 24 and then increased since week 24–48 in CHB with IFN-α treatment. NK cells played an important role in the process of HBV progression and IFN-α therapy.
Introduction
Hepatitis B virus (HBV) infection is a global disease that seriously affects human health. China has high incidence of HBV infection, it is conservatively estimated that there are more than 250 million people chronically infected with HBV, and these carriers are at high risk of hepatitis B-associated liver cirrhosis (HBV-LC) and hepatocellular carcinoma (HBV-HCC) (7).
The only effective method to block the progression of the disease is antiviral therapy, interferon-α (IFN-α) is one of approved antiviral therapies, it acts by activating nature killer (NK) cells and NK T cells and enhancing the innate immune response to achieve viral clearance (1,2,4). NK cells plays a key role in defense against HBV infection by killing infected cells or by producing cytokines such as IFN-γ, TNF-α, TGF-β, and IL-10 and interacting with adaptive immune system's cells (13). In acute hepatitis B, the innate immune mainly caused by NK cells would detect viral infection and then lead the adaptive immune response to clear HBV. But to chronic hepatitis B (CHB), both weakly innate and adaptive immune responses caused to eradicate HBV difficultly. Although IFN-α has been widely used for both anti-HBV and immunoregulation dual functions to treat CHB in past decade, it is still far from achieving sero-clearance of HBV surface antigen, the molecular mechanisms determining the efficacy of IFN-α is still poorly defined.
As dysfunctional innate and adaptive immune responses are the characteristic of chronic HBV infection, and few studies have investigated the status of innate immune system during IFN-α treatment of chronic HBV infection, the precise mechanisms underlying immune cell regulation are not fully understood (3,11).
To further explore the change of immune system in chronic HBV-infected patients and the dynamic correlation between NK cells and antiviral efficacy of IFN-α treatment, we designed the following study.
Materials and Methods
Patients
Two hundred ninety-five patients with chronic HBV infection (HBV group), median age was 47.5 ± 13.7 years (range: 21–73 years) with 205 men (69.5%) and 90 women (30.5%), including 178 patients of CHB group, 76 patients of HBV-LC group, and 41 patients of hepatitis B-associated HBV-HCC group were enrolled in this study. The diagnosis was based on the guidelines for CHB diagnosis of the American Association for the Study of Liver Diseases (AASLD) (9). Fifty healthy individuals were enrolled as normal controls (Control group) shown as Table 1. Fifty CHB were positive for serum HBsAg for >24 weeks and had elevated serum HBV-DNA of >20,000 IU/mL and alanine aminotransferase (ALT) between 80 and 400 U/L (2–10 ULN) were selected to accept interferon-α-1b (recombinant human interferon-α-1b for injection, CHN; Shenzhen Kexing Biotech Co., Shenzhen, China) 5 MIU every other day (IFN group). The observation lasted for 48 weeks. All subjects accepted physical examination and serum analysis at week 0, 12, 24, and 48.
Baseline Characteristics of Patients and Healthy Individuals
p < 0.01.
CHB, chronic hepatitis B; HBV, hepatitis B virus; HBV-LC, hepatitis B-associated liver cirrhosis, HCC, hepatocellular carcinoma; NK, natural killer.
The exclusion criteria included the following: (i) used antiviral or immunomodulating treatment in the past 6 months, (ii) positive pregnancy test in female, (iii) alcoholic liver disease, (iv) subjects with bacterial infections (v) with hepatitis C virus, hepatitis D virus, or human immunodeficiency virus co-infection, (vi) accompaniment of diabetes, thyroid dysfunction, autoimmune diseases, and psychological issues were excluded from the study. The study protocol was approved and monitored by the Ethics Committee of Nanjing Jiangbei Peoples' Hospital, and written informed consent was obtained from the patients.
Methods
Peripheral blood samples (5 mL) were taken from all the subjects. The level of NK cells expression was detected by flow cytometry (Beckman), Olympus Au640 automatic biochemical analyzer was used to detect liver function, and HBV-DNA was tested by Real-time PCR (Beijing Kean Company).
Statistical analysis
Results were reported as mean ± standard deviation. Statistical comparisons between two groups used independent samples t-test. The one-way ANOVA and Scheff method were used for multiple comparisons. Spearman correlation analysis was used to evaluate relationships between two variables. Data analysis was done by using SPSS version 13.0 for Windows (SPSS, Inc., Chicago, IL). Confidence interval was 95%.
Results
Baseline characteristics of HBV patient cohort
The average age of HBV group was significantly higher than control (39.2 ± 12.3 vs. 47.5 ± 13.7, p = 0.001) (Table 1), but there was no difference between control and CHB (39.2 ± 12.3 vs. 41.4 ± 11.9, p = 0.885) (Table 1). We attributed this result to the age of onset was delayed in the HBV-LC and HBV-HCC.
In IFN group, 1 (2%) patient discontinued treatment due to intolerance and 4 (8%) patients had no response at week 12 and then changed to use nucleos(t)ide analogs (NAs) therapy. Forty-five (90%) patients completed the full course of therapy and obtained the virological response without hepatitis B surface antigen negative.
The level of NK cells was decreased significantly in HBV and subgroup
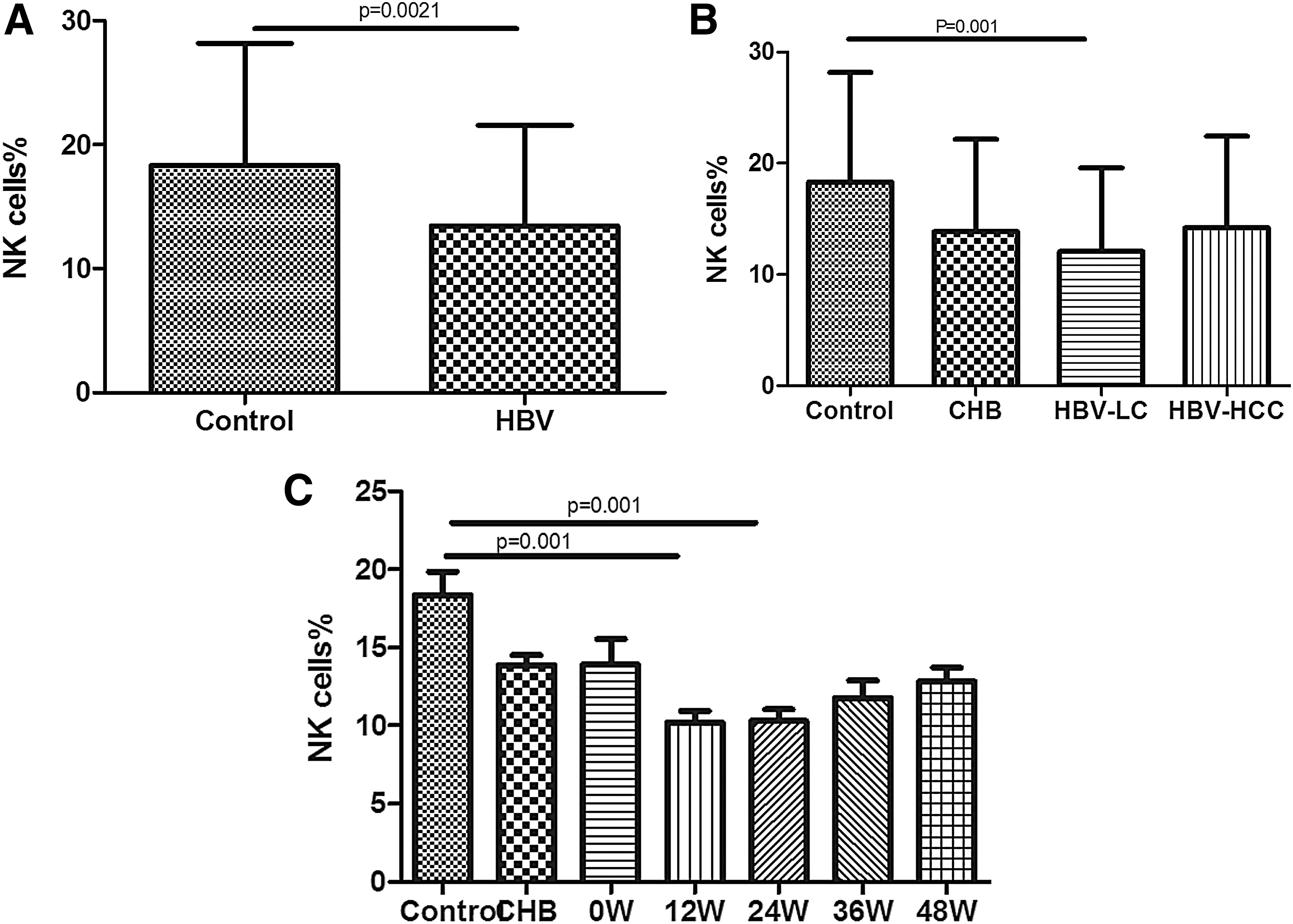
We defined the level of NK cells as the population of CD3−CD56+ cells taken the percentage of total leukocyte cells (Fig. 1A). Result showed that the level of NK cells was significantly lower in HBV than control (13.4 ± 8.1 vs. 17.6 ± 8.6, p = 0.002) (Table 1) and a representative image from each group is shown in Figure 2A. It means that the innate immune response against chronic HBV infection was suppressed.

The expression of NK cells in HBV and during IFN-α treatment. NK cells were significantly decreased in HBV-LC patients
The level of NK cells in HBV and during IFN-α treatment. The level of NK cells was significantly lower in HBV than control
Further subgroup analysis showed that, compared with control, NK cells expression was significantly lower in HBV-LC group (12.1 ± 7.5 vs.17.6 ± 8.6, p = 0.001) (Table 1) and an example image for each group is displayed in Figures 1A and 2B. Results showed that NK cells were inhibited more seriously in HBV-LC.
NK cells fluctuated during IFN-α treatment
We longitudinally studied the dynamic changes in the level of NK cells at the time points in 0, 12, 24, 36, and 48 weeks to assess the effect of IFN-α treatment, then found that the frequency of NK cells gradually decreased from the baseline to week 24 and then increased since week 24–48 (Table 2) and typical image from each group is offered in Figures 1B and 2C.
Nature Killer Cells Fluctuated During IFN-α Treatment
p < 0.01.
IFN, interferon.
The relationship between NK cells and liver inflammation indicators
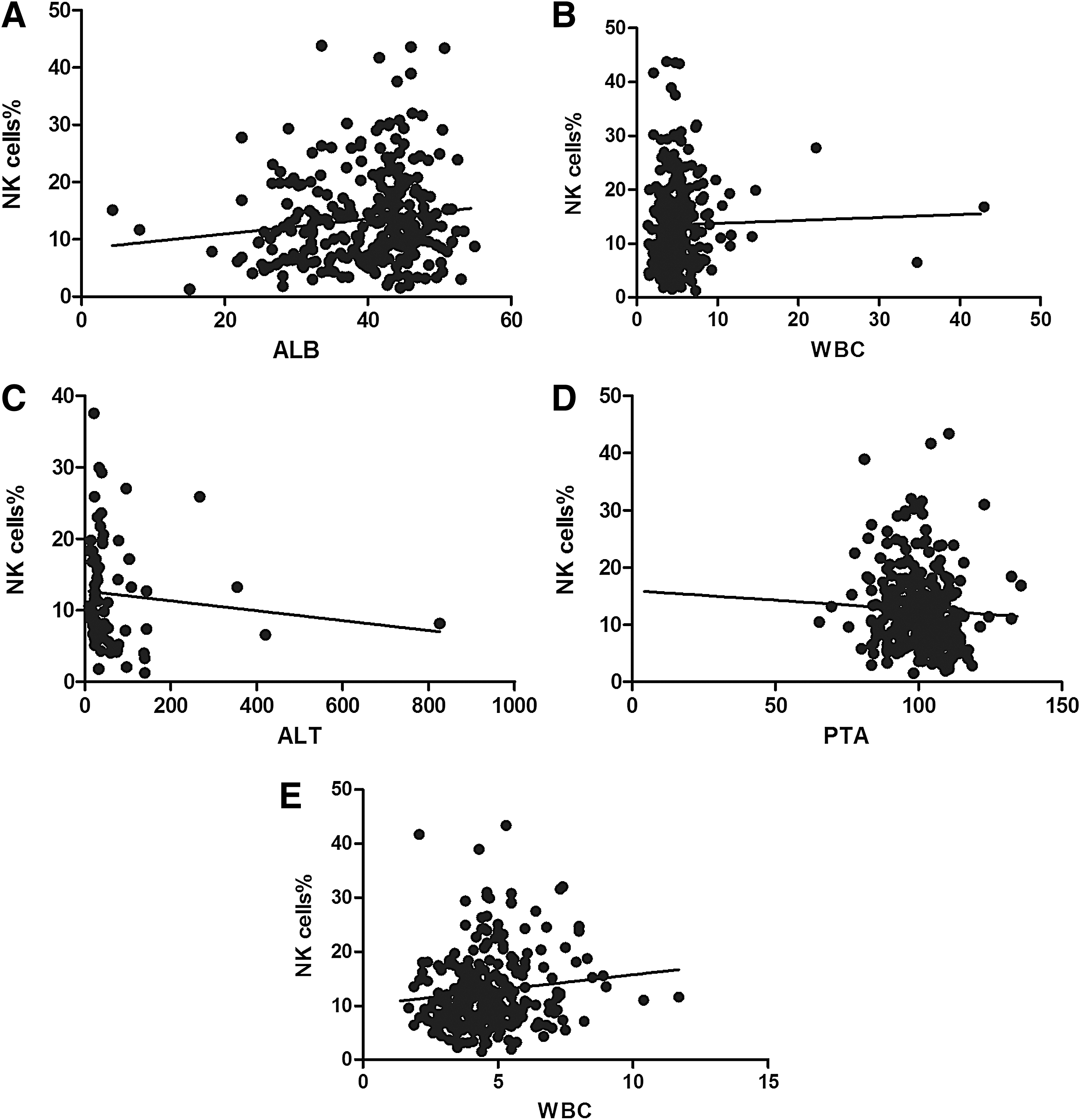
We selected ALT, total bilirubin, albumin (ALB), prothrombin time activity percentage (PTA), white blood cell (WBC), and HBV-DNA as the biochemical indicators of liver inflammation, and used spearman correlation analysis to evaluate relationships between liver inflammation and NK cells. Results revealed that there were significant correlations between NK cells and ALB (r = 0.131; p = 0.025; Table 3 and Fig. 3A), WBC (r = 0.119; p = 0.042; Table 2 and Fig. 3B) in HBV group, the study also showed a direct link between NK cells and ALT (r = −0.286; p = 0.012; Table 3 and Fig. 3C) in HBV-LC group, and there was no significant relationship between NK cells and liver inflammation indicators in CHB or HBV-HCC groups. HBV-DNA had no relationship with the expression of NK cells in HBV group or subgroup.
The relationship between NK cells and liver inflammation indicators. There were significant correlations between NK cells and ALB
Results of Spearman Correlation Analysis for Nature Killer Cells to Liver Inflammation Indicators
p < 0.05.
ALB, albumin; ALT, alanine aminotransferase; PTA, prothrombin time activity percentage; SD, standard deviation; TB, total bilirubin; WBC, white blood cell.
Through IFN-α treatment, the relationships between liver inflammation indicators and NK cells were changed, those main in PTA (r = −0.119; p = 0.048; Table 3 and Fig. 3D) and WBC (r = 0.152; p = 0.011; Table 3 and Fig. 3E).
Discussion
After HBV infection, the antigen structures in liver cell were changed, immune systems that included humoral and cellular immunity were sensitized, which enhanced the function of immune cells and led to removal of HBV. At the same time, the responses also attacked the liver cells with surface of the HBV antigen, which was the most important reason for liver injury (10,14). As long as HBV made the immune system stability disorder, autoimmune injury caused by cellular immunity loss control and humoral immunity hyperactivity would induce liver cell necrosis, destroy the normal structure of liver cells, decrease liver metabolism, fibroblast proliferation, and synthesis of collagen fibers that led to the gradual progression of liver fibrosis to liver cirrhosis, even liver cancer in the end.
Similar to previous research (3,8), our study revealed that the expression of NK cells was not more active in CHB patients, suggesting that there was no significant upregulation of innate immune function in the course of HBV infection, the result may be related to incomplete immune clearance and the cause of recurrent abnormal liver function. The percentages of peripheral NK cells were reduced significantly in HBV-LC patients compared with other subjects. One study analyzed the expression of NK cell receptors in HBV-LC patients, found that the expressions of activation receptors (NKp44, NKp46, and NKG2D) and activation markers (TRAIL, HLA-DR, CD38, and CD69) were elevated, the expression of inhibitory receptors (CD158a and CD158b) was decreased (15), the results maybe relationship with more active immune system abormalities in HBV-LC.
One aim of our study was to monitor longitudinally the impact of the treatment with IFN-α. We speculated that IFN-α could increase the innate immunity by activating NK cells, so as to achieve the goal of eliminating HBV virus and reducing liver inflammation. Our findings showed that NK cells were not upregulated significantly in CHB, with the treatment course of IFN-α, HBV-DNA was inhibited, liver function returned to normal, while NK cells showed a process of decreasing first and then rising. That was not exactly consistent with previous research conclusions.
We analyzed this expression as follows: first, after HBV infection, the innate immune system should be activated and NK cells eliminate HBV as the main effector cells, but in CHB, the level of NK cells was not increased significantly prompting the existence of abnormal function of innate immune system that caused the failure to remove HBV completely, which may be one of the mechanisms of liver cirrhosis. Second, multiple studies had shown that HBV antigens could impair NK cell's function, several mechanisms such as by activing inhibits plasmacytoid dendritic cell function, modulating the balance of activity and inhibitory receptors on the cell surface, existing in the immunosuppressive cytokine environment with high levels of IL-10, rising HBV-induced NK-reg cells were involved in (6,12,16,17). The final result of all reactions was that NK cell expression did not increase in CHB. NK cells as the main effector cells to defend HBV infection were abundant in the normal liver (4), during IFN-α treatment, NK cells in peripheral blood maybe enriched into liver at first, then with the levels of HBV-DNA and serum HBV surface antigen (HBsAg) decreased, the expression of NK cells in peripheral blood rose again, as in the result of Lee et al.'s study (5).
Now, we report here that NK cells played an important role in the clinical course of CHB. IFN-α therapy could improve the innate immunity disorder by regulating NK cells' expression to achieve HBV clearance.
In conclusion, the situation of innate immune system was very necessary to comprehend the mechanism of chronic HBV infection, this study demonstrated that there were sustained changes of NK cells in patients at different clinical stages of chronic HBV infection. The function of NK cells was activated, and that maybe played an important role in the process of HBV progression and in the treatment by IFN-α.
The limited sample population and duration of follow-up in study precluded us from further refinement. In this study, we have initially discussed immunomodulatory effects of INF-α, but the exact mechanism is not known, we will further investigate the pathways between innate immune system and HBV in antiviral therapy, and put efforts on the phenotypic and functional characterization of NK cells.
Footnotes
Acknowledgments
The project supported by the Medical Technology Development of Nanjing (YKK18243); Nanjing Medical Science and Technique Development Foundation (QRX17098).
Author Disclosure Statement
No competing financial interests exist.