
Abstract
Influenza viruses are major respiratory pathogens that cause seasonal epidemics and occasional pandemics. Immune response to influenza viruses is majorly targeted against the hemagglutinin antigen. A laboratory-based retrospective cross-sectional study was conducted on 50 acute and 50 follow-up samples to assess the immune response to influenza A(H1N1)pdm09 virus after natural infection and detect the presence of pre-existing antibodies against influenza A(H3N2) and influenza B viruses. Two–fourfold rise in hemagglutination-inhibition (HAI) titer was observed in 100% of the follow-up samples for influenza A(H1N1)pdm09 virus. No change in HAI titers for influenza A(H3N2) and influenza B viruses was observed.
Introduction
Influenza virus is a respiratory pathogen that transmits from person to person through respiratory droplets or by direct contact with an infected person (3). Influenza viruses belong to the family Orthomyxoviridae and there are currently four types of influenza viruses that are classified as A, B, C, and D based on the antigenic differences (7). It is estimated that seasonal influenza may result in 290,000–650,000 deaths every year. The global annual attack rate of influenza is estimated to be 5–10% in adults and 20–30% in children (16). In India, influenza accounts for 20–42% of hospitalizations during the rainy season (15).
Influenza virus has two surface glycoproteins namely hemagglutinin (HA) and neuraminidase of which HA is a major antigenic protein. Mutations in the HA protein may result in the emergence of variant influenza viruses causing epidemics and pandemics (2,7). Antibodies against the HA antigen help in the prevention of illness by neutralizing the virus and also facilitating the phagocytosis of virus particles (14). The complex inherited factors and age-related changes are often related to the host immune responses. Natural infection by influenza viruses elicits a protective immune response, directed against the infecting strain and antigenically related viruses (5).
Previous studies on the immune response to influenza A(H1N1)pdm09 virus were mainly focused on detecting antibodies after vaccination (10,11,18). Limited data are available on immune response in patients after natural infection with influenza A(H1N1)pdm09 virus (9,12). In India, data on immune response after natural infection as well as vaccination are unavailable. In this context, the aim of this study was to detect the humoral immune response to influenza A(H1N1)pdm09 virus after natural infection. The study also aimed to determine the presence of pre-existing antibodies against influenza A(H1N1)pdm09, influenza A(H3N2), and influenza B viruses in influenza A(H1N1)pdm09 cases.
Materials and Methods
Study population
Laboratory-confirmed influenza A(H1N1)pdm09 virus cases recruited as part of the project entitled “Hospital-based Surveillance of Acute Febrile Illness in India” conducted by Manipal Centre for Virus Research at Thirthahalli Taluk, Shimoga District, Karnataka, were included in the study. A total of 676 throat swabs were tested positive during January to April 2017. Archived serum samples from the positive cases were stratified into five different age groups (1–5, 6–15, 16–30, 31–50, and 51–65 years) by the systematic random sampling method. Ten acute and 10 follow-up (after 4–6 weeks of infection) serum samples per age group were included for the study. Age-matched serum samples negative for influenza A/B viruses were used as controls (one per age group).
Hemagglutination and hemagglutination-inhibition assay
The hemagglutination assay was performed for influenza A/Michigan/45/2015(H1N1)pdm09-like virus, influenza A/Hong Kong/4801/2014(H3N2)-like virus, influenza B/Phuket/3073/2013-like virus (B/Yamagata-lineage), and influenza B/Brisbane/60/2008-like virus (B/Victoria-lineage) using the “Reagents for the typing of human influenza isolates 2017 developed by the Victorian Infectious Diseases Reference Laboratory, a WHO Collaborating Centre for Reference and Research on Influenza,” as per the manufacturers protocol (13). Hemagglutination titer was determined and antigens were standardized to four HA units to perform hemagglutination-inhibition (HAI). Before performing HAI, nonspecific inhibitors from serum samples were removed using receptor-destroying enzyme (RDE) treatment. HAI assay was performed on all the RDE-treated serum samples for detecting antibody titers against influenza A/Michigan/45/2015(H1N1)pdm09-like virus and pre-existing antibody titers against influenza A/Hong Kong/4801/2014(H3N2)-like virus and influenza B viruses. HAI titer of ≥40 was considered positive for seroconversion. HAI assay with influenza A/Hong Kong/4801/2014(H3N2)-like virus showed background titers up to 80 with sheep control serum as well as normal control serum. Antibody titers against influenza A/Hong Kong/4801/2014(H3N2)-like virus were calculated by subtracting the background values. Geometric mean HAI titer (GMT) was calculated for each age group for both acute and follow-up samples.
Statistical analysis
Data were analyzed using GraphPad Prism 8.0.0, demo version (San Diego, CA). Paired t test was used for the comparison of HAI titers between acute and follow-up samples. Statistical significance was defined as p < 0.05.
Results
HAI antibody response to influenza A(H1N1)pdm09 virus
Out of the 50 acute samples tested, 13(26%) showed HAI titer ≥40, but all the corresponding follow-up samples (100%) showed HAI titer ≥40. In acute samples, the duration between onset of illness and date of sample collection was 2 days (median), indicating the presence of pre-existing antibodies and probable chance of reinfection. A significant fourfold increase in the antibody titers was observed between acute to follow-up samples among all the five age groups. HAI titer and corresponding GMT for each age group are shown in Figure 1. One sample in age group 1–5 years showed high HAI titer in acute sample (640) in comparison with follow-up (160). Another sample in the age group 16–30 years showed no difference in HAI titer (320) between the acute and follow-up samples. A higher number (40%) of acute samples in the age group 51–65 years showed HAI titer ≥40 with one sample having titer as high as 1280 (Fig. 1). Difference in HAI titer between acute and follow-up samples was found to be statistically significant (p < 0.05). Age group-wise HAI titer in acute and follow-up samples is shown in Figure 2.
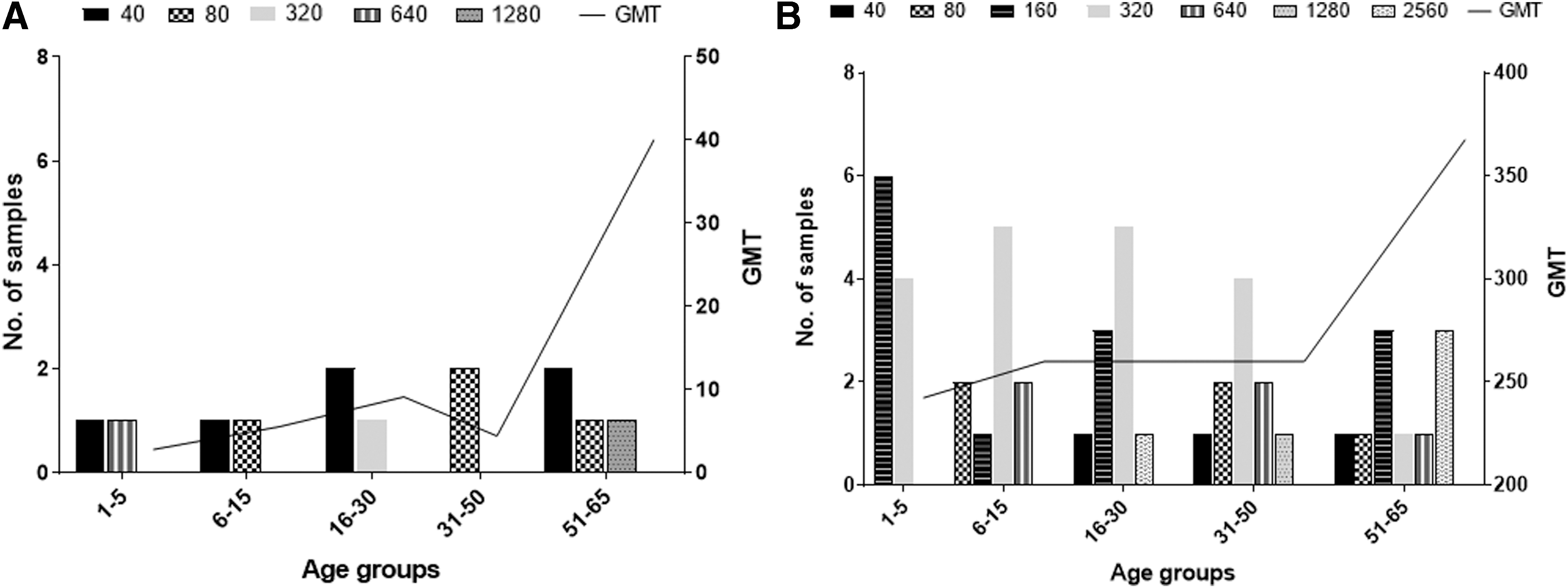
HAI titer against influenza A(H1N1)pdm09 virus in acute
Comparison of HAI titers ≥40 in acute
Pre-existing antibodies against influenza A(H3N2) virus
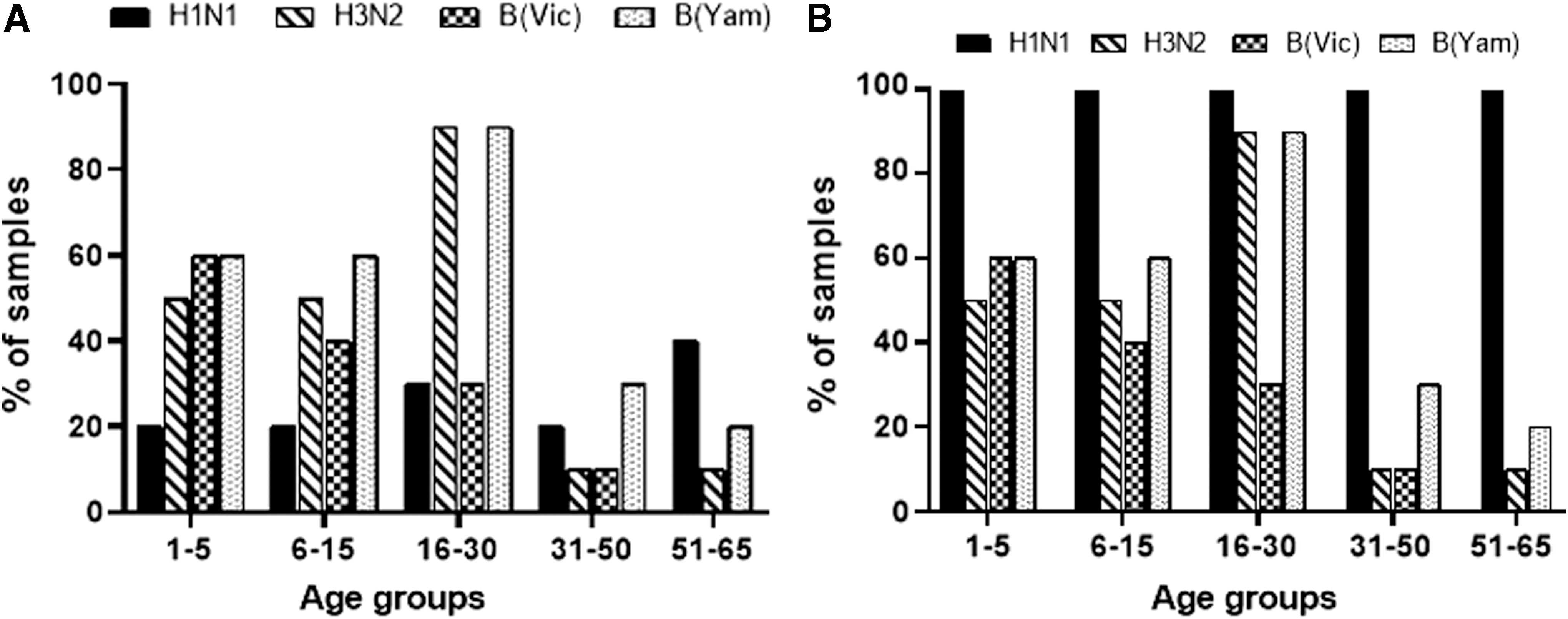
HAI titers against influenza A(H3N2) virus remained same in acute and follow-up samples in all the five age groups. In the age group 16–30 years, 90% of the samples showed HAI titer ≥40, whereas in age groups 31–50 and 51–65 years, 10% of the samples demonstrated HAI titer ≥40 (Fig. 2). No statistical significance was observed in HAI titer between acute and follow-up samples.
Pre-existing antibodies against influenza B viruses
Similar to the HAI results of influenza A(H3N2) virus, there was no difference observed in HAI titer in acute and follow-up samples for influenza B viruses also (Fig. 2). A higher percentage of serum samples from all the age groups showed pre-existing antibodies to influenza B/Yamagata virus in comparison with influenza B/Victoria virus. In the age group 16–30 years, 90% of the samples showed HAI titer ≥40 for influenza B/Yamagata virus. Pre-existing antibodies to influenza B/Victoria among the age group 31–50 and 51–65 years were low (10%) and absent (0%), respectively. Difference in HAI titer between acute and follow-up samples had no statistical significance similar to the results of influenza A(H3N2) viruses.
Discussion
The study demonstrates that natural infection with influenza A(H1N1)pdm09 virus results in seroconversion (HAI titer ≥40) within 4–6 weeks of illness, suggesting the development of humoral immune response in all 50 cases (100%) included in the study. Similar results were demonstrated by Koopmans et al. and Kumagai et al. wherein 90% of the cases showed a fourfold increase in HAI titer during follow-up (8,9). Majority of the acute samples (80%) from age group 1 to 5 years showed no pre-existing antibodies, suggesting the absence of exposure to influenza A(H1N1)pdm09 virus in the past. The presence of pre-existing antibodies was found to be low in younger age groups (up to 30 years), which was similar to the study conducted by Delangue et al. wherein 40% of the individuals of <25 years had low HAI titers (4). Pre-existing antibodies in the age group 31–50 years were also found to be low in this study. The presence of pre-existing antibodies (40%) in the older age group (51–65 years) suggests that there was previous exposure to influenza A(H1N1)pdm09 virus. A previous study by Koopmans et al. demonstrated similar finding wherein antibodies to influenza A(H1N1)pdm09 virus were found to be highest in the oldest age group (>60 years) (8).
Previous studies on cross-reactive immunity against influenza viruses after influenza A(H1N1)pdm09 virus infection showed that cross-reactive anti-HA immunity was developed against different virus subtypes (1,8,11). This study showed a higher magnitude of pre-existing anti-HA antibodies to influenza A(H3N2) and influenza B viruses among patients with influenza A(H1N1)pdm09 natural infection from age groups 1 to 5, 6 to 15, and 16 to 30 years. Cross-reactive antibody response to influenza A(H3N2) and influenza B viruses was not observed in this study since there was no change in HAI titer between acute and follow-up samples. A previous study carried out by Koopmans et al. in age groups 10–19, 20–49, and ≥50 years showed HAI titer ≥40 for influenza A(H3N2) virus (8), but in this study age groups >31 years demonstrated pre-existing antibodies in only 10% cases. Age group 16–30 years showed the higher percentage (90%) of samples with pre-existing antibodies against influenza A(H3N2) virus and influenza B/Yamagata viruses, which correlates with the good immune response induced in younger adults. Antibody titers to influenza B/Yamagata virus were found to be higher than titers to influenza B/Victoria virus, indicating influenza B/Yamagata virus has a higher rate of circulation. According to the World Health Organization, global circulation of influenza B/Yamagata virus has increased since the end of the year 2016 (17). Patients in age groups 31–50 and 51–65 years showed significantly low antibody titers to influenza A(H3N2) virus and influenza B virus, indicating an age-related decrease in antibody titers. A similar study conducted by Jia et al. in the older age group (≥60 years) showed a decrease in antibody titer to influenza A(H3N2) virus with an increase in age (6).
The study demonstrates that influenza A(H1N1)pdm09 virus induces a strong anti-HA immune response after natural infection. The finding of the study demonstrates that the population has been exposed to all four types of influenza viruses, namely influenza A(H1N1)pdm09, influenza A(H3N2), influenza B/Yamagata, and influenza B/Victoria viruses, suggesting that quadrivalent vaccine would be the most appropriate vaccination strategy to prevent influenza outbreaks.
This study was confined to one Taluk of Karnataka state with a smaller sample size; therefore, extensive studies across the country are required to better understand the dynamics of immune responses to influenza viruses in the Indian population. The data from this study form a strong basis for conducting large-scale serosurveillance studies in the future.
Ethical Approval
This study was approved by the Institutional Ethics Committee, Manipal Academy of Higher Education, Manipal (Ref No. UEC/32/2013-2014).
Footnotes
Acknowledgments
This study was funded by ICMR Virology Network Laboratory Grade-I (file. No: 5/8/7/15/2010/ECD-1) and Centers for Disease Control and Prevention, Atlanta, GA, for project entitled Hospital Based Surveillance of Acute Febrile in Western Ghat Region of India (Grant No. 5U01GH001051).
Author Disclosure Statement
No competing financial interests exist.