
Abstract
Recurrent infections of herpes simplex virus in the orolabial area are known as recurrent herpes labialis (RHL). Vitamin D has been shown to have an important immunomodulatory role and to be associated with several infectious diseases. This hospital-based case-control study aimed at investigating the association between vitamin D and RHL by comparing vitamin D levels in individuals with and without RHL. Individuals who presented to the dermatology clinic at a state hospital due to RHL (n = 50) and matching control group of healthy volunteers (n = 51) were studied. Their vitamin D levels were measured, stratified based on clinical guidelines, and compared. The average serum vitamin D (25-hydroxyvitamin D) levels were 23.8 ± 15.5 and 42.0 ± 26.3 nM in the patient and control groups, with significant differences between their average serum vitamin D levels and vitamin D status. The studied population had serious vitamin D deficiency regardless of having RHL, with vitamin D levels below the adequate limits in more than 96% of the population. Most importantly, the study established a significant association between low serum vitamin D levels and the presence of RHL. Further interventional and pathophysiological studies should clarify the nature and mechanism of the relationship.
Introduction
Recurrent infections of herpes simplex virus (HSV) in the orofacial area are known as recurrent herpes labialis (RHL, also known as fever blisters or cold sores) (19). These infections are usually due to type I HSV (HSV1), as opposed to closely related HSV2, which predominantly affects the genitalia or below the waistline (14). The initial infection, known as the primary infection, is kept at bay without clinical symptoms in a vast majority of individuals (10). At the end of the initial infection, the virus enters the sensory nerves and is transported to the sensory ganglia through the axons, most frequently trigeminal ganglion for HSV1, where it evades immune response and establishes a latency stage (10).
A variety of environmental (sunlight, cold, trauma) or physiological (menstrual cycles, emotional stress, immunomodulation, physical fatigue, infections) factors often lead to the reactivation of the latent infection (10,19). These reactivations usually result in painful and unsightly erythematous orolabial lesions that produce vesicles containing infectious virions transmitting the infection to other individuals (10,14). Clinical symptoms of RHL are often mild in immunocompetent individuals and RHL lesions usually heal within 7–10 days, do not leave scars, and are emotionally upsetting at most. However, treatment of HSV infections was considered to be relevant in immunocompetent as well as in immunocompromised individuals due to cosmetic concerns or due to links to other more serious problems such as viral corneal infections and fatal sporadic encephalitis (4,14,17,19).
The prevalence of HSV1 infection and seropositivity was shown to increase with age gradually and to be associated with socioeconomic status (14). Various studies have reported the seroprevalence of HSV1 as 50–60% in the United States, 50–80% in European countries, and 60–90% worldwide (3,19). Not all of those who are seropositive for HSV1 experience RHL, which has a lifetime prevalence of 20–40% in adult populations in the United States and Europe (3). High degree of variation in the prevalence of the HSV infection and the RHL may be attributed to variations in sanitary conditions and the ability of individuals in mounting a proper immune response.
Vitamin D is a steroid hormone with multiple congeners derived from 7-dehydrocholesterol, vitamin D3 (cholecalciferol) being the most important metabolite (8). The vitamin D metabolites are hydroxylated in liver and kidney to produce 25-hydroxyvitamin D (25(OH)D, major circulating form) and 1α,25-dihydroxyvitamin D (biologically active form), respectively. Although vitamin D was classically accredited with a pivotal role in calcium economy and skeletal health, several recent studies have indicated that vitamin D has an important role in the regulation of the immune system (6,8). The presence of vitamin D receptor in the skeletal muscle, heart muscle, colon, breast, prostate, and brain tissues, as well as macrophages/monocytes, and active T and B lymphocytes suggests that vitamin D has a far greater role than just skeletal health (8).
The fact that macrophages or monocytes carry the enzyme that converts 25-hydroxy to 1α,25-dihydroxyvitamin D, which, in turn, regulates cellular proliferation and differentiation in cells of immunity, suggests that vitamin D may have an important role in mounting a proper innate and adaptive immune response in the face of infections (8). Indeed, vitamin D deficiency, a common problem worldwide, has been shown to be associated with various bacterial and viral infections and inflammatory diseases (7,22).
In this study, we compared the vitamin D levels (represented by serum 25(OH)D) of individuals with RHL due to HSV infection with those of individuals without to investigate the association between the two.
Materials and Methods
This hospital-based case-control study included the individuals who presented to the dermatology clinic at Erzurum Palandöken State Hospital in Turkey (Latitude: 39.9°N) between June and November 2016. Case-control studies compare individuals with a specific disease (cases) with those without (controls) in terms of various clinical features. Thus, as in this study, this design allows investigating whether the examined features are more frequently observed in the case or control group and whether they are associated with the disease state and constitute a risk factor. The study sample was divided into two groups: The patient group included those diagnosed with RHL based on physical examination in this period and patient history; the control group included the subjects who were selected in a synchronized manner (i.e., in similar dates as the patients) from a pool of healthy volunteers without any visible herpes infection or history thereof.
The dermatology specialist made the RHL diagnosis. Subjects in the control group were given information about HSV infection, shown color pictures of RHL lesions, asked whether they had experienced such outbreaks, and those who had not were included in the group. Study excluded the subjects younger than 18; those who had taken vitamin D supplement in the previous 12-month period; those with systemic diseases of the liver, kidney, cardiovascular system, or digestive system; or those who used steroids or other immune-modulating drugs. The local Clinical Research Ethics Committee at Atatürk University School of Medicine has approved the study; written informed consent was obtained from all participants.
Serum vitamin D levels
For 25(OH)D (from here on vitamin D) analysis, a 5-mL sample of forearm venous blood was taken into anticoagulant biochemical tubes. Blood samples were centrifuged at 1,000 rpm for 15 min to obtain serum samples. Sera were stored at −80°C for 6 months until analysis. Serum vitamin D levels were measured by using a commercial kit (COBAS reagent kit; COBAS e601 Analyzer Series; Roche Diagnostics, Basel, Switzerland) according to the manufacturer's protocol based on the electrochemiluminescence binding method. Vitamin D levels were stratified based on the Clinical Practice Guideline of the Endocrine Society (9).
Statistical evaluation
Statistical analyses of the data were performed by using SPSS program (v24; SPSS, Inc., Chicago). Frequency and percentage were used to summarize categorical variables; continuous variables were presented as mean ± standard deviation. The distribution of the continuous variables was tested with Kolmogorov–Smirnov test; comparisons of those with normal distribution were performed with an independent-samples t-test. The comparisons of the groups for categorical variables were performed with Fisher's exact chi-square test. Correlations between numerical parameters were evaluated with Spearman's rank correlation coefficient. The level of statistical significance was set at p < 0.05.
Results
A total of 101 individuals were included in the study: 50 in the patient group and 51 in the control group. The descriptive data for and the comparison of the patient and control groups were summarized in Table 1. In the patient group, the average duration of HSV infection was 95 months (7.9 years); the average age of onset of RHL was 24 years; and patients had on average 21 RHL outbreaks per year (1.8 per month). Gender and age distribution in the patient and control groups were similar (p = 0.999 and p = 0.408, respectively). The study sample mostly comprised females (86.1%, M/F ratio: 0.16). The average age of the study sample was 31.0 (±10.6) years, ranging from 18 to 62. The average serum vitamin D level in the study sample as a whole was 13.2 (±9.4) ng/mL (33.0 ± 23.4 nM), which meant that more than 96% of the population had serum vitamin D below the adequate level.
Descriptive Statistics and the Comparison of Vitamin D Levels and Other Biochemical Indicators in the Patient and Control Groups
Bold indicates significant differences between the patient and control groups (p < 0.05).
Fisher's exact chi-square test was used for comparison.
Independent-samples t-test was used for comparison.
Vitamin D levels were stratified based on the Clinical Practice Guideline of the Endocrine Society (9).
ALT, alanine aminotransferase; AST, aspartate aminotransferase; SD, standard deviation; WBC, white blood cell count.
Although a great majority of both the control and patient groups were below the adequate levels according to the recommendations of the Endocrine Society (Fig. 1), a significant difference was found between the RHL patients and the controls in terms of both the average serum vitamin D levels (p < 0.001) and the vitamin D adequacy status (p = 0.003). No significant correlation was found between the number of RHL outbreaks per year and the vitamin D levels (Spearman's r = 0.036, p = 0.805). There was no significant difference between the patient and control groups regarding kidney or liver function or blood test parameters. Although a difference was observed in the platelet counts, both groups were within the reference range (150–400 × 109/L)(p = 0.006).
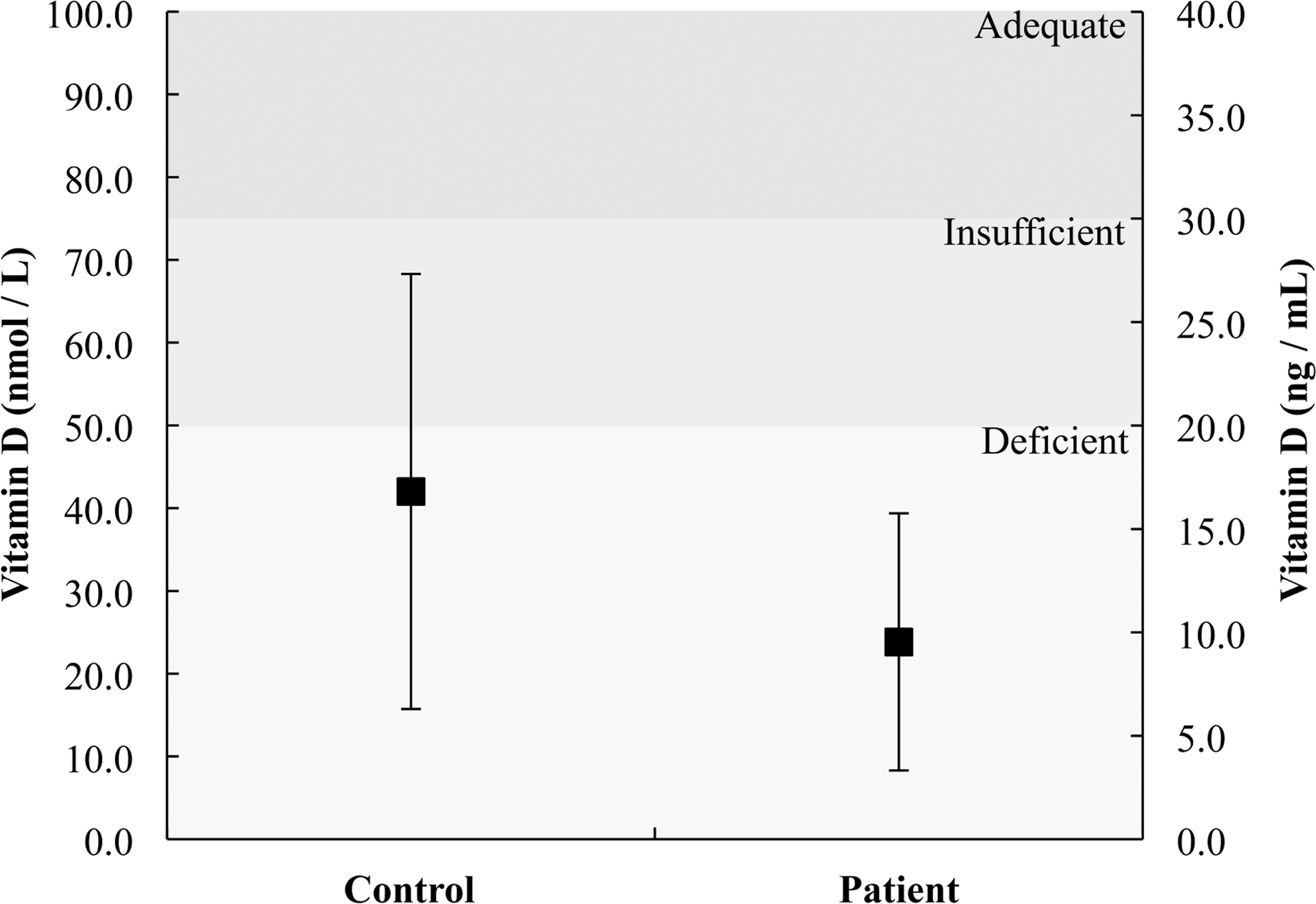
Serum vitamin D levels in the control and patient groups. Error bars represent ± standard deviation.
Discussion
HSV1 infection and the resulting recurrent outbreaks of herpes labialis are ubiquitous in all parts of the world. The fact that RHL episodes generally follow periods of decreased immunocompetency underlines the importance of maintaining a robust immune system in limiting the effects of RHL (12). Vitamin D has been shown to play a pivotal role in the regulation of innate and adaptive immunity, in addition to its classical role in skeletal homeostasis (2,23). In this study, having RHL was found to be associated with lower levels of serum vitamin D.
Although serum vitamin D levels were extremely low in the study sample as a whole, interestingly, none of the subjects in the patient group had adequate levels of serum vitamin D (25-hydroxyvitamin D ≥ 75 nM). This suggests that having adequate levels of vitamin D may contribute to mounting a powerful immune response against recurrent HSV1 infections. This finding is in support of a recent in vivo study, which demonstrated that vitamin D supplementation in two forms downregulated the HSV1 mRNA and DNA and reduced the viral load in HeLa cells (11). Interestingly however, we did not find a link between the number or frequency of RHL episodes and serum vitamin D levels.
A growing number of studies indicate an association between lower vitamin D levels and increased presence of infectious diseases. In agreement with the results of this study, vitamin D supplementation has been suggested to contribute to the protection against seasonal influenza A infection (21). Adequate vitamin D levels were also associated with significantly lower rates of acute viral infections of the upper respiratory tract and lower number of prescriptions for antibiotics (16). Vitamin D deficiency in pregnant women was found to be associated with higher risk of human immunodeficiency virus transmission from the mother to child, which was attributed to a poorer innate immune response to viral activity in these women (1). Vitamin D was found to facilitate the innate immune response against Mycobacterium tuberculosis through the 1α,25-dihydroxyvitamin D-dependent activation of the gene encoding antimicrobial peptide cathelicidin, which kills the bacterium (1).
In general, vitamin D is considered to activate the innate immune system while inhibiting the adaptive immune system; it was even speculated to be at the crossroads of innate and adaptive immune systems (2,7). In case of viral infections such as those involved in RHL, the innate immune system is the frontline defense mechanism and vitamin D-dependent processes through the activation of epithelial cells of the target organ and the immune cells such as macrophages and neutrophils may potentiate the resistance against acute infections (2). Although vitamin D is attributed such a pivotal role in the immunity and the structural human health, its deficiency was found to be widespread in all parts of the world, including developed as well as developing countries (5,20).
There is a general agreement on what serum vitamin D levels should be considered adequate for skeletal health and calcium homeostasis; however, both the nature of vitamin D's impact on non-skeletal tissues and the adequate levels for the optimum effect on these tissues remain disputed (16). Some studies also argue that lower vitamin D values might be a result rather than the cause of diseased state (13). Nevertheless, it has been suggested that a proper regulation of calcium homeostasis and skeletal health requires serum vitamin D levels above 50 nM whereas values above 75 nM are generally recommended to get full benefit for non-skeletal tissues such as the cells of the immune system (15,16). The letter value is close to the Km (Michaelis constant) of 25-hydroxyvitamin D-1α-hydroxylase for its substrate, 25-hydroxyvitamin D, in macrophages (18).
Adequate levels of serum vitamin D (25-hydroxyvitamin D) have been suggested to allow macrophages to locally generate 1α,25-dihydroxyvitamin D, which acts as an intracrine or autocrine hormone and elicits biological response in the cells in the vicinity to facilitate an appropriate immune response (1). That being said, this study indicated that the studied population had serious vitamin D deficiency according to the commonly accepted clinical guidelines, regardless of having RHL outbreaks (9). The reason for this deficiency is an important subject but this study did not address this issue, as we did not collect data on the factors such as dietary habits or sun exposure practices of the participants, which are known to affect serum vitamin D levels.
As a matter of fact, the province of Erzurum, where the study was conducted, is in a religiously and socially more conservative part of the country, which may have an effect on the clothing preferences and sun exposure practices of the participants, leading to lower levels of vitamin D. However, since the case and control groups were randomly selected from the same geographic region and cultural backgrounds, we have reason to believe that they were similar in terms of dietary habits or sun exposure practices, although we did not collect data on these factors.
This study has some limitations associated with the data collection procedure as well as the nature of the infection in question. First, we have collected vitamin D data from patients throughout a period covering summer and fall; attention was paid to keep the patient and control groups temporally synchronous but we were not able to analyze the seasonal variations due to limited sample size. Second, we did not investigate the serological markers for HSV1 infection in the control group, which means that lower rates of RHL in controls might be due to the absence of the primary infection of HSV1. Thus, this study only reflects the differences between the populations with and without RHL outbreaks, regardless of HSV1 seropositivity.
Lack of data on the dietary habits or preferences or sun exposure practices of the participants was another limitation of the study. Finally, the results only suggest an association between the two but not a causative role for vitamin D since we did not intend to perform an interventional study to determine the influence of vitamin D levels on the frequency of outbreaks, which may be a follow-up study.
Conclusion
In conclusion, this study found a serious vitamin D deficiency in the studied population regardless of their infection status. The study also demonstrated a significant relationship between low levels of circulating vitamin D metabolites and the presence of RHL, regardless of the primary infection presence. More research is warranted for clarifying the degree of association, seasonal variations, the mechanism of the relationship, and whether the relationship is causative or not, through pathophysiological and interventional studies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.