
Abstract
Hepatitis delta virus (HDV) is a highly pathogenic virus and causes rapid disease progression from fulminant hepatitis to development of hepatocellular carcinoma in patients infected with hepatitis B virus (HBV). HDV is endemic in Pakistan; however, there are no available data on HDV prevalence among the high-risk group of HBV-infected pregnant women. A total of 1,394 pregnant women, visiting different public-sector hospitals in Lahore, were enrolled in this study. Their demographic data and blood samples were collected from May 2016 to July 2017. Samples were screened for both HBsAg and anti-HDV. Anti-HDV positive samples were tested for HDV RNA, and samples positive for HDV RNA were further sequenced to determine the HDV genotype. Of the 1,394 samples, HBsAg was positive in 63 (4.5%). Of these 63 HBsAg-positive samples, 13 (20.63%) were positive for anti-HDV. Of the 13 HBsAg/anti-HDV positive samples, HDV RNA was detected in 4 (30.8%) samples and all 4 carried HDV genotype 1. The age of enrolled women varied from 20 to 40 years, with most of the women living in urban areas, having education more than secondary school level, belonging to middle class, and being housewives. Majority of the tested women were of age from 25 to 30 years (39.2%); however, the prevalence of HBV was higher in age group 31–35 years (10.7%, confidence interval [CI]: 4.73–16.67); however, anti-HDV prevalence was 1.9% (CI: −0.7 to 4.7). This study is the first report on HDV prevalence among pregnant women in Pakistan. Our study showed a high predominance of HDV (20.63%) in HBV-infected pregnant women and the prevalence of HDV genotype 1 infection. The findings contribute to a better understanding of the HDV/HBV coinfection among pregnant women and circulating HDV genotypes in the country.
Introduction
Hepatitis delta virus (HDV) is a satellite virus that is dependent on hepatitis B virus (HBV) for its replication and expression. Chronic HBV and its coinfection or super-infection with HDV continues to be a major health burden worldwide. HBV–HDV coinfection results in more severe acute diseases than HBV monoinfection, and aggravates the risk of severe complications such as hepatocellular carcinoma, cirrhosis, and fulminant hepatitis (17). It is estimated that >350 million people are infected with HBV infection of which 15–20 million are coinfected with HDV worldwide (23). More than 68,000 HBV-infected people die annually (15). Hepatitis B is very much endemic in Pakistani general population infecting 7–9 million people, with a prevalence ratio between 3% and 5% (3).
Molecular characterization shows that both HBV and HDV are genetically highly diverse; HBV has been classified into 10 groups (A–J), whereas there are eight distinct clades of HDV 1–8 (11). There is no efficient direct acting antiviral therapy available for >15 million chronic HBV patients coinfected with HDV infection.
Hepatitis D virus is ssRNA virus with ∼1.7 kb long circular genome surrounded by HBsAg coat of dsDNA HBV virus. Prenatal transmission is thought to be the most important route of transmission of both viruses (6). Pakistan is considered endemic to HDV infections with the seroprevalence ranging from 16.5% to 58.9% (7). Except few studies, most of the reported studies focused the stratified groups of hepatitis patients or patients at higher risk of HDV infections. However, recent molecular epidemiological data on HBV/HDV coinfection report prevalence rate of 14.6% of HDV in HBV-infected people (2).
As HDV causes disease progression much faster in patients affected with HBV, also it can be transmitted from mother to child, but no such data are available on HDV/HBV prevalence among the pregnant women in Pakistan, and this is the first study to address this issue. Therefore, the main objective of the study was to estimate the prevalence and characterize the HDV/HBV infection among pregnant women of Pakistan.
Materials and Methods
Samples were collected from different public-sector hospitals of Lahore district, Punjab, Pakistan between May 2016 and July 2017. The study was directed in two phases. In the first phase, written informed consent was obtained from the entire participants after explaining the objectives of this study. A detailed questionnaire was filled by each participant, while the questionnaire/data sheet contained the information about history of jaundice, diagnosis of HBV in family, area, education level, socioeconomic status, work status, and age. About 5 mL of blood sample collected in Ethylenediaminetetraacetic acid (EDTA)-containing tubes was centrifuged, and plasma was stored in aliquots at −20°C. In the second phase, samples were analyzed for HBV/HDV infections through enzyme-linked immunosorbent assay (ELISA), and then by polymerase chain reaction (PCR) for presence of HDV viral RNA and genotype.
A total of 1,394 pregnant women had given consent to enroll in the study that had no clinical or biological signs of severe hepatitis infections. Enlisted women belonged to different geographical regions of the province. The collected sera of all pregnant women were subjected to serological analysis of HBsAg and anti-HDV antibodies using ELISA (DIA.PRO; Diagnostic Bioprobes Srl, Italy) according to the manufacturer's instruction in the specified manual. The data were analyzed statistically using SPSS version 20, and p-values <0.5 were considered significant.
Samples positive for anti-HDV antibodies were further analyzed for confirmation of HDV viral RNA. Two hundred microliters of the serum sample was used for HDV RNA extraction using the Nucleospin Extraction Kit from Macherey-Nagel (Duren, Germany) according to the kit protocol. The detection and genotyping of HDV RNA were done as described previously [2]. In brief, RNA was extracted using a Nucleospin Viral RNA Extraction kit (Macherey-Nagel), and qualitative analysis of HDV was done in a SmartCycler by using real-time PCR kit from Sacace Biotechnology (Como, Italy). For genotyping of HDV, cDNA was synthesized, and reported primers were used in nested PCR following the same protocol (2) for the amplification of 406 nucleotide fragment of HDAg gene. Eluted PCR products amplified by inner sense and antisense primers (utilized in nested PCR) were sequenced with ABI Prism BigDye terminator cycle sequencing ready reaction kit (ABI, Foster City, CA) and run on a 3100 Automated Genetic Analyzer (Applied Biosystem, Inc.). By aligning the sequenced strands using both forward and reverse primers, consensus sequences were generated after validation using the Phred-Phrap Software (Seattle). Sequences were submitted (accession no. MF677937 to MF677940) to GenBank (National Center for Biotechnology Information, Bethesda, MD). Forty-three HDV genotype 1–8 sequences were retrieved from GenBank. Sequences were aligned using CLUSTAL Omega. After manually adjusting the alignment, the evolutionary history was inferred by using the maximum-likelihood method based on the general time reversible model (16). The tree with the highest log likelihood (−3,766.16) is shown. Initial tree(s) for the heuristic search were obtained automatically by applying the maximum parsimony method. A discrete gamma distribution was used to model evolutionary rate differences among sites (five categories (+G, parameter = 0.4810)). The rate variation model allowed for some sites to be evolutionarily invariable ([+I], 24.79% sites). The tree is drawn to scale, with branch lengths measured in the number of substitutions per site. The analysis involved 46 nucleotide sequences. All positions containing gaps and missing data were eliminated. There were a total of 357 positions in the final dataset. Evolutionary analyses were conducted in MEGA7 (10).
Results
In this study, total 1,394 pregnant women were enrolled in the study, who fulfilled the study criteria and had filled the complete data sheet. The ages of enrolled women vary from 20 to 40 years, with most of the women living in cities, having education more than secondary school level, belonging to middle class, and being housewives (Table 1). All sera samples were initially screened for HBsAg ELISA from which 63 (4.52%) samples were positive. Of 63 HBsAg-positive sera, anti-HDV ELISA was found positive in 13 samples (20.63%). Majority of the tested women were of age from 25 to 30 years (39.2%); however, the seroprevalence of HBV among pregnant women was higher (10.7%; with confidence interval [CI]: 4.73–16.67) in age group 36–40 years (Table 1). Anti-HDV prevalence was also common (1.9%, CI: −0.7 to 4.7) in pregnant women with age ranging from 36 to 40 years (Table 2).
Prevalence of HBV Among Pregnant Women According to Different Selected Variables
CI, confidence interval; HBV, hepatitis B virus.
Distribution of HDV According to Different Selected Variables in the Pregnant Women
HDV, hepatitis delta virus.
RNA was extracted from all the 13 anti-HDV reactive cases and was analyzed for HDV infection using HDV-specific primers in nested PCR. Four hundred six nucleotides fragment was amplified. Total of 4 (30.8%) of 13 anti-HDV positive samples were found positive for HDV RNA. Of four samples, one was found positive in age group between 21 and 25 years, two were positive in age group between 26 and 30 years, and one was found positive for HDV RNA in age group between 31 and 35 years. The higher incidence of HDV may be due to the medical deprivation and low socioeconomic positions of the pregnant women. The nucleotide sequence of the local strains showed 90–93% homology with the reference HDV genotype I isolate. All of the four local isolates cluster with HDV genotype IE (Fig. 1), showing HDV I the only prevalent HDV genotype among this risk group. The 1E group was further divided into three clades, and our Pakistani isolates fell in two different clades E-I and E-II. Sequence MF677937 was closer to isolates from Iran. Rest of the three isolates made a separate clad.
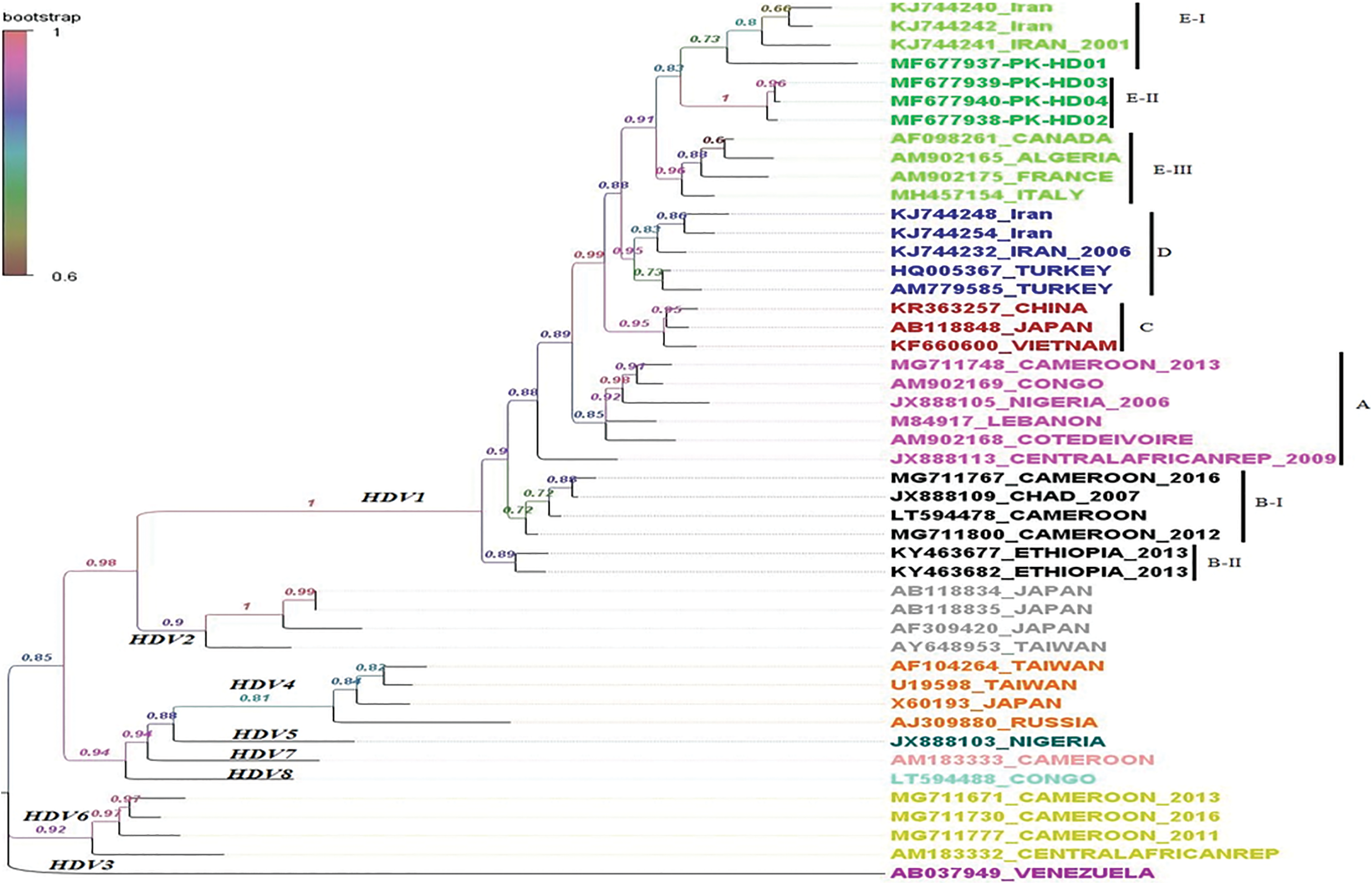
Phylogenetic analysis of HDV isolates from pregnant women in Pakistan. HDV phylogeny was constructed using maximum likelihood through GTR + G with 1,000 bootstraps. Branches are colored and labeled according to bootstrap values. Pakistani isolates group into two distinct clads E-I and E-II of genotype HDV1E with strong bootstraps of 1 (E-II) and 0.73 (E-I). Tip labels are colored for better understanding of different genotypes and clades. GTR+G, general time reversible+gamma; HDV, hepatitis delta virus. Color images are available online.
Discussion
The HBV monoinfection and HBV/HDV coinfection rates have been estimated using serological assays in this study. The prevalence and characterization of HDV among pregnant women were further analyzed by using nested PCR, sequencing and constructing a phylogenetic tree. Pregnancy has been considered as a potential risk factor for replication of the virus due to low immune response of the pregnant women (21). Postpartum hemorrhages, coagulation defects, organ failure, and high maternal mortality as well as poor outcomes in newborns, for example, neonatal deaths, still births, acute or chronic liver disease and hepatocellular carcinoma are well associated with viral hepatitis in pregnancy; therefore, early diagnosis is required (8). Incidence of viral hepatitis widely varies in different geographical regions, but the severity and course of the viral hepatitis are relatively different in pregnant women as compared with nonpregnant women in developing countries and the developed countries (9).
In this study, the seroprevalence of HBV monoinfection and HDV/HBV coinfection is significantly higher in the age groups from 36 to 40 years; however, detection of HDV RNA using nested PCR shows higher infection rate in age group 26–30 years, which is in accordance with the already published data in which coinfection with HDV was higher in age group (21–30 years) in Pakistan (2). We found an overall HBV monoinfection prevalence rate of 4.5%, which is relatable to the already published data from the country with HBV seroprevalence rate of 3–5% (3) and the overall prevalence rate of HBV/HDV coinfection was 1.10% (13/1,394); however in HBV-infected pregnant women it was 20.63% (13/63) in Pakistan. However, prevalence of HDV antibody in Pakistani HBsAg-positive individuals is 16.6% (1).
This is the first study to demonstrate the bioburden of HBV–HDV coinfection among pregnant women in Pakistan. The findings of our study are in contrast to those reported by Vranckx et al., who revealed that no anti-HDV antibodies were found in HbsAg-positive pregnant women of Indonesia (22). Likewise, another study exhibited very low prevalence of HDV in HBV-infected population in Birjand Hepatitis Clinic, Iran (24). Another study corroborates the findings of our result by showing >14% coinfection of HBV–HDV in pregnant women in Mauritania (12).
The prevalence of HBV and HDV in pregnant women suggests a high rate of vertical transmission of both viruses. HDV genotype I was only found in all the HDV RNA-positive samples, which is in accordance with the already reported data from the country (2,5,14,18). Splitting of Pakistani isolates into two clades in genotype E shows that HDV is going through intraevolution in Pakistan (Fig. 1). Our isolates share evolutionary history with isolates of Iran, Canada, France, and Italy. The finding is also in agreement with the predominant HDV genotype in the neighboring country such as Iran and in the middle-east regions such as Lebanon, Egypt, and Turkey (4,13,19,20).
Conclusion
In conclusion, this research represents the first large-scale study related to HBV and HDV infection in pregnant women. Our study reported 4.5% prevalence of HBV in pregnant women of which ∼20.63% had HDV coinfection. It is necessary to practice safe injections, and introduce mass immunization programs and more effective treatments for the elimination of viral infections and control of HBV–HDV related morbidity and mortality. Further studies are required on clinical implication of HDV among pregnant women.
Footnotes
Acknowledgments
The authors acknowledge all the patients for providing the samples and all the doctors and paramedical staff of the hospitals (involved in this study) for their cooperation.
Ethical Approval
This study was approved by Institutional Ethical Committee (“Ethical Review Committee of Lahore College for Women University”). Informed written consent was obtained after detailed explanation of the study at the time of sampling from all participants.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.