
Abstract
Hepatitis C virus (HCV) is a major public health concern globally, resulting in liver-related complications. Approximately 6% population of Pakistan is infected with HCV. HCV is error prone, due to which it is classified into 7 genotypes and 67 subtypes. HCV genotype determination is critical for treatment and therapy response. In this study, 3,539 samples were collected from 2015 to 2019 from all over Punjab. RNA was extracted from samples using QIA Amp Viral RNA MINI kit (Qiagen, Germany) and viral genotyping was performed. Furthermore, a systemized literature search (2009–2018) was done to analyze the HCV genotype distribution pattern in Pakistan. In Punjab, genotype 3a (86.46%) is most prevalent, followed by untypable (7.17%) and genotype 1a (3.84%) and 3b (1.04%). Mixed genotype constitutes only 0.67% of total infections. Genotype 2a, 2b, 3c, and 4 were found to be rare. Data available from literature review when compiled showed that HCV genotype 3a (58.16%) was predominant in Pakistan, followed by genotypes 3b (9.05%), 2a (6.70%), 1a (6.22%), and 1b (2.39%). The frequency of mixed genotypes was found to be 4% and 12% of untypable HCV variants. This study highlights the HCV genotype distribution pattern in different regions of Pakistan. Therapy response and disease management depend on genotype, so HCV genotype determination is crucial. In Pakistan, the most prevalent genotype is 3a, followed by untypable genotype. Both interferon and sofosbuvir are effective against genotype 3a, but treatment with sofosbuvir has comparatively high sustained virological response, less adverse effects, and more tolerability.
Introduction
Hepatitis C is a considerable public health challenge worldwide (4). Hepatitis C virus (HCV) precisely affects the liver causing chronic hepatitis and hepatocellular carcinoma (HCC), resulting in morbidity and mortality worldwide (23,72). According to an estimate, almost 200 million people are thought to be infected with HCV around the globe (5,23,63). Worldwide, roughly 350,000 deaths occur due to pathological hepatocellular complications caused by HCV (5,72). High fatality rate of HCV-infected individuals can be correlated to the fact that persistent and untreated HCV infections can lead to the development of HCC (58). One of the major risk factors for the development of HCC includes HCV infections and the most prevalent HCV genotype in HCC patients was 1b (60). The progression rate of HCV chronic hepatitis to the development of HCC seems to depend on various host and environmental factors, that is, age, gender, alcohol consumption, viral load, and viral variants (57).
African and east Mediterranean regions have the highest rate of HCV prevalence, whereas the regions having minimal HCV prevalence (<2%) are Americas, Australia, and Western Europe. Although the prevalence of HCV is different for individual countries in Asia, its combined prevalence is estimated to be slightly more than 2%. Egypt surpasses other nations, being the country bearing the highest HCV burden of ∼14% (73). Of the total population of Pakistan, 6% individuals are infected with HCV, suggesting that viral hepatitis is alarmingly high in general population (48). An estimate suggests that ∼10 million individuals in Pakistan are infected with HCV, making it a state with second highest HCV burden after Egypt (7). In developing countries like Pakistan, HCV burden is continually on the rise, significantly due to lack of awareness, unsafe blood transfusion, improper surgical and dental procedures, use and reuse of unsterilized syringes and medical equipment, and unsafe barber, tattooing, and nose/ear piercing tools (4,8,75). Prevalence of HCV in high-risk groups is 66%, which is much higher than the prevalence in general population (3.13–23.83%) and healthy blood donors (1.05–20.8%) (4,73).
HCV belongs to family Flaviviridae and is a member of genus Hepacivirus (35). It is a positive single-stranded RNA virus comprising 9.6 kb genome encoding a single polypeptide (31,43). Replication executed by RNA-dependant RNA polymerase is error prone, which results in severe heterogeneity of HCV (19,71). According to an estimate, 10−2 mutations occur per nucleotide per year (64).
HCV genome is classified into 7 major genotypes based on its phylogenetic and sequence analysis; genotypes are further classified into 67 recognized subtypes and 20 provisional subtypes (52). Genotype 1 and genotype 3 are distributed worldwide, accounting 46% and 30% of all HCV infection, respectively (52). In European countries, genotype 1 is most prevalent followed by genotype 2 and genotype 3 (58). South Asia accounts for most (75%) cases of genotype 3. East Asia is endemic with genotype 2 and genotype 6. Genotype 5 is very rare and most cases are found to be present in Eastern and Southern Africa. In Middle Eastern non-Arab countries (Cyprus, Israel, Iran, and Turkey), genotype 1 accounts for most of the cases, whereas Arabian countries are endemic with genotype 1 and 4 (70).
In Pakistan, the most predominant HCV genotype is 3a and 3b followed by 1a, 2a, and untypable genotype (6,7,18,37). In Khyber Pakhtunkhwa (KPK), Punjab, and Sindh, genotype 3a and 3b were found to be most prevalent, whereas most of the patients from Baluchistan were infected with genotype 1a and 2a (37).
Determination of HCV genotype is critical for deciding the clinical management and predicting the prognosis of HCV infection. Genotype is the fundamental predictive parameter for sustained virological response (SVR) (81). In Pakistan previously, the main option for treatment was interferon (IFN) based on its ease of availability, low cost, and high SVR against particular genotypes (4). Other options include pegylated IFN (PEG-IFN), ribavirin, or their combinations (10,67,79). Advancement in the development of direct-acting antivirals (DAA) has revolutionized the treatment approach, having high SVR with lesser side effects and short duration. The Asian Pacific Association for the study of the Liver guidelines have emphasized on the use of Solvadi (sofosbuvir-NS5B inhibitor) for treating viral genotypes GT1, GT2, and GT3 (4).
As the genotype determination is crucial for the selection of therapeutic strategies and duration, in such circumstances, there is a need to analyze the HCV genotype distribution pattern in different regions of Pakistan to precisely design a treatment strategy according to viral genotype.
Methodology
Sampling
The study was conducted from 2015 to 2019. A total of 3,539 (Males: 1,609 [45.46%], females: 1,930 [54.53%], M/F ratio: 1:1.19) samples from Punjab were genotyped for the study with informed and written consent of each patient. We excluded the subjects with comorbidities, pregnant women, and the participants younger than 7 years. This study was approved by the ethical committee of Department of Life Sciences, University of Management and Technology, and Lahore Clinical Laboratory and Research Centre, Lahore, Pakistan.
HCV qualitative test
Serum separated from the blood samples collected from 3,539 hepatitis C patients was subjected to RNA extraction using QIA Amp viral RNA MINI kit (Qiagen, Germany). All the steps of HCV quantitative test were performed according to the protocol provided by the manufacturer. In a reaction mixture of 20 μL, reverse transcription of 5′ untranslated region (5′ UTR) of extracted viral RNA was carried out using reverse transcriptase enzyme of Moloney–Murine Leukemia Virus (M-m LVRTase; Invitrogen), at 37°C for 60 min. Polymerase chain reaction (PCR) of first round was carried out using antisense and outersense primers to amplify the complementary DNA (cDNA) of 5′ UTR (55). Second round of nested PCR was completed using inner primers. Thermus aquaticus (Taq) DNA polymerase was used to amplify template DNA in both first and second round of PCR. The amplified product produced in first round of PCR was used as a template in second round of nested PCR. A Gel documentation system was used to visualize the amplified PCR products of second round, when they were made to run on 2% agarose gel electrophoresis. Reconfirmation of all the PCR-positive samples was done on Real-Time Rotor Gene Equipment (Qiagen) using HCV RG–RT PCR kit.
HCV genotyping
All HCV-positive samples were subjected to genotyping. Generally, six distinct genotypes of HCV can be/were identified using the method of Ohno et al. (55). Two hundred units of M–mL Virus RT was used to carry out the process of reverse transcription for the synthesis of cDNA using viral RNA (10 μL) as a template. In first round of PCR, forward primer (5′-GGGAGGTCTCGTAGACCGTGCACCATG-3′) and reverse primer (5′-GAGACGGGTATAGTACCCCATGAGAGTCGGC-3′) were used to amplify 5 μL of synthesized cDNA. For each first-round PCR sample, two second-round PCRs were performed. One second round was carried out with mix 1, composed of primers for genotype 1b, 2a, 2b, and 3b. The other second round was completed with mix 2, which consisted of genotype-specific primers for 3a, 4, 5a, 1a, and 6a. Taq DNA polymerase (Invitrogen) was used to amplify the template cDNA in all PCRs. Amplified products of second round of PCR was visualized on gel documentation system after they were subjected to electrophoresis on 2% agarose gel with a DNA marker of 100 bp ladder. HCV genotype of each sample was confirmed by comparing the obtained band size with the HCV genotype-specific PCR band.
Literature review
A systematic review of literature was conducted on PubMed, PakMedinet, and Google scholar using the following keywords: “HCV, Genotype, Prevalence, and Pakistan.” In total, 55 articles were searched for the HCV genotype distribution in different regions of Pakistan; out of these, only 36 studies were included in our study and 19 articles were excluded. The articles that did not have subtypes of HCV genotypes required for our analysis and articles before 2009 were not included in this study.
Results
A total of 3,539 HCV-positive samples were genotyped from year 2015 to 2019. Out of 3,539 patient samples, 1,930 (54.37%) were female and 1,609 (45.62%) were male (Table 1). The distribution frequency of different viral genotypes and subtypes was determined and evaluated as shown in Figure 1. Genotype 3a was found to be the most prevalent genotype (n = 3,060, 87%), followed by untypable genotype (n = 254, 7.17%), genotype 1a (n = 136, 3.84%), and genotype 3b (n = 37, 1.04%), whereas very rare number of patients of genotype 2a, 2b, 3c, and 4a was reported to be infected in our study. Co-infection of genotypes accounts 0.67% of total infected pool, as illustrated in Figure 1.
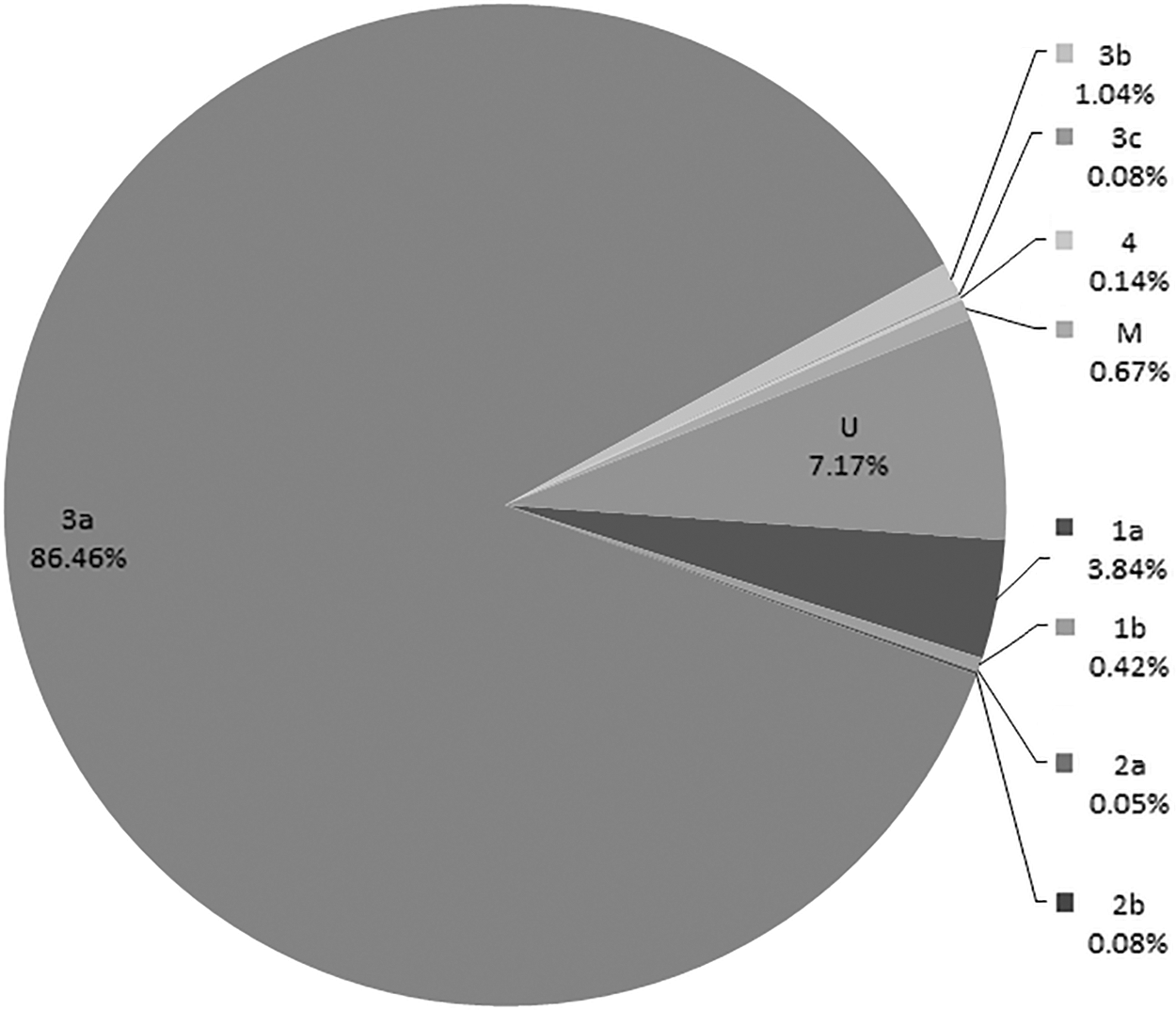
Results of this study showing HCV genotype distribution in Punjab (2015–2019). HCV, hepatitis C virus.
Hepatitis C Virus Genotype Distribution in Punjab (2015–2019)
SD, standard deviation.
Available literature analysis from 2009 to 2018 about the frequency distribution pattern of HCV genotypes in Pakistan showed that genotype 3a (58.16%) was the most prevalent in Pakistan, followed by genotypes 3b (9.05%), 2a (6.70%), 1a (6.22%), and 1b (2.39%). Genotypes 2b and 4b accounted for 0.82% and 0.05% of the total sample pool of Pakistan. The frequency of mixed genotypes was found to be 3.47% and 11.82% of samples could not be assigned a specific genotype or subtype. Infections due to HCV genotype 5a, 6a, and 4b were rare, accounting 0.09%, 0.06%, and 0.05%, respectively, as shown in Table 2 and Figure 2.
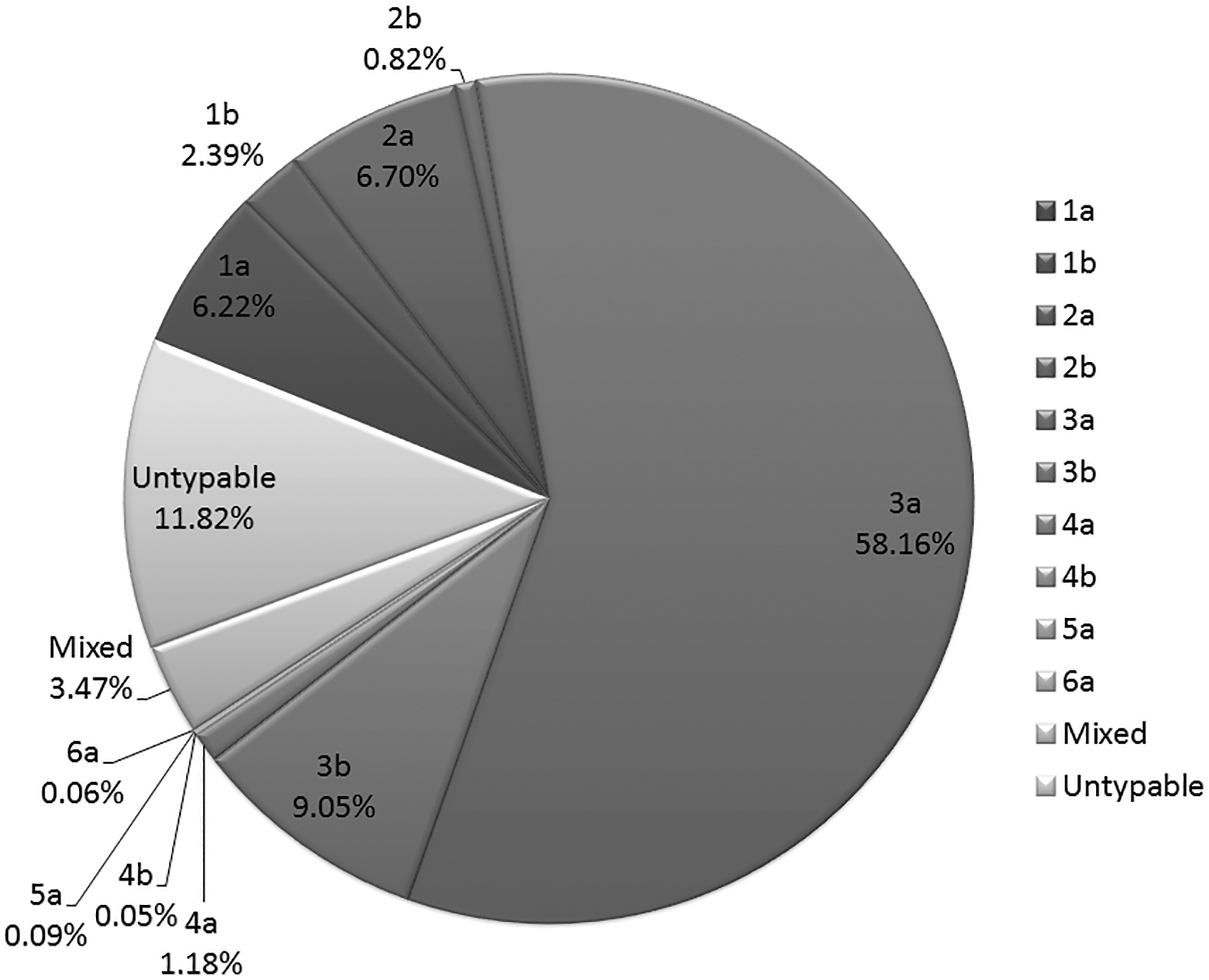
HCV genotype distribution in Pakistan (2009–2018).
Hepatitis C Virus Genotype Distribution in Pakistan (2009–2018)
S. No., serial number; TS, total sample; HCV, hepatitis C virus; AJK, Azad Jammu and Kashmir; KPK, Khyber Pakhtunkhwa.
In Punjab province, a significantly higher frequency of genotype 3a (80.23%) was observed and the untypable genotype (4.91%), which was appreciably lower (in frequency) compared to other provinces. The other genotypes followed by genotype 3a were 1a (6.46%), 3b (3.97%), 4a (2.45%), and mixed (1.98%), as illustrated in Figure 3. Both the genotypes 1b and 2a accounted for only 0.76% and 0.45% of the total sample pool. Patients diagnosed to be infected with HCV genotype 4b (0.23%) and 6a (0.05%) were rare.
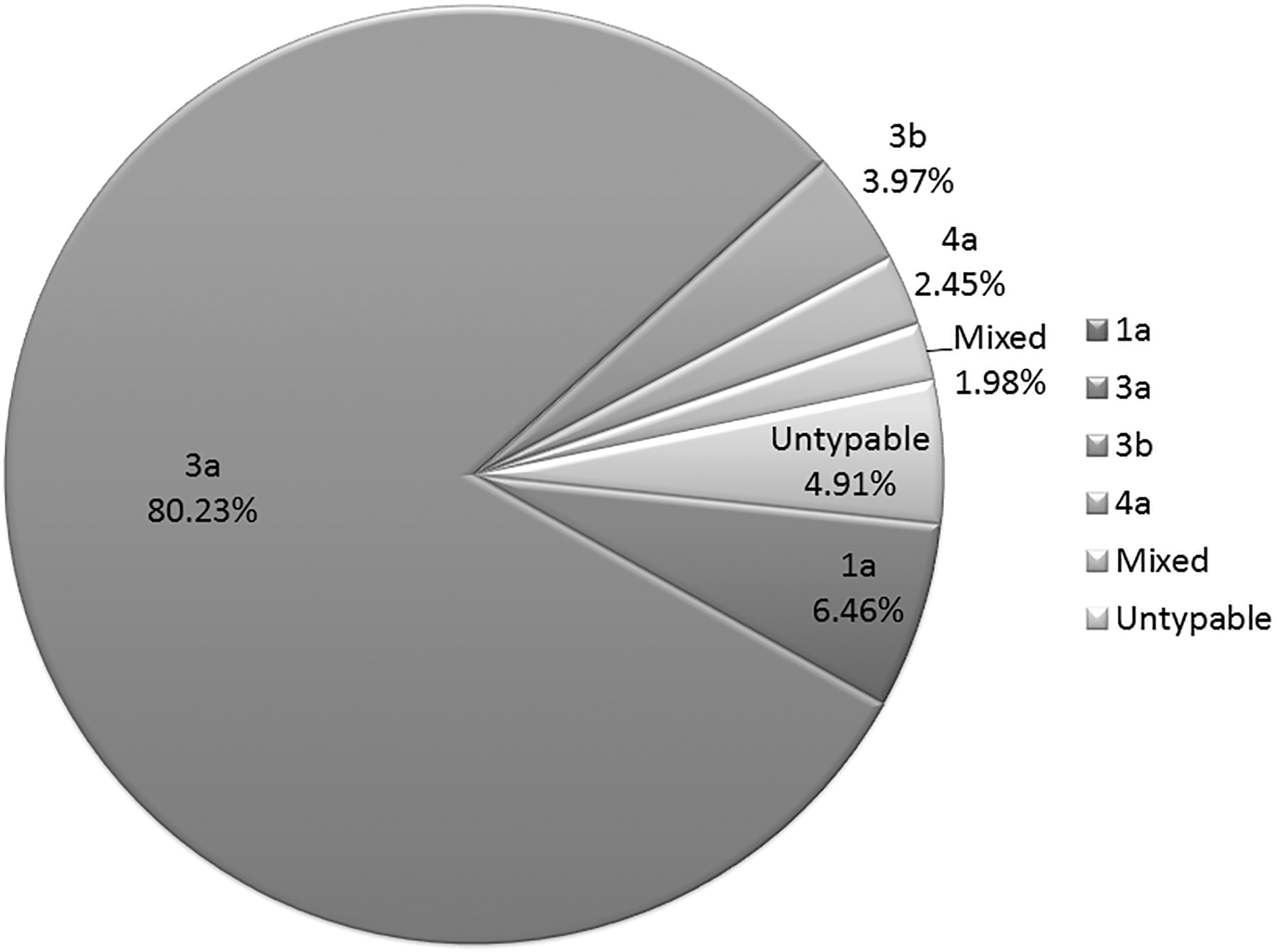
HCV genotype distribution in Punjab.
Of the successfully genotyped samples in Sindh province, 61% were infected with 3a, 21% were HCV sample-unidentified genotype, 9% were 3b, and 4% were 1a. Two percent samples were infected with 1b and 2a each. Mixed genotypes constitute only 1% of total samples genotyped, as shown in Figure 4.
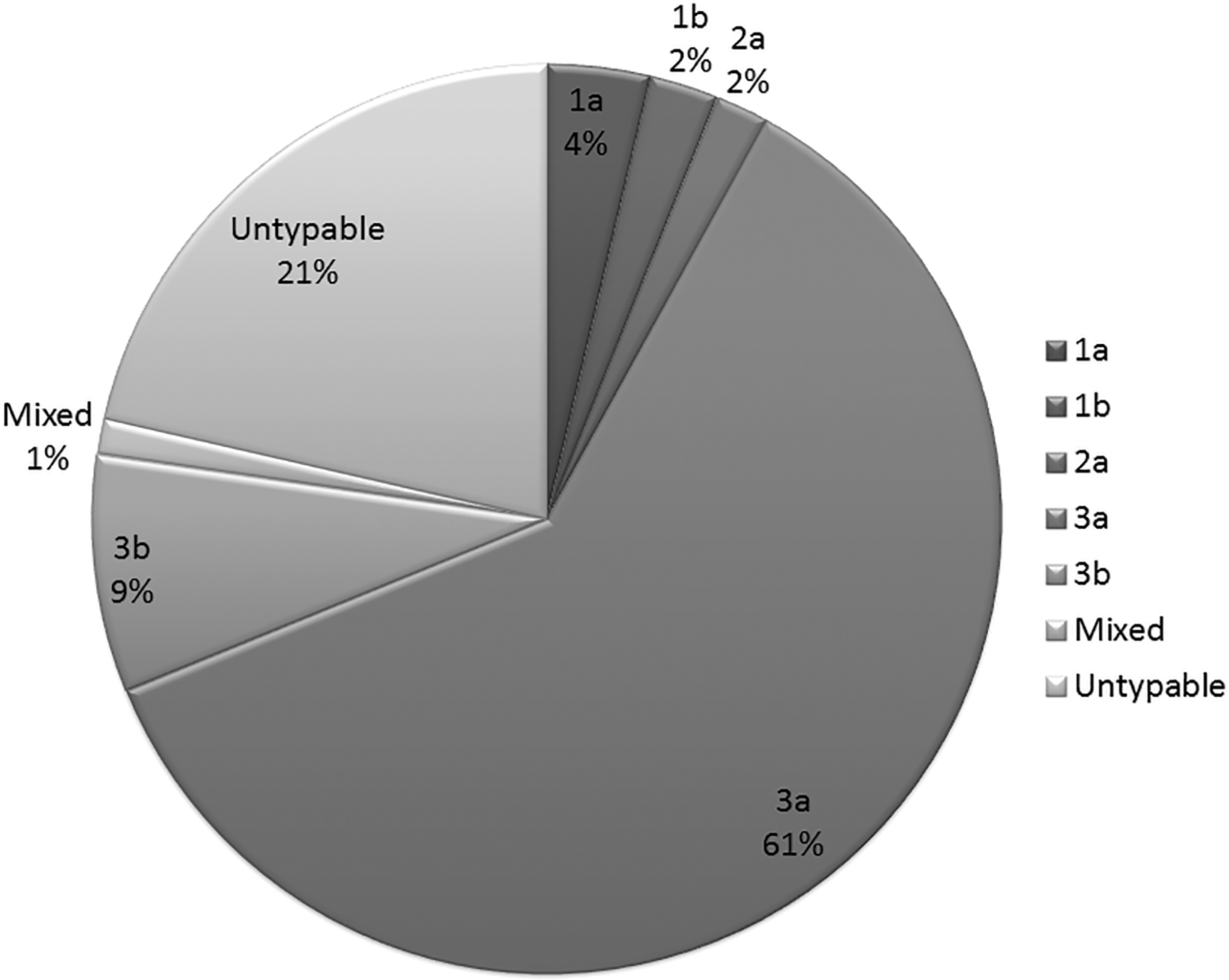
HCV genotype distribution in Sindh.
The genotype distribution pattern in KPK province was a bit different from other provinces of Pakistan in which genotype 3a (49%) was followed by genotype 2a (12%) and untypable genotype (14%), whereas in other provinces, genotype 2a was rare. The frequency of all other genotypes were 3b (9%), 1a (7%), and mixed (5%). Genotype 4a and 2b account for only 1% of the total samples genotyped in KPK, as shown in Figure 5.
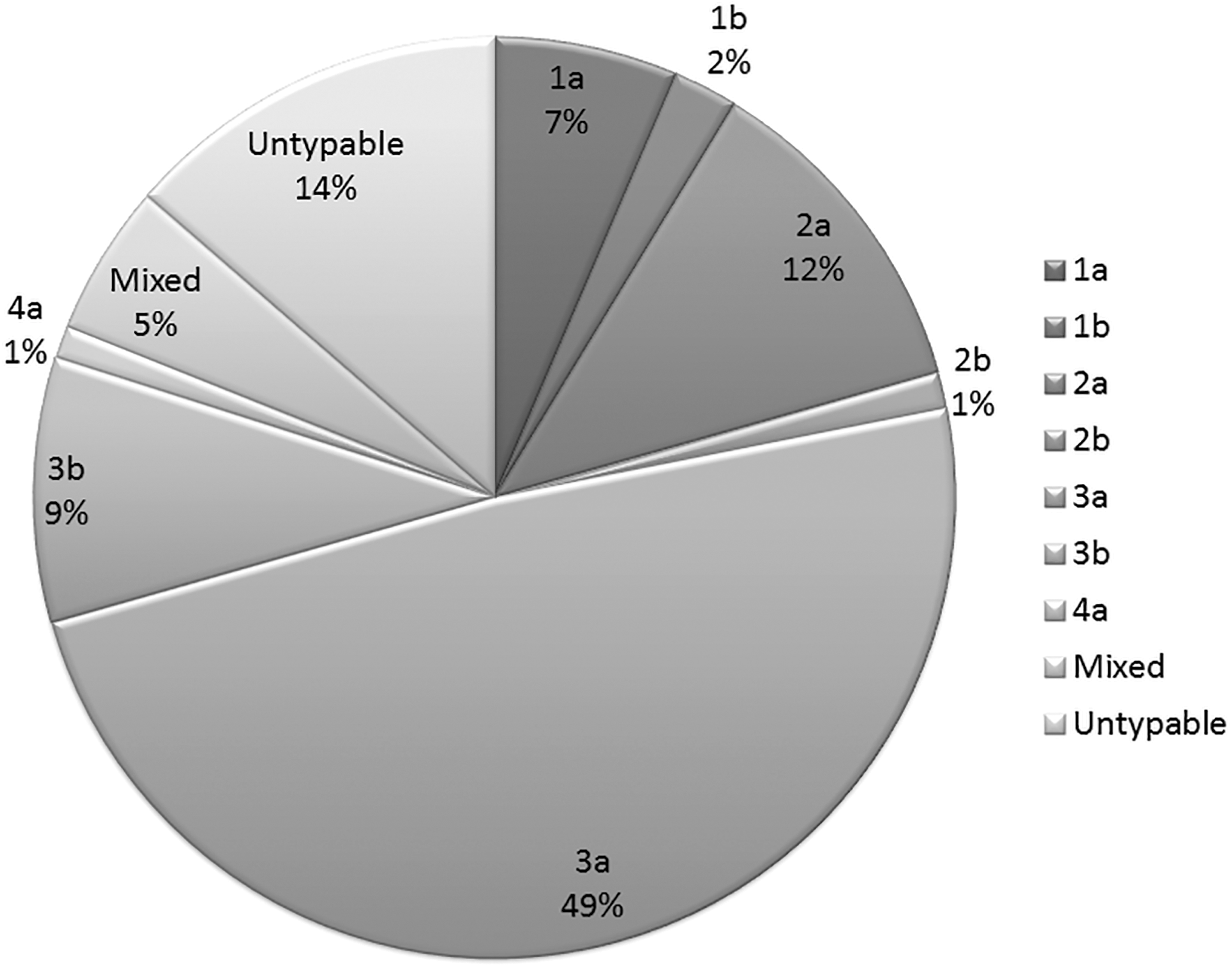
HCV genotype distribution in Khyber Pakhtunkhwa.
The data from Baluchistan province are very limited and there was only one study carried out in the year 2009. In this study, only 28 HCV-positive samples were genotyped. Study revealed that the highest number of patients were infected with genotype 3a (50%), followed by the unidentifiable genotypes (32%), and the frequency of two other genotypes 3b and 1a was 11% and 7%, respectively, as shown in Figure 6.
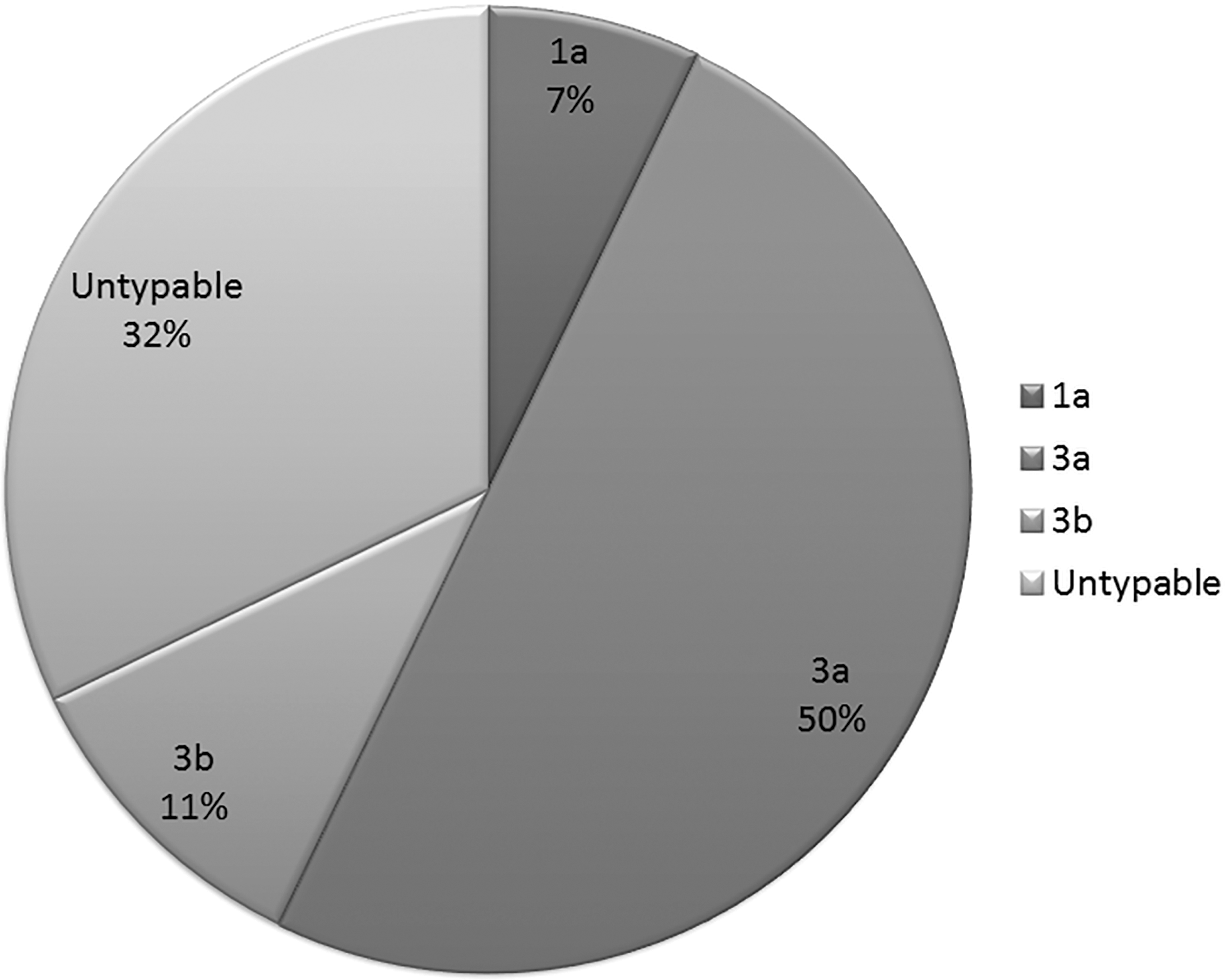
HCV genotype distribution in Baluchistan.
In Azad Jammu and Kashmir (AJK), HCV genotype 3a is predominant, accounting 59%. Other genotypes following 3a were 3b (19%), 1b (7%), 1a (7%), and 2a (4%). Unidentified genotype was found to be only 4%, whereas infections with genotype 4, 5, and 6 were not found in AJK region of Pakistan, as illustrated in Figure 7.
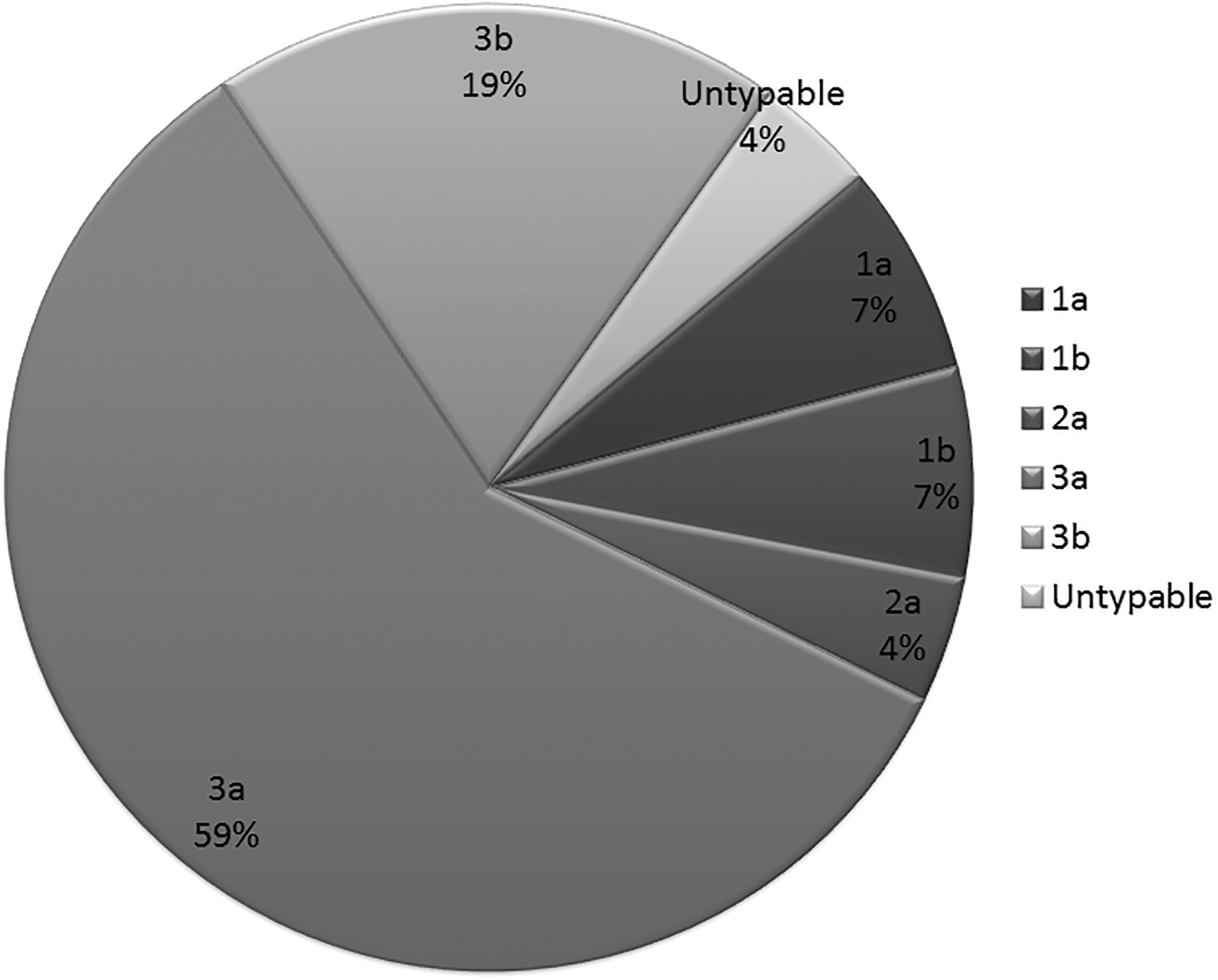
HCV genotype distribution in Azad Jammu and Kashmir.
In all the provinces of Pakistan, genotype 3a emerged as the most prevalent genotype (80.23%, 61%, 59%, 49%, and 50% in Punjab, Sindh, AJK, KPK, and Baluchistan, respectively). The second most prevalent frequency was of untypable genotype (32%, 21%, and 14% in Baluchistan, Sindh, and KPK, respectively); in contrast, only 4.91% and 4% samples from Punjab and AJK were untypable.
Discussion
It is estimated that ∼6% of population of Pakistan is infected with HCV (48). For the management of incidence of increasing HCV infections, epidemiological studies that accurately depict the prevalence of HCV infection and the geographic distribution of HCV genotypes are crucial. These studies help us strengthen the preventive and therapeutic strategies.
In this study, 3,539 HCV-infected patients were genotyped from all over Punjab. HCV genotype 3a is the most prevalent in Punjab population, as noticed in this analysis and previous studies (9,21,47). The frequency of genotype 2a-infected patients was found to be decreasing and the frequency of the patients infected with unidentifiable genotype was increasing. Genotype 1a and 3b were also prominent in all the studies published till now.
The data assembled and compiled from previous publications about HCV distribution pattern in Pakistan from year 2009 to 2018 allowed us to demonstrate the pattern of HCV genotype infections. Predominance of genotype 3a was observed in this study and the studies conducted in past from Pakistan. Other genotypes following the genotype 3a were untypable and 3b. The genotype frequency pattern illustrated in our study was almost similar to the results published by Butt et al. and Umer Mand Iqbal (26,73); some differences might be due to geographical differences. The analysis conducted by Khan was somehow in contrast with our study, which showed genotype 2a as second most prevalent genotype, whereas in our study, untypable was the most prevalent after genotype 3a (44). It was observed that the incidence of genotype 3a, untypable, and 3b is increasing in Pakistan, with decrease in the incidence of genotype 2a, 2b, and 1a.
Very limited data were available about the genotyping in Baluchistan province. The results in this study were comparable with the study conducted in 2009, which showed high prevalence of 1a and 2a, but according to our analysis, 3a and untypable were the most prevalent (37). The difference in results might be due to less sample size; so, there is need to conduct more systematic and synchronized genotyping in Baluchistan province of Pakistan.
In all previous studies (3,13,14,46) and this study, 3a and unclassified genotype are predominant in KPK province. The results reported by Kumar et al. showed that infections with 2a (4.1%) are rare compared to our analysis; frequency of genotype 2a is 12%. Latest study from 2017 demonstrates an increase in the incidence of mixed genotypes and 1a, which is in contrast with the results of this study (48).
All previous studies correspond well with this analysis, at a point that 3a is most prevalent in Punjab Province (2,9,20,21). Results of this study showed high frequency of 1a, whereas results published by Aziz et al. (20,21) observed comparatively less frequency. 2a and 1b are less frequent in Punjab province according to this study and past studies. Prevalence of untypable genotype in Punjab is very less compared to other provinces.
HCV genotyping data of Sindhi patients published in 2014 resemble our findings (12). These analyses demonstrate 3a as most prevalent genotype, followed by untypable, 3b, and 1a in decreasing order (12,24). Conclusions drawn by Shaikh et al. were in contrast with the analysis in this study, which showed 3a (50.8%) as most prevalent, and exceptionally high frequency of untypable (47%) was observed, followed by 2a (1.6%). All other genotypes were not seen in a total of 120 sample size (68).
The main purpose of HCV therapy is to prevent disease progression, liver cirrhosis, morbidity, and mortality (32). The quality of life of an HCV-infected patient can be improved by selecting a therapy that efficiently eradicates viral RNA from body, achieving high sustained virologic response (SVR), with minimal adverse effects (34). Patient's age, ethnicity, viral load, rapid virologic response (RVR), and viral genotype are the predictive factors for the selection of therapy type and duration (29,76). Genotype identification before treatment is crucial/decisive as treatment of HCV is purely genotype dependent (27).
The traditional HCV treatment supported the use of standard IFN and PEG-IFN (PEG-IFN alpha 2a or 2b) as a monotherapy or in combination with ribavirin. As Pakistan is a developing country with low health budget, standard IFN with ribavirin was preferred due to its low cost compared to PEG-IFN (28,36). Crespo et al. observed that patients treated with IFN achieved SVR of 53%, but with PEG-IFN, higher SVR of 78% was observed (30). Idrees and Riazuddin showed that in Pakistan, end-of-treatment response (ETR) is 67% when treated with ribavirin plus IFN (38). SVR of 77% was observed, whereas 23% patient relapsed after the completion of treatment (25). Although antiviral treatments have appreciable SVR rates, it results in several complications. Patients treated with IFN were observed to be suffering from anxiety, depression, and acute psychosis (53), whereas with PEG-IFN, headache, nausea, insomnia, myalgia, and weakness was commonly reported (38). Most common adverse effect of ribavirin noticed was hemolytic anemia, loss of appetite, and indigestion (51,56). Few years back, IFN plus ribavirin with treatment efficacy of 50–81% SVR was the only choice for HCV treatment, despite its detrimental effects.
New advancements about the HCV life cycle and viral enzymes have led to the development of DAA (17,33). Sofosbuvir is a nucleotide analogue that acts by inhibiting NS5B polymerase (49). It is a potential drug for curing and limiting the spread of viral infections with an SVR of 80–95% (77). Reports published in 2017 have shown exceptionally good results, yielding RVR, ETR, and SVR of 99.5%, 99%, and 98.5%, respectively (69).
The strongest prognostic aspect of the treatment response and efficacy is the genotype of viral HCV. Determination of genotype before selection of a therapy type and duration is necessary, as therapy response is genotype dependent (59). Study conducted by Idrees and Riazuddin (38) concluded the results of SVR achieved when patients of different genotypes were treated with IFN plus Ribavirin. Patients infected with HCV genotype 2 achieved highest SVR of 69.7%, followed by genotype 3 (57.3%); however, genotype 1 achieved lowest SVR of 24.2% (38). Lam et al. reported that genotype 3 has lower SVR rate (84%) than genotype 2 (94%), when treated with SOF, Sofosbuvir - NS5B inhibitor plus RVR for 24 and 12 weeks, respectively (49). Another study reported the comparison of SVR achieved in patients of genotype 3 and 2 (56% and 97%, respectively), when treated with sofosbuvir (65).
Conclusion
In Pakistan, HCV disease burden is escalating very rapidly, infecting almost 6% (10 million) of population. This study highlights the HCV genotype distribution pattern in different regions of Pakistan. There were no data available from Gilgit Province and very limited data were available from Baluchistan; so there is a need for more systemized analysis of genotype distribution in these provinces. Genotype determination is crucial for viral eradication and therapy response. For disease management, there is a need to design a treatment achieving high SVR with minimal adverse effects. In Pakistan, the most prevalent genotype is 3a, followed by untypable genotype. Both IFN and sofosbuvir yield good SVR against genotype 3a, but treatment with sofosbuvir has comparatively high SVR, less adverse effects, and more tolerability.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There is no role of any funding agency related to this study.