
Abstract
Chikungunya fever is a re-emerging viral disease caused by chikungunya virus (CHIKV). The disease is generally self-limiting, but chronic arthralgia/arthritis may persist for months or years. We evaluated the expression of 12 cytokines/chemokines and matrix metalloproteinases (MMP)-1 and MMP-3 using enzyme-linked immunosorbent assays (ELISAs) and compared among patients who still had arthralgia (persistent arthralgia), patients who had fully recovered, and healthy controls. There was a significant increase in interleukin (IL)-1β, IL-6, IL-8, monocyte chemotactic protein-1 (MCP-1), MMP-1, and MMP-3 levels in patients with persistent arthralgia in comparison to healthy controls (p < 0.05) and a significant increase in tumor necrosis factor-alpha (TNF-α), MMP-1, and MMP-3 levels in patients with persistent arthralgia in comparison to patients who had fully recovered (p < 0.05). Interferon (IFN)-γ, IL-6, and transforming growth factor beta (TGF-β) levels tended to be increased in patients with chronic CHIKV-induced arthritis compared with fully recovered. TNF-α, IL-12, and MCP-1 levels were elevated (p < 0.05), whereas regulated on activation, normal T cell expressed and secreted (RANTES) levels were decreased in patients with severe pain compared with patients with nonsevere pain (p < 0.05). IFN-γ, IL-1β, IL-6, and IL-8 levels tended to be elevated in patients with severe pain compared with patients with nonsevere pain. We proposed a role played by TNF-α, IL-6, IL-8, and MCP-1 in persistent arthralgia or chronic disease through the activation of MMP-1 and MMP-3. The increase in TNF-α, IL-12, and MCP-1 levels (and the tendency toward an increase in IFN-γ, IL-1β, IL-6, and IL-8 levels) in patients with severe pain compared with patients with nonsevere pain suggests the role of these inflammatory markers in chronic disease and severity of the disease.
Introduction
Chikungunya fever is a re-emerging viral disease caused by chikungunya virus (CHIKV), which is a mosquito-borne arthritogenic alphavirus (12,48). In 2008–2009, an outbreak occurred in Southern Thailand. By December 2009, it had spread to other parts of the country and affected more than 52,000 people (39). The typical symptoms of acute CHIKV fever are high fever, severe polyarthralgia, myalgia, and fatigue (1,2,12,42). Arthralgia mainly affects the wrist, knee, ankle, and small joints of the hands but can also affect the large joints (46,53). Other symptoms include skin rash and headache (1,14). The disease is generally self-limiting. Most symptoms disappear within several weeks (9), but chronic arthralgia/arthritis may persist for months or years (4,7,9,16,23,30,51,52,56). The symptoms in the chronic phase include arthralgia, myalgia, and weakness (16,28,37,40,50,51,55). Long-term arthralgia is typically polyarthralgia (1,16,40,50). The population of patients suffering from musculoskeletal disorders varies among studies. Some studies reported that ∼60% of patients are affected until 12–36 months after acute illness (16,30,37,40,50,51), whereas other studies of the Indian epidemic in 2006 showed that 4.1% and 1.6% of patients suffered from persistent rheumatic pain 1 and 2 years after acute infection, respectively (9).
The long-term consequences of CHIKV infection have been systematically reviewed. The most frequent problems are persistent arthralgia, arthritis, hair loss, and depression (54). Postchikungunya chronic inflammatory rheumatism is characterized by polyarthralgia, morning stiffness, joint edema, and joint redness (11,49). A systematic review and meta-analysis that estimated the prevalence of chronic articular pain and arthritis after chikungunya fever in the Americas based on 41 articles suggested that 52% of CHIKV-infected patients will present chronic articular symptoms, even if high heterogeneity between studies is found (15). Another systematic review and meta-analysis of 34 studies that estimated the proportion of patients who did not recover based on the virus genotype and the time of disease onset reported that the overall no recovery rate was 43% (95% CI: 35–52%) after 3 months and 21% (95% CI: 19–22%) after 12 months of follow-up. The prevalence of CHIKV-associated chronic discomfort varies by virus lineage, with the highest prevalence of 50% (95% CI: 40–60%) resulting from the East Central South African (ECSA)-diverged genotype and a lower prevalence of 36% (95% CI: 20–52%) resulting from the Asian lineage genotype (45). Musculoskeletal disorders associated with CHIKV infection may persist for up to 6 years after acute illness (25,36). Unfortunately, while there are numerous reports of chronic CHIKV-induced arthralgia and/or arthritis, there is currently no demonstration of the mechanisms that link the initial CHIKV infection to the development of chronic arthralgia.
Immunologic factors seem to play important roles in the pathogenesis of CHIKV-associated illness during acute illness. A systematic review and meta-analysis of immune signatures in patients with acute CHIKV infection (1–10 days after illness onset) based on 14 cohort studies that were conducted during outbreaks across different geographic locations from 2008 to 2010 revealed that the following 20 cytokines/chemokines were significantly elevated in PCR-positive CHIKV-infected patients compared with healthy controls: the proinflammatory cytokines interferon (IFN)-α, IFN-γ, interleukin (IL)-2, IL-2R, IL-6, IL-7, IL-12, IL-15, IL-17, and IL-18; the anti-inflammatory cytokines IL-1Ra, IL-4, and IL-10; the chemokines G-CSF (granulocyte colony-stimulating factor), interferon gamma-induced protein 10 (IP-10), monocyte chemotactic protein-1 (MCP-1), monokine induced by gamma interferon (MIG), macrophage inflammatory protein (MIP) 1α, and MIP-1β; and the growth factor basic fibroblast growth factor (FGF-β) (53). In addition to the 20 immune mediators mentioned above, IL-1β was also elevated during acute CHIKV infection (42).
The precise mechanisms involved in chronic joint pathologies induced by CHIKV infection remain unclear. Potential causes of chronic CHIKV-induced arthritis have been proposed, including viral persistence, persistent immune responses, the induction of autoimmune disease, the exacerbation of the pre-existing joint disease, and/or direct effects of the virus (17,18,22). Arthralgia experienced by CHIKV fever patients are closely similar to the symptoms induced by some other arthritogenic alphaviruses (41). Such alphavirus infection promoted macrophage activation, leading to the release of macrophage migration inhibitory factor and inducing the secretion of tumor necrosis factor-alpha (TNF-α), IL-1β, and IL-6 (3). Production of these cytokines was followed by the expression of matrix metalloproteinases (MMPs) 1 and 3, which could be involved in the articular damage (3). In addition, there are remarkable similarities between macrophage responses induced by some arthritogenic alphaviruses (Sindbis virus [SINV]) infection and those observed in rheumatoid arthritis (RA), a condition which is characterized by severe joint pains due to inflammation and tissue destruction caused by inflammatory cytokines (3). In addition, other studies showed that a proportion of CHIKV-infected patients have joint manifestations closely resembling those of RA and described biological markers of joint damage in the CHIKV-induced arthritis patients (5,38). Thus, it is possible that the immunopathogenesis of chronic arthralgia after CHIKV infection have similarities to those arthritides and/or similar to the immunopathogenesis of RA.
This study focused on immunological factors. We evaluated the expression of 12 cytokines/chemokines and the MMP-1 and MMP-3 in patients who still had arthralgia 5 years after the 2008–2009 outbreak in Southern Thailand and compared the expression among patients who still had arthralgia (persistent arthralgia), those who were fully recovered, and healthy controls.
Patients and Methods
Study area and population
This study was conducted in CHIKV-infected patients with persistent articular manifestations 5 years after the acute phase of CHIKV fever in Nakhon Si Thammarat and Phatthalung provinces in southern Thailand, where clinically suspected or diagnosed cases were reported during the outbreak in 2008–2009. Participants were recruited from patients diagnosed or suspected to be infected with CHIKV in rural communities during the outbreak from a total of 35 villages in Nakhon Si Thammarat province and a total of 4 villages in Phatthalung province. In the context of the epidemic, patients had been suspected to be infected with CHIKV based on initial clinical symptoms, including high fever and severe polyarthralgia. Clinical data and blood samples were collected between April 2013 and September 2014, which ranged from 56 to 60 months after the outbreak. This study was approved by the Ethics Committee of Walailak University (WU: 031/2554), and written informed consent was obtained from all participants.
Selection criteria
All of the patients, confirmed or suspected to be infected with CHIKV, who still had CHIKV-related symptoms in each village surveyed, were invited to this study. The participants who had any history of chronic arthritis before the outbreak and who had a fever at any time between the day of the blood sample collection and the previous 7 days were excluded from the study.
Subjects were classified as having persistent arthralgia if they declared that they still had joint manifestations at the time of the interview or had experienced at least one relapse within the past 8 days (30). The joint manifestations included at least one of these symptoms: joint pain, joint swelling, or morning joint stiffness. The control subjects were (1) patients with suspected or confirmed CHIKV infection who no longer had chikungunya-related symptoms (full recovery) and (2) healthy volunteers who had no history of CHIKV fever (healthy control). The control subjects were systematically selected from the same villages or the same geographic zone as infected cases, and they were matched for sex, age, and comorbid conditions with persistent arthralgia and full recovery cases.
The patients with persistent arthralgia were subdivided according to their joint pain intensity into severe and nonsevere groups. The patients were classified as having severe pain if (1) their pain score was >6 at the time of the interview or the blood sample collection, (2) they suffered from joint pain accompanied by joint swelling (all cases who had joint swelling also reported a pain score >6), or (3) their pain score was >6 and they suffered from joint pain every day. The intensity of the joint pain was self-reported by the patients and quantified using a verbal numerical rating scale using numbers from 0 (no pain) to 10 (worst pain).
In a total of 35 villages in Nakhon Si Thammarat Province and a total of 4 villages in Phatthalung Province, approximately 5% of healthy controls remained in the population during the outbreak, 2–10 houses in each village surveyed. At the time of the interview and blood sample collection, nearly all of the patient population was fully recovered. A total of 63 patients with persistent arthralgia, 30 fully recovered patients, and 30 healthy controls were included in this study. Of the 63 patients with persistent arthralgia, 51 cases (80.9%) had severe joint pain, and 12 cases (19.05%) had nonsevere joint symptoms. A total of 30 fully recovered patients and 30 healthy controls, with sex, age, and comorbid conditions matched, were also included. Clinical data and blood samples were collected. The study population and number of cases identified are detailed in Figure 1.

The study population and the number of cases identified. *As calculated from the total number of patients identified.
Laboratory tests
Blood samples of 20–25 mL/person were collected from the participants. The sera were separated from the clotted blood and stored at −80°C until the serology study and the measurement of cytokine and enzyme levels.
The presence of CHIKV-specific immunoglobulin G antibodies in serum
The sera of patients and healthy controls were collected and examined for the presence of anti-CHIKV immunoglobulin G (IgG) antibody using an indirect immunofluorescence technique (IIFT) with a commercial kit (Euroimmun Anti-CHIKV IIFT, Euroimmun, Germany) according to the manufacturer's protocols and as described previously (24,32,47). Briefly, the patients' sera were diluted 1:10 in phosphate-buffered saline (PBS), and 20 μL of the diluted sera was transferred into the reaction field of a reagent tray. A slide containing mounted glass biochips coated with CHIKV (strain EU-14)-infected Vero cells or uninfected Vero cells was then placed into the recesses of the reaction tray, which allowed all biochips to come into contact with the sera. After incubation for 30 min at room temperature, the slide was then washed three times with PBS containing 0.05% Tween 20. Following washing, the slide was placed into a reagent tray reaction field containing fluorescein isothiocyanate-conjugated goat anti-human IgG (Euroimmun, Germany) diluted to the working concentration in PBS. After 30 min of incubation, the slide was washed and mounted. A coverslip was added, and the slide was examined for fluorescence using a fluorescence microscope (Olympus); titers of ≥1:10 were considered positive. A positive reaction was indicated by a homogeneous to granular pattern of fluorescence in the cytoplasm of CHIKV-infected Vero cells and no fluorescence in uninfected Vero cells.
Cytokine and enzyme measurements by ELISA
The concentrations of the cytokines, chemokines, and enzymes (IFN-γ, TNF-α, IL-1β, IL-4, IL-6, IL-8, IL-10, IL-12, IL-17, TGF-β, MCP-1[CCL2], RANTES [CCL5], MMP-1, and MMP-3) in serum samples from each group were investigated using commercial ELISA Kits according to the manufacturer's instructions. The ELISA Kits used to measure IFN-γ, TNF-α, IL-1β, IL-4, IL-6, IL-8, IL-10, IL-12, IL-17, and MCP-1 were purchased from BD Biosciences Pharmingen. The ELISA Kits used to measure TGF-β, MMP-1, MMP-3, and RANTES were purchased from R&D Systems. The assay was based on a double-antibody sandwich ELISA technique. Briefly, the capture antibody was coated onto the microplate overnight. After the aspiration and washing steps, the standards and the samples were added to the microplate and incubated, which allowed the cytokines in the serum to bind to the capture antibody. Unbound molecules were then removed by aspirating and washing steps. The detection antibody combined with streptavidin/horseradish peroxidase was subsequently added to each well and incubated. After aspirating and washing away the unbound molecules, the substrate solutions were added to each well. The amount of colored product was formed in proportion to the amount of cytokine present in the serum. The reaction was terminated by the addition of sulfuric acid. The concentration of the cytokine in the serum was then analyzed by comparing the absorbance of the test samples to the standard curve. Each serum sample was measured in duplicate. The cytokine levels in sera were reported as pg/mL.
Statistical analysis
The results were expressed as the mean ± standard error, or median with interquartile (25th and 75th) according to data distribution. Data were analyzed using SPSS 17.0 (SPSS, Inc., Chicago, IL). The statistical comparisons were analyzed using an independent t-test or one-way ANOVA for continuous data with a normal distribution or a Mann–Whitney U or Kruskal–Wallis test for continuous data with the non-normal distribution. Differences were considered statistically significant when p < 0.05.
Results
The presence of CHIKV-specific IgG antibody in serum of the participants
For the serological follow-up in patients, of the 93 suspected and confirmed cases, 80 cases (86.0%) were positive for anti-CHIKV IgG antibody up to 60 months after CHIKV infection. Anti-CHIKV IgG antibody could be detected in both the persistent arthralgia and full recovery groups, and there was no significant difference in persistence between these two groups. The number of patients with positive serology at 5 years postoutbreak is detailed in Table 1. Healthy controls are people who had no history of CHIKV fever and negative for anti-CHIKV IgG antibody.
The Number of Subjects with Positive Serology for Anti-Chikungunya Virus Immunoglobulin G Antibody at 5 Years Postoutbreak
The cutoff point was at an antibody dilution of 1:10.
CHIKV, chikungunya virus; IgG, immunoglobulin G.
Levels of cytokines/chemokines in serum
The levels of cytokines/chemokines, MMP-1, and MMP-3 in serum were measured using ELISA and compared among patients who still had arthralgia (persistent arthralgia), patients who had fully recovered, and healthy controls. There was a significant increase in the IL-1β, IL-6, IL-8, and MCP-1 levels in patients with chronic CHIKV-induced arthritis compared with those in healthy controls. There was a significant increase in the TNF-α levels in patients with chronic CHIKV-induced arthritis compared with those in patients who had fully recovered. There was a significant increase in the TNF-α, IL-1β, IL-8, and MCP-1 levels in the full recovery group compared with the healthy control group. There was no difference in the IL-4, IL-10, IL-12, IL-17A, and RANTES levels among the three groups. The IFN-γ and TGF-β levels tended to be increased in patients with chronic CHIKV-induced arthritis compared with those in fully recovered (Tables 2 and 3 and Figs. 2 and 3).
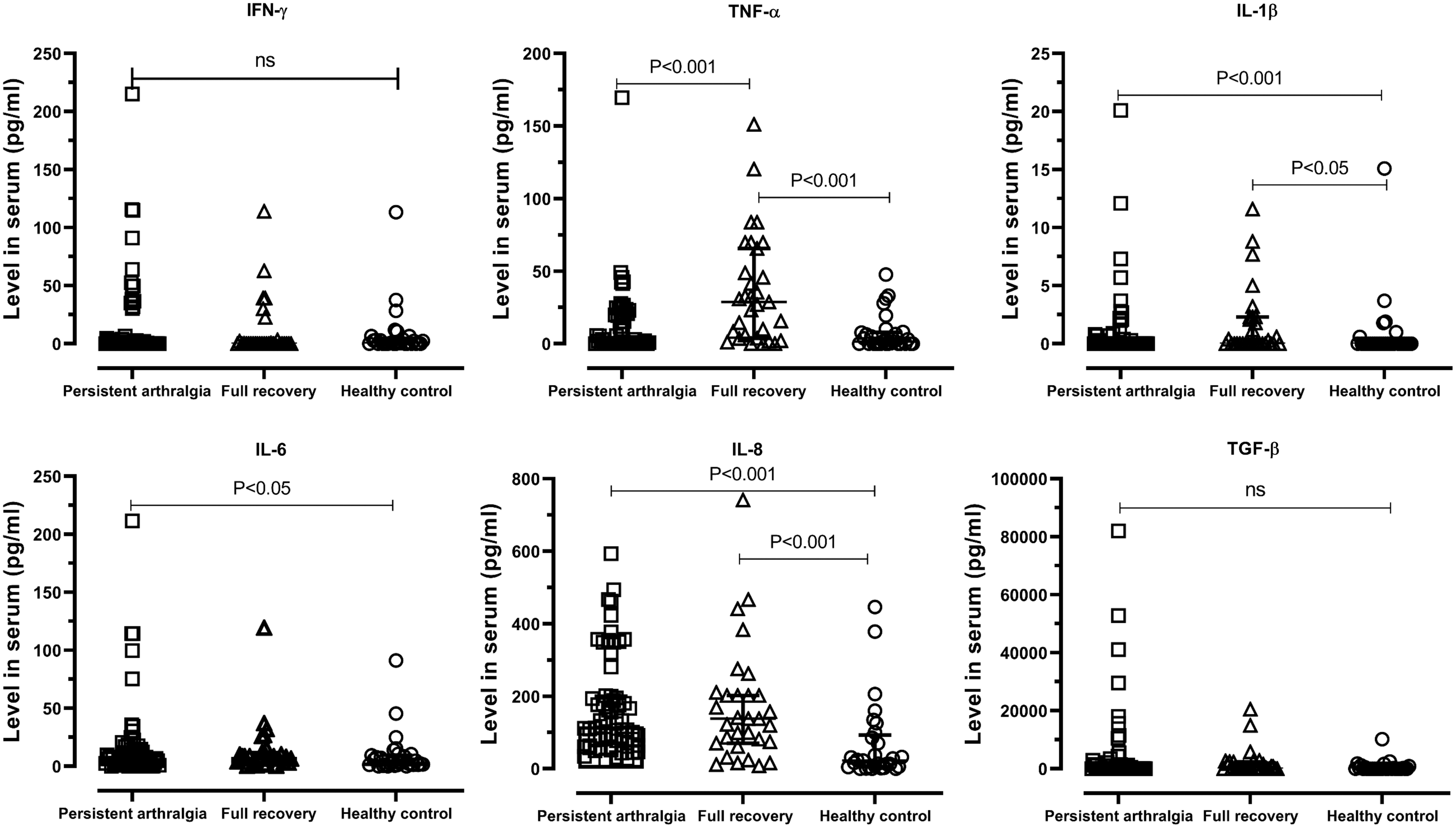
Levels of IFN-γ, TNF-α, IL-1β, IL-6, IL-8, and TGF-β in serum. Persistent arthralgia (n = 63); full recovery (n = 30); healthy control (n = 30). IFN-γ, interferon-gamma; IL, interleukin; TNF-α, tumor necrosis factor-alpha; TNF-β, transforming growth factor-beta.
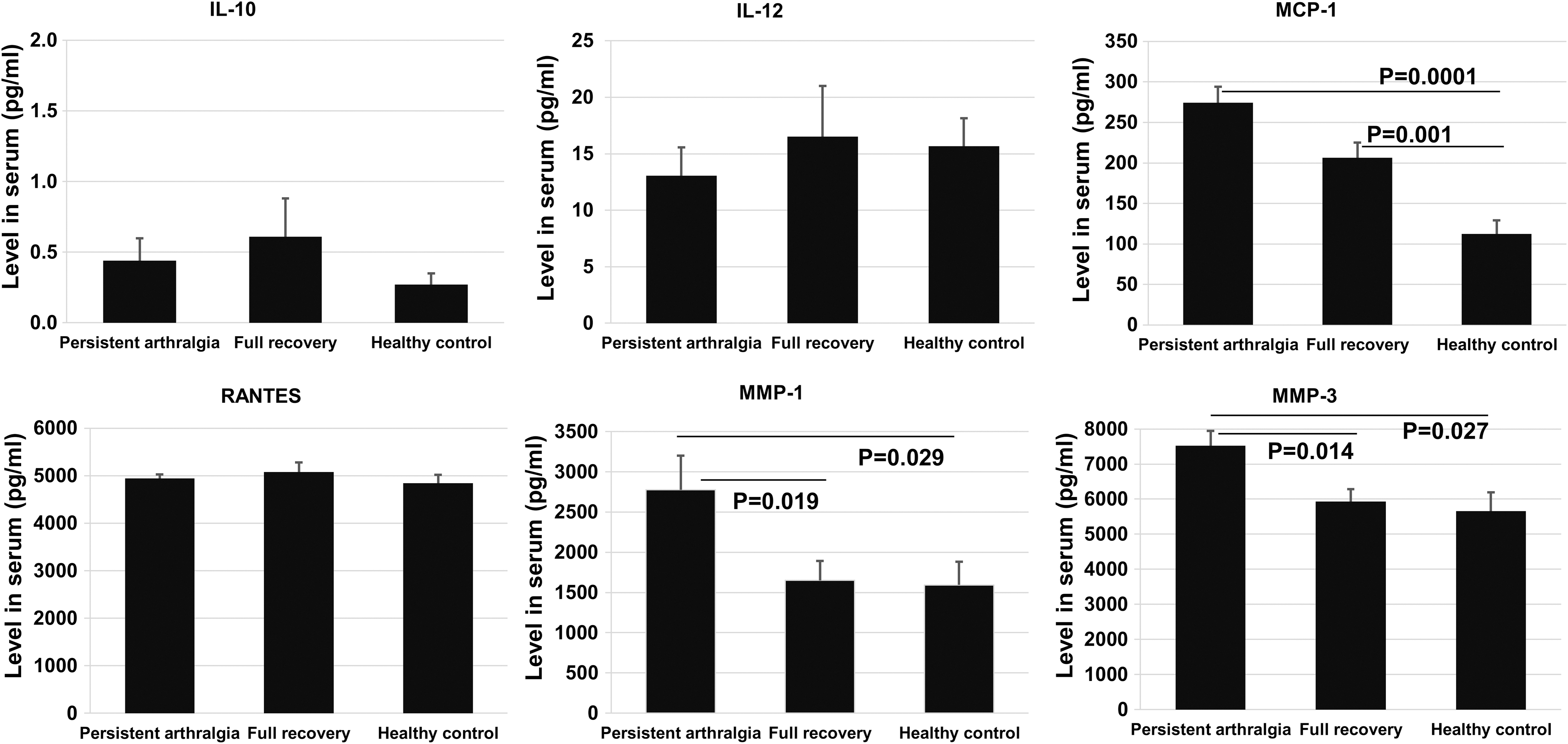
Levels of IL-10, IL-12, RANTES, MCP-1, MMP-1, and MMP-3 in serum. Persistent arthralgia (n = 50–63); full recovery (n = 25–30); healthy control (n = 20–30). MCP-1, monocyte chemotactic protein-1; MMP, matrix metalloproteinases; RANTES, regulated on activation, normal T cell expressed and secreted.
Level of Cytokines in Serum
Data were expressed as median (IQR) and analyzed using a Mann–Whitney U or Kruskal–Wallis test. The mean difference is significant at the 0.05 level.
IFN-γ, Interferon-gamma; IL, interleukin; IQR, interquartile range; ns, not significant; TNF-α, tumor necrosis factor-alpha; TNF-β, transforming growth factor-beta.
Level of Cytokines and Enzymes in Serum
Data were expressed as mean ± SE and analyzed using independent t-test or one-way ANOVA test. The mean difference is significant at the 0.05 level.
MCP-1, monocyte chemotactic protein-1; MMP, matrix metalloproteinases; RANTES, regulated on activation, normal T cell expressed and secreted; SE, standard error.
The persistent arthralgia patients were then further subdivided into severe and nonsevere and compared. TNF-α, IL-12, and MCP-1 were elevated, whereas RANTES were decreased in patients with severe pain compared with those with nonsevere pain. IFN-γ, IL-1β, IL-6, and IL-8 tended to be elevated in patients with severe pain compared with those with nonsevere pain. The level of TGF-β tended to be increased in patients with nonsevere pain compared with patients with severe pain (Table 4 and Figs. 4 and 5).
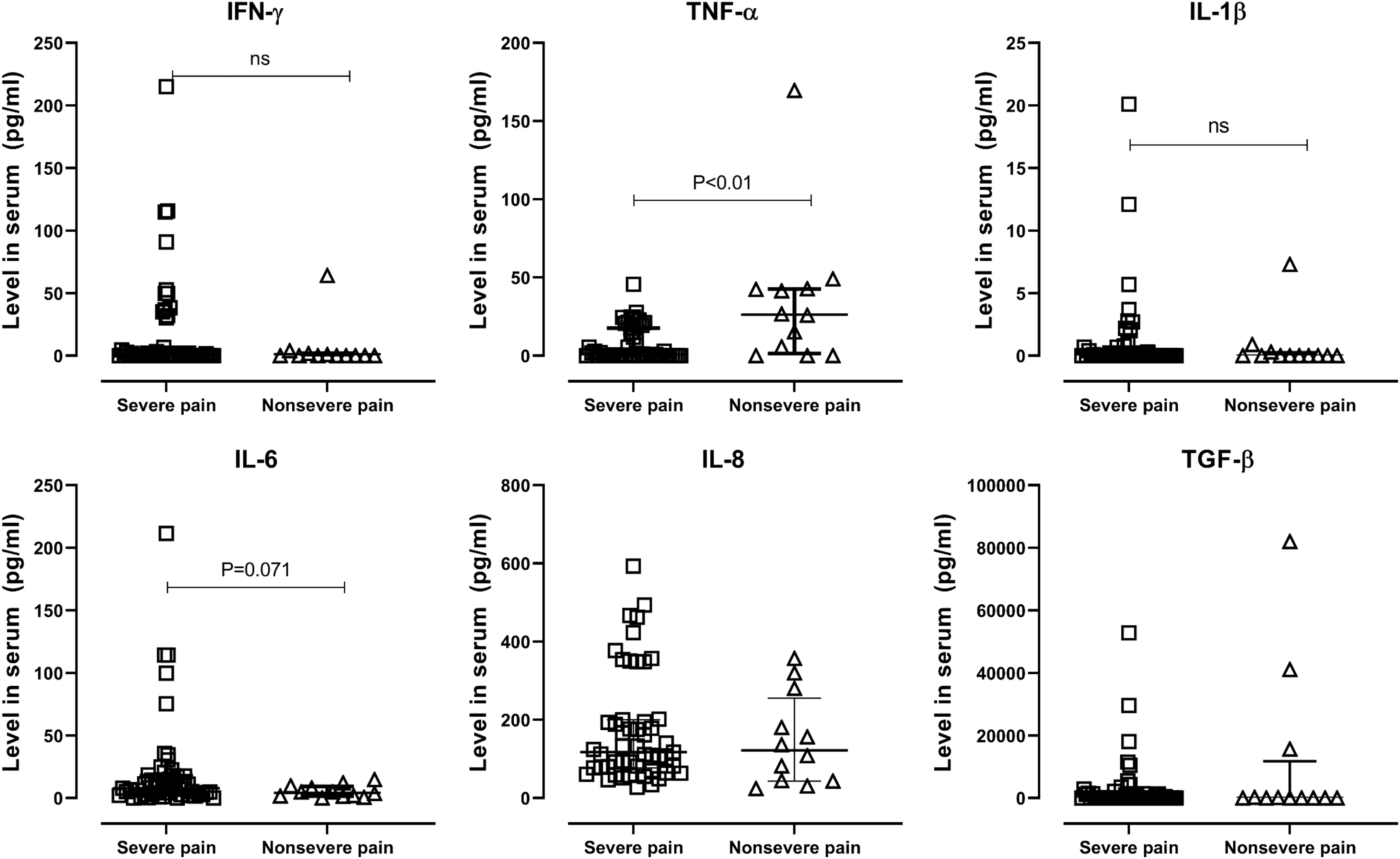
Levels of IFN-γ, TNF-α, IL-1β, IL-6, IL-8, and TGF-β in serum obtained from patients with severe and nonsevere pain. Severe pain (n = 51); nonsevere pain (n = 12).
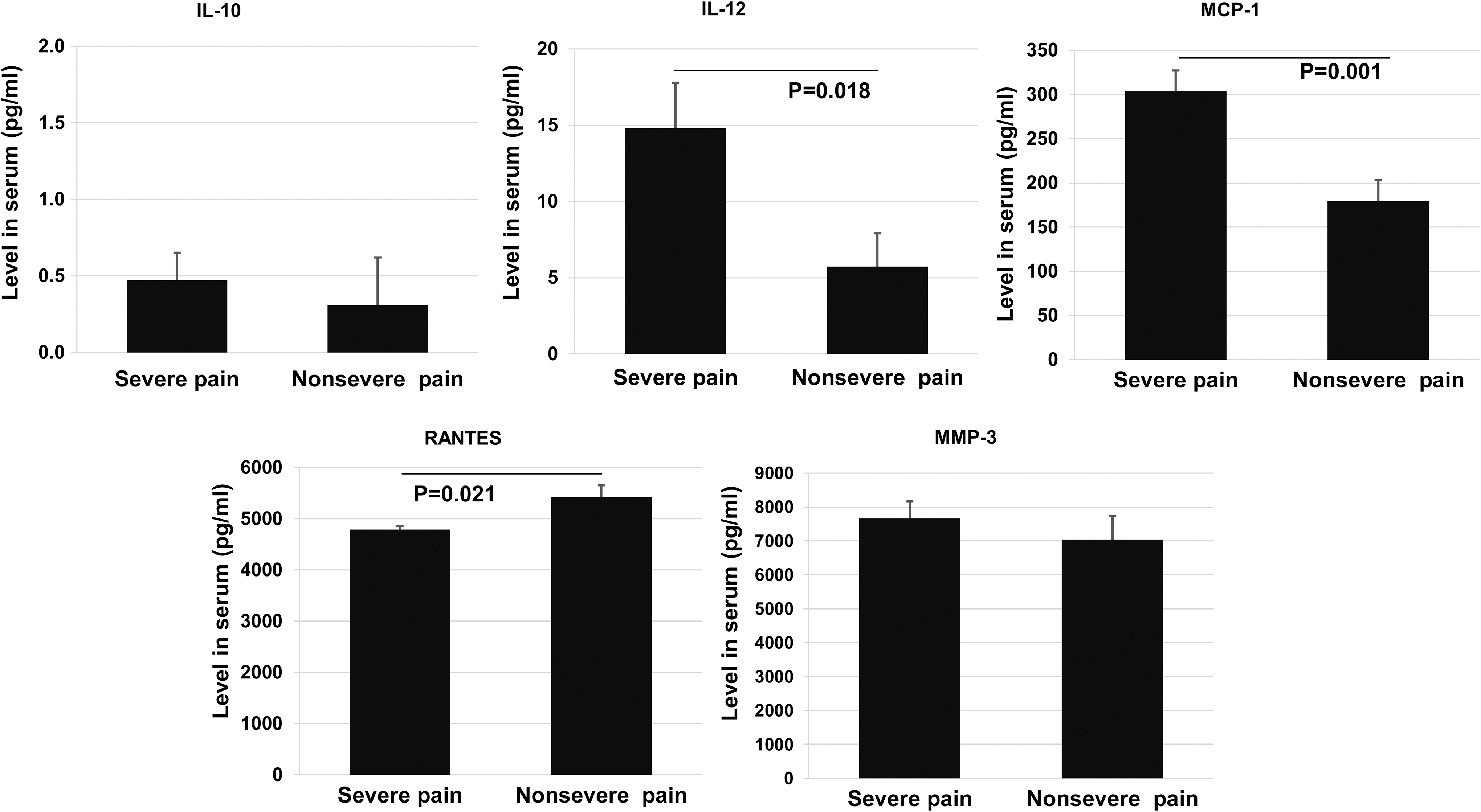
Levels of IL-10, IL-12, MCP-1, RANTES, and MMP-3 in serum obtained from patients with severe and nonsevere pain. Severe pain (n = 38–51); nonsevere pain (n = 12).
Comparison of Cytokine Levels in Serum Obtained from Patients with Severe and Nonsevere Pain
The mean difference is significant at the 0.05 level.
Data were expressed as median (IQR) and analyzed using a Mann–Whitney U test.
Data were expressed as mean ± SE and analyzed using independent t-test.
Levels of MMP-1 and MMP-3 in serum
There was a significant increase in the MMP-1 and MMP-3 levels in patients with chronic CHIKV-induced arthritis compared with those in healthy controls. There was a significant increase in the MMP-1 and MMP-3 levels in patients with chronic CHIKV-induced arthritis compared with those in patients who had fully recovered (Table 3 and Fig. 4).
Discussion
It seems that persistent immune responses may cause chronic arthritis or arthralgia after CHIKV infection. Numerous cytokines are produced during acute CHIKV infection, including the proinflammatory cytokines (IFN-α, IFN-γ, IL-1β, IL-2, IL-2R, IL-6, IL-7, IL-12, IL-15, IL-17, and IL-18); the anti-inflammatory cytokines (IL-1Ra, IL-4, and IL-10); and the chemokines (G-CSF, IP-10, MCP-1, MIG, MIP-1α, MIP-1β; and FGF-β) (42,53). Of these cytokines, many remain elevated during persistent long-term arthralgia/arthritis (6,9,10,22,26,34). Studies of cytokines involved in chronic arthritis/arthralgia associated with CHIKV infection revealed that the level of IL-6 in serum remained elevated in chronic CHIKV-infected patients 2 years after CHIKV infection (9). IL-17 became detectable as the disease progressed to the chronic phase of CHIKV illness (10), and patients with persistent arthralgia had higher levels of IL-6 and granulocyte/macrophage colony-stimulating factor (GM-CSF) (10). The elevation in TNF-α, IL-1β, IL-6, IL-8, and IL-10 levels was reported in patients who developed progressive erosive arthritis over 24 months after CHIKV infection (34). The elevation of MCP-1, IL-6, IL-8, MIP-1α, and MIP-1β levels was also found in the chronic phase after CHIKV infection (6). The levels of IFN-γ, TNF-α, IL-1β, IL-5, IL-10, and IL-12, which were low in the acute phase in CHIKV patients, were significantly elevated at later time points 6 and 12 months after CHIKV infection (26). IL-12 was elevated in serum starting from the first day of clinical acute infection, and its level remained dramatically elevated for months in chronically CHIKV-infected patients but not in acutely infected or recovered patients (26). Moreover, Hoarau et al. (22) provided evidence of an association between the persistent presence of CHIKV antigen in synovial tissues and the high levels of MCP-1, IL-6, and IL-8 in synovial fluid and the resulting cytopathic effects in synovial tissue in a patient with chronic arthralgia after 18 months of CHIKV infection (22). In this study, patients with persistent arthralgia showed significantly increased production of IL-1β, IL-6, IL-8, MCP-1, MMP-1, and MMP-3 in comparison to healthy controls and significantly increased production of TNF-α, MMP-1, and MMP-3 compared with fully recovered patients. IFN-γ, IL-6, and TGF-β tended to be increased in patients with chronic CHIKV-induced arthritis compared with fully recovered. IL-4, IL-10, and IL-17A were expressed at very low concentrations, and the levels showed no differences among the groups. Overall, it is likely that TNF-α, IL-1β, IL-6, IL-8, MCP-1, MMP-1, and MMP-3 are increased during the chronic stages of the disease. This finding and those of future studies may link acute infection to persistent arthritis/arthralgia or chronic disease (6,22,26,34).
IFN-γ is a major cytokine secreted by T helper 1 (Th1) cells. In addition to IFN-γ, Th1 cells produce IL-2 and IL-12 but not IL-4. TNF-α, IL-4, and IL-10 are markers of Th2 cells. The secretion of IL-17A defines Th17 cells (20). The expression of IL-12 drives the development of the Th-1 subset of T cells that produce IFN-γ (20). Our study showed a significant increase in IL-1β, IL-6, IL-8, MCP-1, MMP-1, and MMP-3 levels in patients with persistent arthralgia compared with healthy controls and a significant increase in TNF-α, IL-12, and MCP-1 in the severe pain group compared with the nonsevere pain group. This finding suggests the prominent role of Th1 cells, but not Th2 and/or Th17 cells, in persistent arthralgia/arthritis induced by CHIKV infection. It has been postulated that chronic arthralgia/arthritis induced by CHIKV infection is a Th1-driven disease and does not involve Th2 or Th17 cells (22). It was reported that IL-12 was elevated starting from the first day of clinical acute infection and its level remained dramatically elevated for months only in the chronic group; IL-12 decreased to the background level starting at day 15 in the recovered group, whereas IL-4, IL-10, and IL-13 (Th2 cytokines) were expressed at very low levels in CHIKV-infected patients (22). Chirathaworn et al. also suggested that the involvement of the Th1 response in CHIKV infection was mediated by IL-18 production; IL-18 and IL-18 BP levels were higher in both acute and convalescent patients compared with control patients (8).
TNF-α, IL-1, and IL-6 are produced by immune cells as signals of inflammation, especially by macrophages and T cells. TNF-α is one of the most potent osteoclastogenic cytokines, and its role in arthritic outcomes is generally known. TNF-α has been shown to upregulate MCP-1 (CCL2), a major chemoattractant for monocytes/macrophages, expression (25). MCP-1 is one of the key chemokines that is upregulated at sites of infection, and it regulates the migration and infiltration of monocytes, memory T lymphocytes, and natural killer (NK) cells (13). Higher production of this mediator might indicate the involvement of macrophages and Th1 cells in persistent joint inflammation in CHIKV-induced arthritis. There was evidence of the increased expression of TNF-α and an increase in IFN-γ-secreting NK-like T cells (CD56+ CD3+ cells) in chronic chikungunya-induced arthritis patients compared with controls (54), and the presence of infiltrating macrophages, NK, and T cells (CD4+ but rare cytotoxic CD8) in synovial tissue, and CHIKV (RNA and proteins) in perivascular synovial macrophages in a patient with chronic arthralgia 18 months post-CHIKV infection was demonstrated (22). Overall, this finding showed that Th1 cytokines and their downstream cytokines were elevated in patients with chronic arthralgia/arthritis, indicating that Th1 cells and macrophages play a major role in the pathogenesis of chronic arthritis after CHIKV infection. Furthermore, in the current study IL-4, IL-10, and IL-17A were expressed at very low concentrations, and their levels were not different among the groups. Again, cytokines IL-4, IL-10, and IL-17A are not upregulated emphasizing the role of Th1 cells and macrophages.
The macrophage tissue tropism and local viral persistence are thought to be involved in the establishment of chronic disease after CHIKV infection (14,21). It has been reported that CHIKV (RNA and proteins) was found in perivascular synovial macrophages in one chronic patient 18 months postinfection (19). Macrophages are the main cellular reservoirs of CHIKV infection in vivo (21,29,44). However, to support that the persistent arthralgia in these patients were caused by persistent CHIKV infection of macrophages, which in turn may contribute to secreting most of these proinflammatory mediators in chronic disease, further studies remain to be done.
The cytokine profile related to disease severity during acute CHIKV infection seems to be similar to that related to chronic CHIKV infection. Studies of biomarkers of disease severity during acute CHIKV infection have reported that an increase in IL-1β and IL-6 and a decrease in RANTES in peripheral blood were correlated with disease severity (22,42). Another report showed an association between disease severity and CXCL9/MIG, CXCL10/IP-10, and IgG levels in the acute phase of CHIKV infection (26). In this study, when patients with severe and nonsevere pain were compared, TNF-α, IL-12, and MCP-1 were elevated and RANTES were decreased in patients with severe pain compared with patients with nonsevere pain. IFN-γ, IL-1β, IL-6, and IL-8 tended to be elevated in patients with severe pain compared with those with nonsevere pain, and these results suggest the role of these inflammatory markers in chronic disease and severity of the disease.
The level of TGF-β tended to be increased in patients with nonsevere pain compared with those with severe pain. TGF-β, which is an anti-inflammatory cytokine, is a potent suppressor of T cell activation and can decrease T cell proliferation and cytokine production. A slight increase in TGF-β in chronic CHIKV-induced arthritis, especially in patients with nonsevere pain, might indicate the presence of an anti-inflammatory response in nonsevere pain patients that reduces inflammation in these patients compared with those with severe pain.
MMPs, which are enzymes that fragment matrix collagen, are thought to have a role in cartilage destruction and the progression of osteoarthritis (43). Evidence of cartilage and bone damage has been reported in CHIKV-infected patients (34,35). IFN-γ and TNF-α enhanced the production of many other proinflammatory mediators, such as IL-6 and IL-8 (43). The induction of IL-6 production by IFN-γ and TNF-α in human articular chondrocytes has been reported (19). IL-6 increases the production of cartilage-destructive enzymes (MMP-3 and MMP-9) and the expression of bone destruction-related molecules, such as NF-kappa-β ligand (RANKL) (27,31). IL-1β and TNF-α induce abundant secretion of IL-8 from human articular chondrocytes (33) and upregulate the production of MMP-1 and MMP-3 in chondrocytes (28). The co-occurrence of high levels of MCP-1, IL-6, and IL-8 in synovial fluid and cytopathic effects in synovial tissue was shown in a patient with chronic arthralgia 18 months after CHIKV infection (22). It is thus likely that the increase in IL-6, IL-8, MCP-1, MMP-1, and MMP-3 levels in the patients with persistent arthralgia could be a consequence of the elevation of IL-1β and TNF-α, and/or a slight increase in IFN-γ, and could play a role in cartilage and bone destruction and the inflammation of joints.
Our study had some limitation, that is, none of the patients included in the present study has been diagnostically tested during the acute illness. Their diagnosis during the initial phase of the infection was primarily based on epidemic data and clinic symptoms during the outbreak. The presence of anti-CHIKV-specific IgG antibodies in these patients has been tested later at 5 years after the acute illness during population screening and clinical data collection between April 2013 and September 2014. Thus, the proportion of patients positive for anti-CHIKV IgG reported might have been underestimated.
Conclusions
This study provides evidence of a persistent immune response mediated by Th1 cells in persistent arthralgia after CHIKV infection and a link between acute CHIKV infection and the development of chronic arthralgia. We propose that the increase in TNF-α, IL-1β, IL-6, IL-8, and MCP-1 levels could play a significant role in the pathogenesis of CHIKV-induced chronic arthralgia through inflammation cascades and the activation of MMP-1 and MMP-3. The increase in TNF-α, IL-12, and MCP-1 levels (and the tendency toward the increase in IFN-γ, IL-1β, IL-6, and IL-8) in patients with severe pain compared with those with nonsevere pain suggests the role played by these cytokines in disease severity. In addition, a trend toward increased TGF-β levels in persistent arthralgia patients, especially in nonsevere patients, might indicate the presence of an anti-inflammatory response in nonsevere pain patients that reduces inflammation. This study provides more clues about the association between inflammation markers and the chronic diseases and the severity of the disease after CHIKV infection. However, further studies with larger sample sizes are needed to prove the correlation between these factors and the development of severe disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was supported by Walailak University (reference number: WU54302) and the Thailand Research Fund (TRF) (reference number: MRG5580070), and this research was partially supported by the new strategic research (P2P) project, Walailak University, Thailand.