
Abstract
Dengue virus (DENV) infection has become an increasingly common concern in tropical and subtropical regions. It has protean manifestations ranging from febrile phase to severe life-threatening illness. In this study, we estimated Th1 and Th2 cytokines and correlated the levels with dengue severity along with certain hematological and biochemical parameters. We also studied the seroprevalence of dengue between October and December 2017 at the Government Theni Medical College, India. Individuals with dengue fever (DF) were positive for either IgM or IgG, or both. The biochemical and hematological parameters along with plasma tumor necrosis factor alpha (TNF-α), interferon-gamma (IFN-γ), granulocyte monocyte-colony stimulating factor (GM-CSF), interleukin (IL)-13, IL-12p70, IL-10, IL-5, IL-4, and IL-2 cytokines were estimated. The prevalence of DF was 42.9% during the study period. IL-2, TNF-α, IL-4, and IL-10 levels were significantly elevated (p < 0.005) in patients with secondary DENV infection, whereas the level of IL-13 remained unaltered during both primary and secondary infections. No statistically significant difference was noticed with IL-12p70, IL-5, IFN-γ, and GM-CSF between the healthy controls and the primary and secondary DENV-infected groups. Increase of 1 unit of TNF-α was associated with a decrease of 160 units of blood platelets. Together, the study suggests that TNF-α could play a key role in the pathogenesis of dengue, and despite the decrease in platelet levels, it remains to be seen whether any other inflammatory cells regulate the levels of TNF-α in DENV infection.
Introduction
Dengue virus (DENV) infection represents a major threat with ∼50 million people chronically infected across the tropical and subtropical world, and estimates suggest that ∼24,000 die annually. Depending on the quality of treatment rendered, mortality rates range from 1% to 20%, particularly in India where 5,000 to 10,000 cases are reported annually (2,16,36,42). Aedes aegypti is a primary vector for transmission as the disease is transmitted through mosquito bite (58). DENV is an enveloped positive-sense single-stranded RNA virus with four serotypes DENV1 to DENV4 (31). Immunity to one specific serotype does not render protection against other serotypes (18). In humans,
Based on clinical symptoms, the WHO has classified dengue with or without warning signs and severe dengue (54). The clinical manifestations vary from self-resolving dengue fever (DF) to most severe form of illness such as dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) (43). DF is characterized with fever, headache, myalgia, bone/joint pain, and rashes, whereas DHF is associated with bleeding and plasma leakage including all the mentioned symptoms of DF. In some cases, it may progress to potentially life-threatening DSS owing to hypovolemic shock (45 –47). During DHF, apoptosis of T cells accounts for viral persistence and disease severity (35). Primary dengue (PD) commonly remains asymptomatic or presents mild symptoms and signs. However, successive infection with other serotypes may result in severe manifestations such as DHF/DSS, also known as secondary dengue (SD) (34,38,44). Cross-reactive memory T cells play an important role in the pathogenesis of SD by altering the cytokine profiles (14,39). Individuals with heterotypic secondary infection are more prone to DHF (19). The presence of non-neutralizing antibodies against heterotypic DENV due to antibody-dependent enhancement is responsible for disease severity in secondary infection (18). Severity of clinical dengue is influenced by factors such as age, serotype and genotype of the infecting virus, immune status of individuals, and genetic makeup of the population (8,27,32,34,51,57).
The clinical signs of DENV infection includes prolonged viremia, leukopenia, neutropenia, and low levels of lymphocytes (17,33,56). The hallmark of the most severe form of DENV infection is thrombocytopenia and clotting abnormalities (13,30,41,50). It blocks the repairing mechanisms of damaged endothelial tissue leading to hemorrhages and third-spacing fluids. Some studies suggest that thrombocytopenia could be due to phagocytosis of DENV-infected mature thrombocytes by autoimmune mechanisms (13,22,52,55). Studies have revealed the role of non-structural protein 1 (NS1) in thrombocytopenia describing that platelet dysfunction arises due to presence of cross-reactive anti-NS1 antibodies (14,53). Severe DENV infection has shown increased levels of antithrombocyte IgM (14) as well as evidence of cytokine storm and plasma leakage resulting from endothelial dysfunction resulting from imbalance in pro- and anti-inflammatory cytokine levels (35,46). An activated cytokine increases the levels of several other cytokines and other cellular mediators (46) facilitating inflammation (11). Studies have revealed the association of cytokine levels with the pathogenesis and severity of infectious diseases. In this study, we measured the plasma levels of several Th1 and Th2 cytokines, namely, tumor necrosis factor alpha (TNF-α), interferon-gamma (IFN-γ), granulocyte monocyte-colony stimulating factor (GM-CSF), interleukin (IL)-13, IL-12p 70, IL-10, IL-5, IL-2, and IL-4 in PD and SD, and correlated with the levels of blood platelets in the patient groups.
Materials and Methods
Ethics statement
The protocols involving human subjects were approved by the Medical Ethics Committee (MEC) of the Government Theni Medical College and Hospital, Theni, India, and were conducted as per the guidelines of the International Conference on Harmonization Guidelines and Declaration of Helsinki. All participants provided written informed consent or assent forms. The written consent form was approved by the ethics committee and signed by the subject or the subject's legally authorized representative. A copy of the document was given to the person signing the form. The study also involved pediatric subjects who provided assent forms. These forms were approved by the ethics committee. The entire consent process was approved by the MEC for conduct of the research.
Patients and specimens
Serum samples were collected from patients with fever from the out-patient clinic of the Theni Government Medical College, Theni, during the months of October to December 2017. Furthermore, nine healthy control samples were also collected for the investigation. The study involved patients aged between 1 and 70 years (both male and female). Patients with the following signs and symptoms were included: vomiting, joint pain, rash, myalgia, retro-orbital pain, and headache, and hemorrhagic manifestation such as petechial rash, melena, bleeding gums, hematuria, and severe abdominal pain. Five milliliters of blood was drawn by venipuncture, and serum was separated to measure the levels of dengue-specific IgG or IgM. Later, the samples were categorized as PD and SD based on the presence of either IgG/IgM or IgG and IgM. The NIV (National Institute of Virology, Pune, India) IgM capture ELISA kit was used to detect dengue-specific IgM (OD >2.1 times P/N ratio, that is, P refers to known positive control and N the known negative control), whereas dengue-specific IgG was detected using a Panbio Dengue IgG capture ELISA kit (IgG >22 units). Secondary DENV infection was determined by measuring IgM/IgG ratio (<1.78) (40). Certain routine laboratory investigations were performed to exclude the other etiological causes of fever of unknown origin. In addition, routine hematological parameters (total white blood cell counts, hematocrit, and platelet counts) and serum biochemical parameters (liver function test) were also performed during the investigation.
Measurement of Th1 and Th2 cytokines
Cytokine measurement was done by using Bio-plexpro™ human cytokine Th1/Th2 panel 9-plex kit (Bio-Rad) as per manufacturer's instructions. The Bio-plex Manager software was used for the optimization of the standard curve and for cytokine measurement. Sample preparation was done by diluting 20 μL of serum sample with 60 μL of Bio-plex human serum diluent. Cytokine standard was diluted in the standard diluent—diluted standard, this solution was kept in ice for 30 min. Followed by this step, fourfold serial dilutions of cytokine standard were done. The 80 μL of standard diluent was taken as blank. The bead preparation was done by diluting the 575 μL of 10 × bead in 5,175 μL of assay buffer and wrapped it with aluminum foil to avoid exposure to light. The 50 μL of bead was added to all 96 wells followed by the addition of 50 μL of blank, standard, and sample accordingly and incubated at 850 rpm for 30 min at 25°C. Meanwhile, detection antibody was prepared by diluting the 300 μL of detection antibody in 2,700 μL of antibody diluent and 25 μL of this solution was added to all wells followed by the incubation at 850 rpm for 30 min. In the intervening period, streptavidin phycoerythrin (SAPE) was prepared by mixing 60 μL of SAPE with 5,940 μL of assay buffer. This solution was vortexed and 50 μL was added to each well followed by incubation at 850 rpm for 10 min. The washing was done in-between every step. The 125 μL of assay buffer was added to all wells and incubated at 850 rpm for 30 sec. Finally, the plate was placed on the Bio-plex microplate platform for cytokine estimation, and values that showed coefficient of variability <10% were included for further analysis as it indicates good level of accuracy.
Statistical analysis
The association between various cytokines, PD, and SD infection as well as healthy control was analyzed using the Kruskal–Wallis test with a post hoc two-tailed Mann–Whitney U test. Pearson correlation was used to study the correlation between the cytokine levels and clinical findings. The association between cytokines, PD/SD infection, and platelet counts was first assessed univariately using linear regression model. All statistical analyses were done using GraphPad Prism 6 software (La Jolla, CA).
Results
Serosurveillance of dengue infection revealed high rates of positivity for infection either for NS1 or for DENV IgM
Between the months of October and December 2017, a total of 2,814 patients with constitutive symptoms and signs of DENV infection were screened for DENV NS1 antigen (Panbio® Dengue Early ELISA, Abbott, CA) or serum IgM MAC ELISA (National Institute of Virology, Pune, India). Not all samples were subjected to both DENV NS1 and IgM, rather choice of use of NS1 or IgM was made based on the timepoint of presentation to the clinic by the patient, that is, if the patients had fever <5 days, NS1 test was carried out, else they were tested for DENV IgM. Of the 2,814 patients tested, 1,208 (42.9%) were positive either for NS1 or IgM antibody or both. Of the 1,208 positive cases, 102 (3.624%) were positive only for NS1, and 1,106 (39.30%) were positive only for DENV-IgM. Table 1 gives the prevalence rate of DENV infection within the study period.
Detection Rate of NS1 and IgM in Dengue Virus-Infected Patients
DENV, dengue virus.
Cytokine profile revealed significant increase in serum TNF-α, IL-2, and IL-10 levels in DENV-infected individuals
Next, we investigated the serum cytokine response to DENV infection among primary and secondary DENV-infected cases using a scatter plot. Our analysis showed that IL-2, TNF-α, IL-4, and IL-10 levels were significantly elevated (p < 0.005) in patients with secondary DENV infection, whereas the level of IL-13 remained constant during both primary and secondary DENV infections. However, there was no statistical significance in the levels of IL-12p70, IL-5, IFN-γ, and GM-CSF between the healthy controls, PD-, and SD-infected groups (Fig. 1). Even though IFN-γ and GM-CSF levels were increased in secondary DENV-infected cases, IL-12 p70 levels were decreased during primary DENV infection together with IL-13 and IL-5 that remained unaltered.
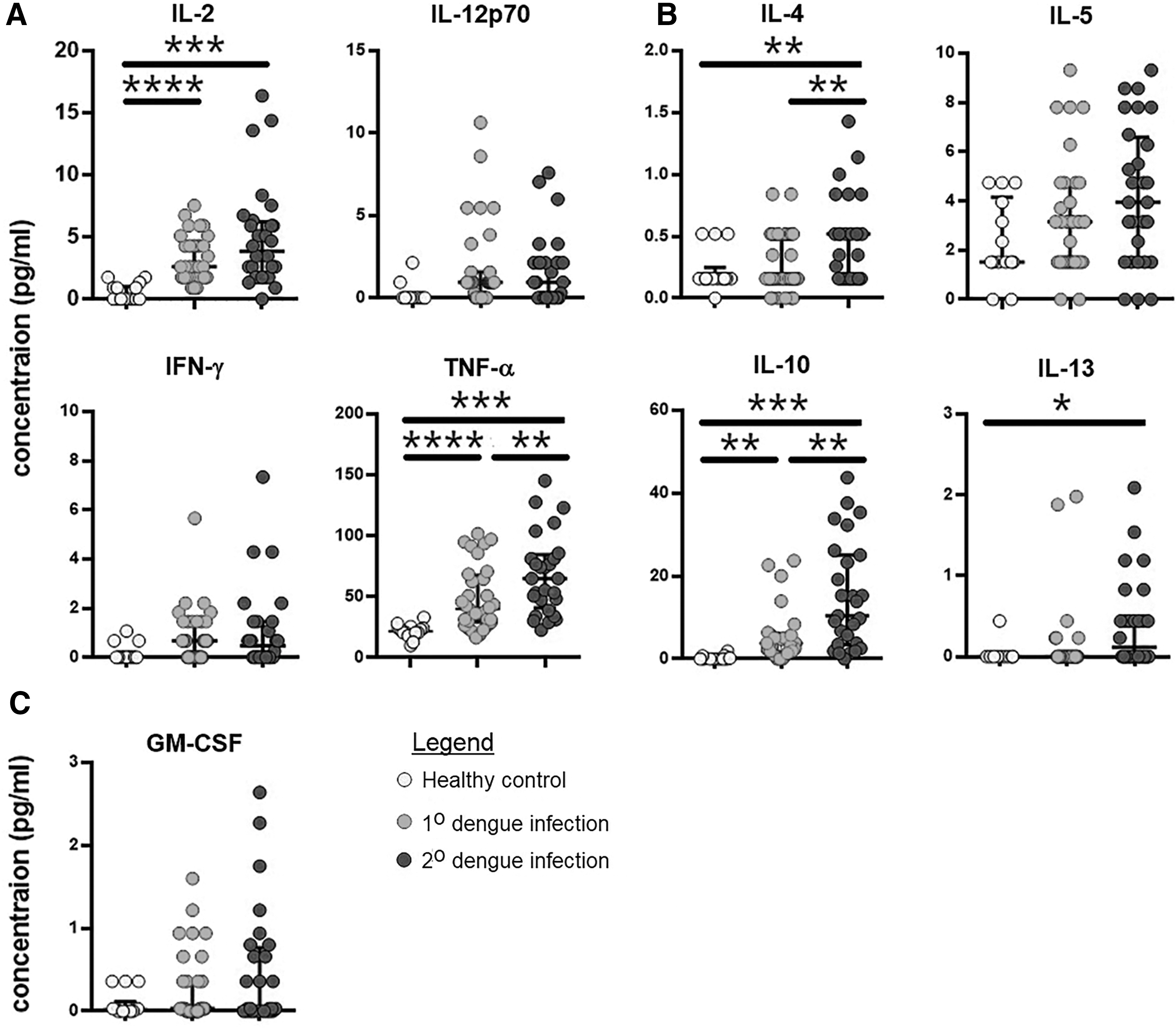
Levels of Th1 and Th2 cytokines as measured between the study groups: healthy control, primary dengue infection, and secondary dengue infection. Scatter plot of levels of each of the Th1/Th2 cytokines (pg/mL) among all the three study groups.
Decrease of blood platelet levels was associated with increase in the serum concentrations of TNF-α among DENV-infected individuals
Next, we further investigated the association of cytokines investigated in our study with dengue-specific thrombocytopenia using a correlation term in the general linear model of analysis. The obtained values revealed that TNF-α showed a negative correlation (R = −0.3437) with blood platelet counts (Table 2). The levels of TNF-α were dependently associated with decrease of platelet count, that is, increase of 1 unit of TNF-α was associated with a decrease of 160 units of platelets. Interestingly, the blood platelet levels were not associated with primary or secondary DENV infections.
Predictors of Platelet Levels (Count) During Dengue Virus Infection in the Study Participants
p < 0.05; ** p < 0.01.
ALP, alkaline phosphatase; GM-CSF, granulocyte monocyte-colony stimulating factor; IFN-γ, interferon-gamma; IL, interleukin; SGOT/ALT, aspartate transaminase; SGPT/AST, alanine transaminase; TLC, total leukocyte count; TNF-α, tumor necrosis factor alpha.
Discussion
Others have compared the levels of IFN-γ and TNF-α among the varying age groups, and have reported that the levels were increased in pediatric DHF (12,15,21,24,25,28) and adult DF patients (6,9,48). Another study compared the cytokine levels among DHF and DF patients to report that the levels of TNF-α, IL-10, IFN-γ, IL-4, IL-13, and GM-CSF were increased in DHF relative to DF (3,11,15,48). The expression of Fcγ receptors in the monocytes and macrophages are upregulated by the IFN-γ and could promote viral replication (29). Interestingly, Chen et al. have noticed that IL-10 was increased in individuals who succumbed to DENV infection, whereas IFN-γ and TNF-α levels remained constant (11). Priyadharshani et al. measured the serum cytokines and reported that TNF-α levels in serum did not reveal any significant difference between DF and DHF patients (49). DENV-infected peripheral blood mononucleocyte culture revealed that IFN-γ, TNF-α, and IL-2 are released during early stages, whereas IL-4, IL-5, and IL-10 cytokines are released during the later phases of infection (1).
In this study, we have assessed the clinical and cytokine profile of dengue cases in Theni, Tamil Nadu, in 2017. Theni district contributes to ∼13% of total dengue cases in Tamil Nadu (20). In our study, 2,814 patients with presumptive symptoms such as fever, headache, and abdominal pain were tested for NS1 and DENV-IgM. Because a strong humoral response is produced on the first day of infection, detectable levels of NS1 are present in the serum of infected cases, followed by high levels of serum IgM. Among the 2,814 individuals tested, only 1,208 were positive for either NS1 or IgM or both (42.9%) during the study period.
DENV infection results in increased production of cytokines by infected monocytes, B lymphocytes, and mast cells. CD4+ and CD8+ T cells are likely targeted by DENV, particularly during secondary infection when serotypes cross-react with bystander CD4+ and CD8+ T cells (4). Assessment of cytokines and their correlation with disease revealed that four cytokines, IL-2, TNF-α, IL-4, and IL-10, were significantly elevated in SD cases as compared with PD and healthy controls. Th1 cells produce IL-2, which plays a protective role against DENV by interacting with its receptor to induce growth, differentiation, and survival of antigen-specific CD4+ and CD8+ T cells (26), whereas IL-4 produced by Th2 cells plays a regulatory role in antibody production, hematopoiesis, and inflammation (10). IL-10 is a pleotropic cytokine that increases the pathogenesis of DENV infection by inhibiting immune mediator secretion, antigen presentation, and phagocytosis (8). T cell-mediated immunological manifestation of secondary DENV infection is influenced by increased cytokine secretion (51). The levels of IL-5 (eosinophil recruitment factor) and IL-12 and IL-4 (anti-inflammatory cytokines) were notably decreased in DF/DHF as compared with healthy controls. TNF-α and IFN-γ are produced by CD4+ T cells against DENV (7). DENV can alter the host immune mechanisms for its survival and also can switch protective Th1 responses to anti-inflammatory Th2 responses (15). Upregulated IL-6 and IL-10 facilitate DENV replication, leading to severe clinical manifestations (23). Others have reported that T cell activation leads to elevated cytokine production, contributing to plasma leakage as a result of vascular endothelial cell dysfunction (37).
Of all the cytokines measured, only TNF-α levels were statistically significant, and correlated negatively with blood platelet counts. TNF-α acts as an important proinflammatory (secreted by monocytes, mast cells, and endothelial cells) and an antiviral cytokine especially during DENV infection. Elevated TNF-α during secondary infection, mainly in DHF patients, reveals the role of TNF-α in increasing the severity of infection (5). TNF-α also contributes to increase of vascular permeability and hemorrhages by inducing the reactive oxygen and nitrogen intermediates (37). Presence of TNF-α indicates a higher risk of more severe forms of dengue infection (34). Together, our study has revealed the association of cytokines along with peripheral blood parameters in primary and secondary DENV pathogenesis. It is also evident that TNF-α could likely play a role in enhancing DENV pathogenesis by contributing to the dengue-associated thrombocytopenia, which, however, remains to be investigated.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Y.K.Y. is supported by a grant from Xiamen University Malaysia Research Funding (XMUMRF), XMUMRF/2018-C2/ILAB/0001. I.J.V. is supported by a Non-NET Fellowship (R170601) from the Central University of Tamil Nadu, India. The remaining authors did not receive funding.