
Abstract
The prevalence of hepatitis B virus (HBV) infection was an imbalance in different provinces of China. This study aimed to investigate the prevalence of HBV infection and evaluate the prophylactic measures in a public hospital of northeast China over the preceding 13 years. A total of 13,948 patients in 2004 and 15,256 patients in 2017 of Shengjing Hospital of China Medical University were tested of serum HBsAg, HBeAg, HBsAb, HBeAb, and HBcAb levels with Abbott MEIA Kits. In people born before 1992, HBsAg-positive rate was 5.45% and 6.47%; isolated HBsAb positive rate was 14.62% and 21.24%; HBV marker negative rate was 54.27% and 42.77% in 2004 and 2017 survey, respectively. The males had a significant higher HBsAg-positive rate than the females. In people born during 1992–2004, HBsAg positive rate was 0.58% and 0.57%, isolated HBsAb positive rate was 41.47% and 46.57%; and HBV marker negative rate was 51.97% and 46.86% in 2004 and 2017 survey, respectively. Males and females had no difference of HBsAg-positive rate. In children born after 2005, HBsAg positive rate was 0.11%, isolated HBsAb positive rate was 76.68%, and HBV marker negative rate was 18.51% in 2017 survey. No difference of HBsAg-positive rate was found between the genders. A dramatic decrease of HBsAg positive rate and a progressive increase of HBsAb-positive rate were found among people born after 1992 and progressed further in those born after 2005. Immunization of infants and timely birth dose was the key method for prevention of HBV infection. Expanded HB vaccination would be needed for people born before 2005, especially those born between 1992 and 2004.
Introduction
Hepatitis B
Perinatal, sexual, and parenteral/percutaneous were the major modes of HBV transmission (20). Transmissions during the perinatal period and early childhood were the main cause for chronic HBV infection (2), it was reported that patients who were infected during neonatal period or early childhood comprised 80–90% of chronic HBV infection, and it was only 5–10% in patients who were infected during adolescence and adulthood (5,8). Therefore, prevention of HBV infection in infants should be the most critical strategy to control chronic HBV infection in China.
The application of HB vaccine was the most effective measure to prevent mother to infant transmission of HBV (16). Following the recommendation of the World Health Organization in 1992, Chinese government included HB vaccination into the national infant immunization programs, but parents had to pay for the vaccine and vaccine administration fees. Therefore, vaccination rates were relatively low in rural and underdeveloped areas. In 2002, hepatitis B vaccine was integrated into Expanded Program on Immunization (EPI), while vaccine administration fees were still paid until 2004. Since 2005, free vaccination against HBV was universal in all neonates (6,3). The vaccination program has resulted in a significantly decreased rate of chronic HBV infection nationally (9,21).
China had a relatively high prevalence of HBV infection. A national survey reported that in 2006, the proportion of HBsAg-positive subjects was 7.18% nationwide, higher than 10% in some high prevalence areas, and 20 million chronic hepatitis B patients were estimated among the HBV infections (6). In 2014, HBsAg-positive rate was 0.32%, 0.94%, and 4.38% among 1–4, 5–14, and 15–29 years old, respectively, according to Chinese Centers for Disease Control (CDC) data (28).
The prevalence of HBV infection was an imbalance in different provinces of China. A Chinese national survey of HBV infection showed that the prevalence of HBV infection in southern China was more serious than that in northern China (6). Understanding the prevalence of HBV infection in the local region was helpful for formulating reasonable prevention and control programs and reducing the prevalence of HBV infection in this area. In 2004, we reported the prevalence profile of HBV infection in a public hospital of Shenyang, China, a moderate prevalence of HBV infection in the adult and significant decrease of HBsAg positive rate in the children were found in that study; however, more that 50% of the children were found nonimmune to HBV (1). To further evaluate the impact of the implementation of hepatitis B vaccine in 1992 and the universal HB vaccination in 2005 on the prevalence of HBV infection in this area and analyze the prophylactic measures, we conducted the reviewing on the prevalence profile of HBV infection in 2017 in the public hospital and compared the data between 2004 and 2017.
Materials and Methods
This retrospective study was carried out in Shengjing Hospital of China Medical University (CMU), which was one of the top 20 largest public hospitals in China and the largest public hospital in northeast China.
A total of 29,204 patients were included in this study. In 2004 survey, we enrolled 13,948 patients hospitalized in Shengjing Hospital of CMU from March 1st to June 30th, 2004, stratifying into two groups based on the date of birth: (1) Born before 1992 (adult group): patients who were born before December 31, 1991; and (2) Born between 1992 and 2004 (young group): patients who were born between January 1, 1992 and December 31, 2004. A total of 9776 patients were enrolled in adult group and 4172 enrolled in young group in 2004 survey.
In 2017 survey, we enrolled 15,256 patients hospitalized from March 1st to May 31st, 2017. They were classified into three groups corresponding to our previous study: (1) Born before 1992 (adult group): patients who were born before December 31, 1991; (2) Born between1992 and 2004 (young group): patients who were born between January 1, 1992 and December 31, 2004; and (3) Born between 2005 and 2017 (children group): patients who were born between January 1, 2005 and December 31, 2017. A total of 9,774 patients were enrolled in adult group, 2,802 in young group, and 2,680 in children group, respectively, in 2017 survey.
To avoid an inflate on the prevalence of HBV infection, patients who had been diagnosed with chronic hepatitis B and were hospitalized repeatedly in these two periods had been excluded.
HBV serum markers were routine examinations for admission in Shengjing Hospital of CMU. Patients' serum samples were collected from venous blood after fasting overnight. HBsAg, HBsAb, HBeAg, HBeAb, and HBcAb levels were tested with chemiluminescence microparticle immunoassay (Architect I8200_C; Abbott, IL). All experiments were performed at the Department of Clinical Laboratory of Shengjing Hospital of CMU. The results of HBV serum markers of the patients were all retrieved from the laboratory information system of Shengjing Hospital. We assumed that it was credible to estimate the prevalence of HBV infection in Shenyang by the information obtained from the hospital information system of Shengjing Hospital.
The rate of HBsAg positive was an indicator for the prevalence of chronic HBV infection. HBsAb was regarded as immune to HBV. Patients who acquired the immunity from HB vaccine usually appeared as positive for isolated HBsAb. The absence of all HBV serum markers was considered as nonimmune to HBV or HBV susceptible. The HBcAb positive patients were deemed as previous exposure to the HBV.
Patients' information used in this study was fully privileged to protect the patient's privacy; there were no additional tests and no harm to the patients for participating in this study. The study procedures were in accordance with the ethical principles and had been approved by the Medical Research and New Technology Ethics Committee of Shengjing Hospital. The Ethics Committee was: The Medical Research and New Technology Ethics Committee of Shengjing Hospital, CMU, and Ethics no. 2015PS118K.
All data were analyzed using the SPSS 24.0 software package (SPSS, Inc., Chicago, IL). Categorical variables were demonstrated with percentage and were compared using the chi-squared test. Multiple groups' comparisons were corrected by Bonferroni correction. p < 0.05 was considered statistically significant.
Results
The prevalence of HBV infection in people born before 1992
In 2004 survey, the prevalence rate of HBsAg positive, HBsAb positive alone, and HBcAb positive and absence of all HBV markers were 5.45% (533/9,776), 14.62% (1,429/9,776), 25.66% (2,509/9,776), and 54.27% (5,305/9,776), respectively, in this group. However, a slight increase of HBsAg positive rate (6.47% [632/9,774]) and HBsAb positive rate (21.24% [2,076/9,774]) was found in 2017 survey, with significant difference comparing with that of 2004 (p < 0.01). In 2017 survey, the rate of all HBV markers negative decreased to 42.77% (4,180/9,774), and HBcAb positive rate was 29.53% (2,886/9,774) of the patients, but with no significant difference when comparing with that of 2004 (p > 0.05) (Table 1 and Fig. 1A).
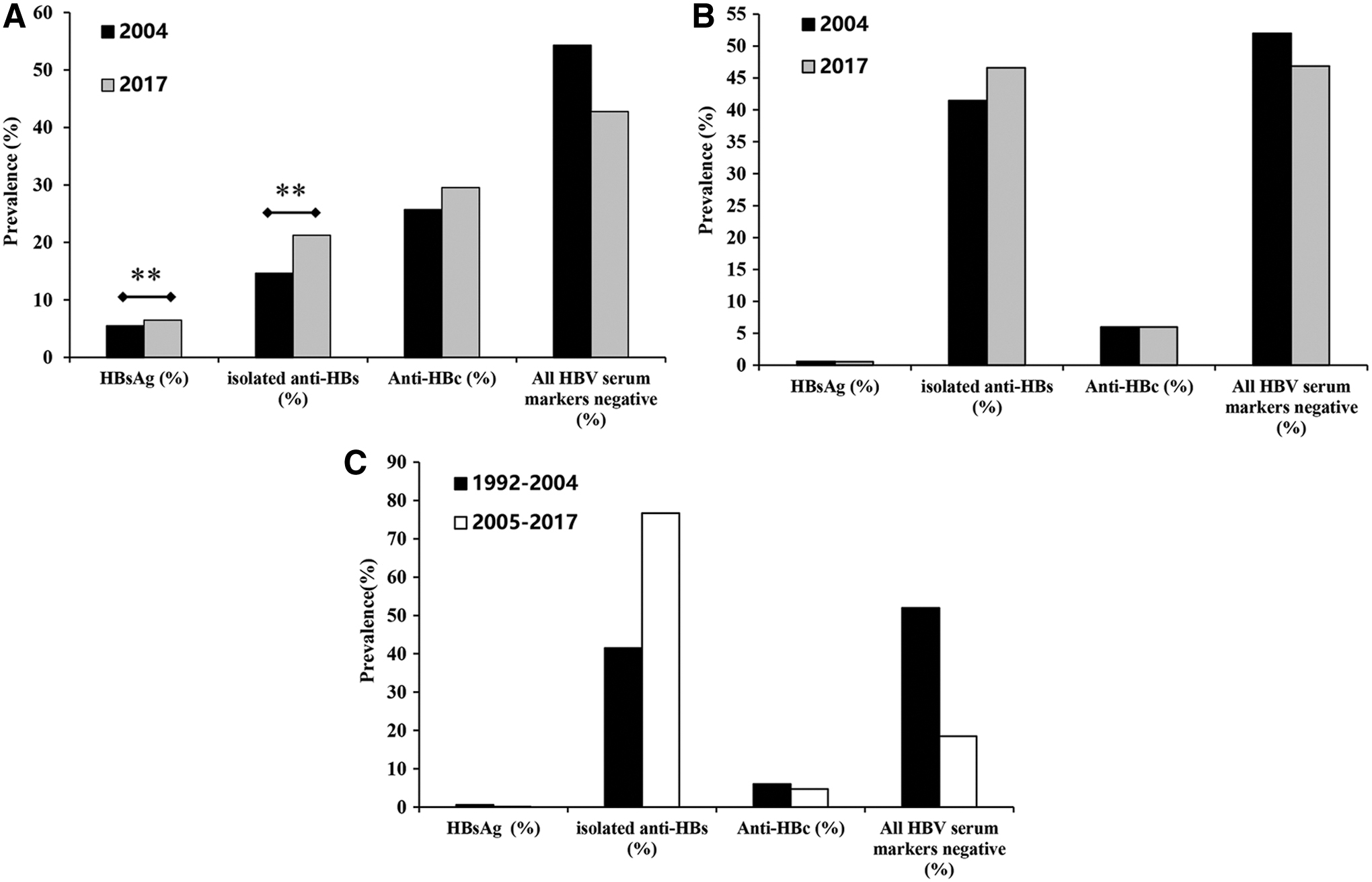
The prevalence of HBsAg positive, isolated anti-HBs positive, anti-HBc positive, and all HBV markers negative in people born before 1992
The Prevalence of HBV Infection in 2004 and 2017, Shengjing Hospital of China Medical University, in Shenyang, China
In 2004 survey, before 1992 versus 1992–2004. In 2017 survey, before 1992 versus 1992–2004, before 1992 versus 2005–2017.
p < 0.01.
Anti-HBc, antibody to the hepatitis core antigen; Anti-HBs, antibody to the hepatitis B surface antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus.
The positive rates of HBsAg in male and female patients were significantly different in people born before 1992. In 2004 and 2017 survey, the positive rates of HBsAg were 8.89% and 9.56% in males and 3.75% and 4.77% in females, respectively. The positive rates of HBsAg in males were significantly higher than that in females in both of these two surveys (p < 0.01) (Table 2).
The Prevalence of HBsAg in Male and Female Patients in 2004 and 2017, Shengjing Hospital of China Medical University, in Shenyang, China
The prevalence of HBV infection in people born between 1992 and 2004
A significant decrease of HBsAg prevalence (0.58% [24/4,172] in 2004 and 0.57% [16/2,802] in 2017) and an increase of HBsAb alone positive rate (41.47% [1,730/4,172] in 2004 and 46.57% [1,305/2,802] in 2017) were found in this group when comparing with the patients born before 1992 in both 2004 and 2017 surveys (p < 0.01). Surprisingly, the ratio of HBV nonimmune patients was still as high as 51.97% (2,168/4,172) and 46.86% (1,313/2,802) in 2004 and 2017 survey, respectively (Table 1 and Fig. 1B).
Although HBsAg positive rate was significantly different in males and females born before 1992, in patients born between 1992 and 2004, the HBsAg positive rates were 0.73% and 0.78% in males and 0.43% and 0.47% in females, respectively, in 2004 and 2017 surveys. No significant difference of HBsAg positive rates was found between different genders (p > 0.05) (Table 2).
The prevalence of HBV infection in people born after 2005
The prevalence of HBV infection in people born after 2005 was evaluated in 2017 survey. The rate of HBsAg positive, HBcAb positive, and HBV nonimmune patients dramatically declined to 0.11% (3/2,680), 4.70% (126/2,680), and 18.51% (496/2,680), respectively. HBsAb alone positive rate increased to 76.68% (2,055/2,680), all with significant differences from those of the patients born before 1992 and born between 1992 and 2004 (p < 0.01) (Table 1 and Fig. 1C).
In the population born after 2005, the positive rates of HBsAg in male and female patients were 0.13% and 0.09%, respectively. No significant difference was found between the two groups (p > 0.05) (Table 2).
Discussion
The prevalence levels of HBV infection are estimated based on the prevalence of HBsAg, which varies widely in the world, and countries can be divided into high endemic areas (HBsAg positive rate ≥8%), regions of intermediate prevalence (HBsAg positive rate 2–7%), and low endemic areas (HBsAg positive rate <2%) of HBV infection (17). According to our results, people born before 1992 (before the implementation of hepatitis B vaccine to infant) in Shenyang city had a moderate prevalence of HBsAg. The first national hepatitis B seroepidemiological survey was released in China in 1992, which showed that the prevalence of HBsAg was about 10% for people aged 1–59 years, including young children (22). In this study, the average HBsAg-positive rate of all population was 3.99% and 4.27% in 2004 and 2017 survey, which was lower than the national prevalence (6,28), but similar to that reported in Jilin province (19,24,25), which is near to Shenyang, and much lower compared with 7.9% in Zhejiang province in southeast China (12).
The HBsAg and HBcAb positive rates were notably higher, while the isolated HBsAb positive rate was significantly lower in people born before 1992 than that in people born after 1992 in both 2004 and 2017 surveys. The percentage of all hepatitis B markers negative was still high in patients born before 1992 and born between 1992 and 2004 in both surveys, but it significantly decreased in those born after 2005. These results suggested that in people born before 1992, when hepatitis B vaccine was not widely accessed in China, HBV infection remained consistently high. People might have mainly acquired the immunity to HBV by covert infection. Surprisingly, we found a slight increase of HBsAg positive rate in people born before 1992 when comparing between 2004 and 2017 survey. These results indicated that although HBV infection was mainly acquired at birth, adults were also at risk of infection. Moreover, we found an increase of HBsAb positive rate in patients born before 1992 and born between 1992 and 2004 in 2017 survey when comparing with those of 2004 survey. We speculated that the reason for this result may be that during the past 13 years, more people realized the importance of HB vaccination, and some of them completed the full course of three doses of HB vaccination. The above findings indicated that the expanding and booster of the HB vaccine among individuals of HBV nonimmune adults might be necessary.
China integrated hepatitis B vaccine into EPI in 2002 and required obstetrical nurses who deliver babies to administer the birth dose of hepatitis B vaccine within 24 h after birth (6,26). HB vaccination of infants contributed directly to the reduction of HBsAg prevalence among populations born during 1992–2004. The national serosurvey in 2006 indicated that HBsAg prevalence for people aged 1–59 years decreased from 9.8% to 7.2% and for children under 5 years was only 1.0% (6). Liang's study discovered that the prevalence of HBsAg was reduced to 2.1% among all children born during 1992–2005 and 1.0% among children born after 1999 (7). Consistent with the literatures, we found that HBsAg-positive rate dramatically decreased 10-folds in people born during 1992–2004 comparing with those born before 1992 in both 2004 and 2017 surveys. Liang's survey reported that in the Eastern provinces, including Liaoning (Shenyang is the capital city of Liaoning), the rates of three-dose and timely birth dose coverage of HB vaccine were 64.2% and 45.2% among children born during 1992–2001. This increased to 96.8% and 85.5% for children born during 2002–2005 (7). Nevertheless, the prevalence of isolated HBsAb in our study was inconsistent with the reports. Individuals with isolated HBsAb were less than 50% among those born between 1992 and 2004 in both 2004 and 2017 surveys. Meanwhile, the prevalence of HBV nonimmune people was about 50% in both surveys. We assumed a possible reason for the discrepancy: HB vaccination rate was still low in general population between 1992 and 2004, especially in the rural and underdeveloped areas. But mothers with chronic HBV infection would pay more attention to HB vaccine. Therefore, the newborns of HBsAg positive mothers might have a higher rate of HB vaccination resulting in a significant decline of HBsAg prevalence.
After hepatitis B vaccine had been fully and freely integrated into infant routine immunization in 2005, a remarkable decrease of HBsAg prevalence was found for children born after 2005 and the rate of HBV nonimmune people was also dramatically decreased. These results indicated that universal HB vaccination was the most important means to improve the immunity against HBV infection and reduce HBsAg prevalence among the population.
The group born in 1992–2004 in 2004 survey and the group born after 2005 in 2017 survey represented people of 0–12 years in 2004 and 2017, respectively. Therefore, we compared the results of these two groups (Fig. 1C). Our results revealed that HBsAg prevalence decreased by 81% comparing to 2004 (from 0.58% to 0.11%) and the prevalence of isolated HBsAb increased from 41.47% to 76.68% among children aged 0–12 years from 2004 to 2017. These results were in accordance with a previous report of hepatitis B serosurveys with an 8-year interval in Shandong Province, with the prevalence of HBsAg decreased from 1.36% in the 2006 survey to 0.21% in the 2014 survey among children aged 1–14 years (10), and Guangdong Province (27) (which was located in the southeast of China) revealed that the HBsAg prevalence was 1.16% among people aged 1–14 years. All of the results showed that with higher overall immunization coverage and timely administration of birth doses, there was dramatic reduction in the prevalence of HBsAg among children born after 2005. However, 18.51% of them were still nonimmune to HBV and 4.7% were positive of HBcAb. The HBcAb positive rate was relatively higher than that in Henan province (2.6%) (23) and Guangdong Province (2.35%) (27). We analyzed the reasons from two aspects. One was HB vaccination coverage and the effectiveness of HB vaccine. It was reported that the rates of three dose and timely birth dose coverage of HB vaccine were 93.4% and 82.6% for children born in 2005 (7). The gap of the coverage rate might account for this situation, and there were a few people with no immune response to HB vaccine. The other was the failure to block HBV mother-to-infant transmission. Our group previously reported that HBsAg prevalence among pregnant women was 3.1% (441/14,314), 34.2% were HBeAg positive, and 25.4% had high viral load of HBsAg positive pregnant woman (≥2 × 106 IU/mL) (15). Infants born to mothers with HBeAg and high HBV DNA viral load had a higher incidence of nonresponse to HB vaccine (4). Therefore, to further reduce HBV infection in neonates, hepatitis B vaccine and hepatitis B immunoglobulin in neonates are necessary, as well as antiviral treatment during middle and late gestation (14). What's more, carrying out a close follow-up for infants born to mothers with HBeAg and high HBV DNA titers is also indispensable.
The advantage of this study was that we investigated the prevalence of HBV infection in hospitalized patients of Shengjing Hospital in both 2004 and 2017 and compared the changes of the prevalence of HBV infection in the population after 13 years dynamically, which could better evaluate the immunity level of the local population to HBV. However, there were some limitations in the study. First, although Shengjing Hospital was the largest comprehensive hospital in this region, the prevalence of HBV infection could roughly reflect the population's HBV infection status, but the results might be different from those of the local residents because of the investigation based on the inpatient population. Second, we did not conduct a one-to-one survey of the population's HB vaccine coverage, but grouped them according to the national HB vaccination strategy, which might lead to bias in the results.
Conclusion
In conclusion, a dramatic decrease of HBsAg positive rate and a progressive increase of HBsAb-positive rate among children born after 1992 were realized after HB vaccine was being included in routine immunization of infants. The higher the coverage of HB vaccine to infants the lower the rate of positive HBsAg and higher the rate of positive HBsAb. Immunization of infants and timely birth dose would be the key point for prevention of HBV infection. However, HBV vaccination rate was still low in those born before 2005; expanded HB vaccination would still be needed for them, especially in people born between 1992 and 2004.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
“Thirteenth Five-Year Plan” Major National Science and Technology Major Projects (2017ZX10202203); Liaoning Provincial Science and Technology Planning Project (2013225021).