
Abstract
The difference of splenic pathologic alterations and immune function changes in portal hypertension (PHT) with different etiology is unclear. We aimed to investigate the differences between the hypersplenic patients with hepatitis B virus (HBV)-related PHT and Budd-Chiari syndrome (B-CS). A total of 93 patients with hypersplenism due to Chinese primary B-CS (B-CS group), 105 patients with hypersplenism due to HBV-related cirrhosis (HBV/PHT group), and 31 healthy people (control group) were included in this study retrospectively. The peripheral bloods and paraffin sections of the spleen from part of patients were analyzed by flow cytometry and immunohistochemistry. Hypersplenism and PHT were more serious in HBV/PHT group than in B-CS group. In the peripheral blood, the percentages of regulatory T cell (15.1% vs. 8.1% vs. 2.2%, p = 0.0021) and myeloid-derived suppressive cells (2.8% vs. 0.8% vs. 0.9%, p = 0.009) were higher, but CD4+ T and CD8+ T cells were lower in HBV/PHT group compared with B-CS and control groups. In spleen, the percentages of CD4+ T and CD8+ T cells were lower, but CD68+ macrophages were higher in HBV/PHT group than in B-CS group. Moreover, CD86, inducible nitric oxide synthase, Toll-like receptor 4, and tumor necrosis factor-α expression in the spleen, as well as the plasma lipopolysaccharide (LPS) level (677.7 vs. 311.1 vs. 222.1 ng/mL, p = 0.0022), were significantly higher in HBV/PHT group than in B-CS and control groups. The HBV/PHT group showed more severe immunosuppression and immune dysfunction and more substantial hypersplenism and splenic phagocytosis than B-CS group.
Introduction
Portal hypertension (PHT) is a common disease that causes splenomegaly and hypersplenism, as well as upper gastrointestinal bleeding and other life-threatening complications (13,32). In China, the most common cause of PHT is hepatitis B virus (HBV) infection; thus, current studies of hypersplenism and PHT are mostly focused on HBV/PHT (12). Studies have shown that splenic immune function is disordered in HBV/PHT, and may participate in hypersplenism and hepatic fibrosis (16,39). Although hypersplenism was thought to be caused solely by increased pooling of platelets in the enlarged spleens due to PHT (22), recent studies have reported a more complicated mechanism of thrombocytopenia, including decreased platelet production, splenic sequestration, and increased platelet destruction (24).
For most patients, the large spleen is the main contributing factor for hypersplenism in PHT patients (22). Nevertheless, alterations in splenic immune function and histopathology remain undefined. Primary Budd-Chiari syndrome (B-CS) is a posthepatic PHT which is different in China from that in Western countries, including clinical presentations, etiology and pathology and mostly patients without hypercoagulable state and infection (26,29,30,33,42). The spleen shows only high portal pressure, which is quite different from the situation of HBV/PHT with both HBV infection and high portal pressure.
The percentage of B-CS patients with splenomegaly varies from 30% to 50% (25,38), while in HBV/PHT patients it is >60% (40,43). Few studies have paid attention to the spleen of B-CS. The pathologic changes and immune functions of spleens with hypersplenism may be significantly different between the two types of PHT. As reported, treatments for enlarged spleen including splenectomy, partial splenic embolization, and splenic artery ligation are common in HBV/PHT patients but rarely in B-CS patients in China (2,36,41). In this study, our aim is to investigate the differences in pathologic alterations and immune functions of the spleen between HBV/PHT and B-CS patients, and help us better understand the role of HBV infection in the mechanism of hypersplenism and immune functions of spleens, as well as therapy potential for PHT.
Materials and Methods
Patients
A total of 359 patients with hypersplenism, including 158 patients with Chinese primary B-CS and 201 patients with HBV-related cirrhosis, were screened for enrollment in this study from June 2012 to September 2017 at the First Affiliated Hospital of Zhengzhou University and the Second Affiliated Hospital of Xi'an Jiaotong University. We included 93 patients with hypersplenism due to Chinese primary B-CS and 105 patients with hypersplenism due to HBV/PHT based on the inclusion/exclusion criteria (Fig. 1). All of the enrolled HBV/PHT patients were treated with entecavir, lamivudine, or adefovir, but not interferon agents, and the HBV DNA were <2,000 IU/mL before surgery. A total of 31 healthy people were enrolled as control group. All HBV/PHT patients enrolled (100%), and only 14 of the B-CS patients (15%) underwent splenectomy.
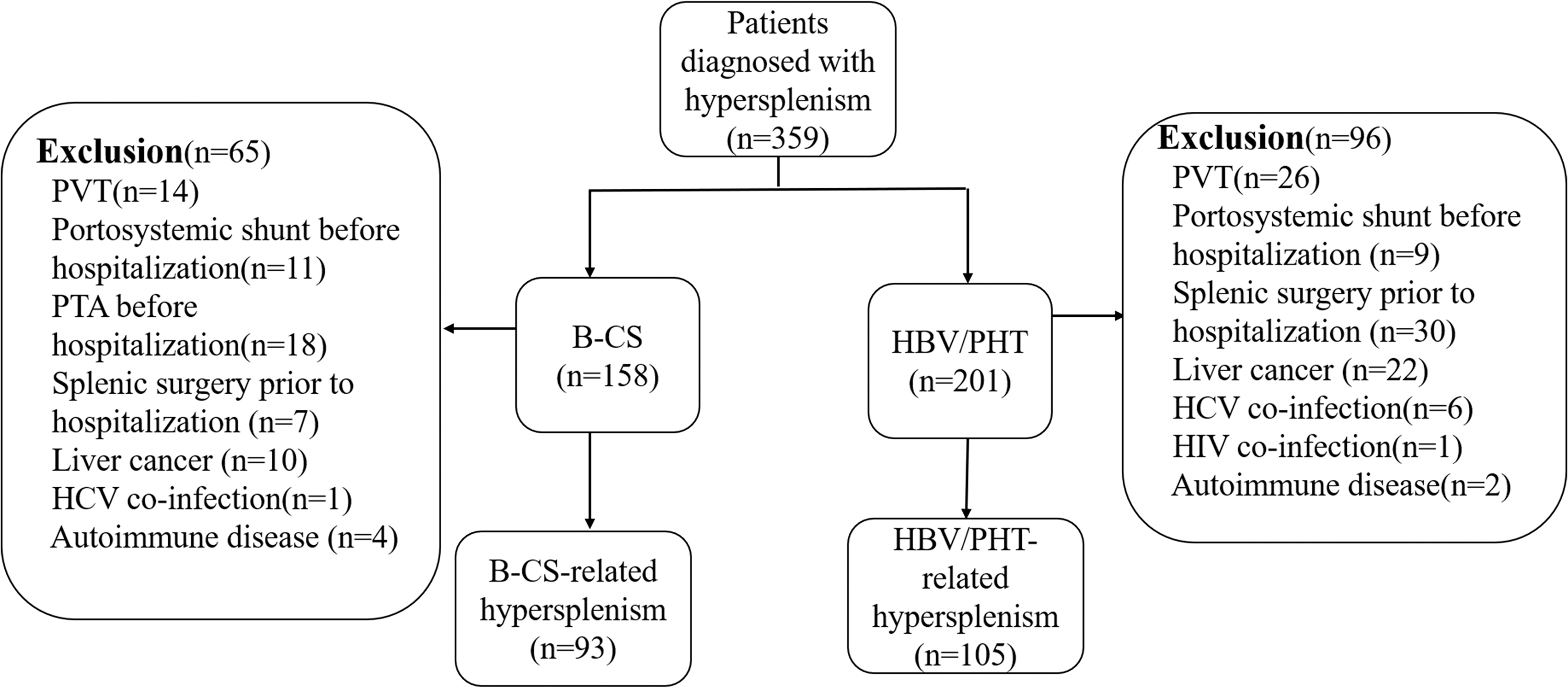
Flow diagram representing the study cohort. B-CS, Budd-Chiari syndrome; HBV/PHT, hepatitis B virus-related portal hypertension; HCV, hepatitis C virus; HIV, human immunodeficiency virus; PTA, percutaneous transluminal angioplasty; PVT, portal vein thrombosis.
Clinical data before treatment, including the whole blood count, liver function, and imaging results, were collected and analyzed. Routine laboratory methods were used to determine the serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin (ALB), globulin, and prealbumin (PA) levels and the white blood cell (WBC) and platelet counts. Spleen size was calculated by the formula (spleen size = 30 + 0.58 × [length × width × thickness]) as previously described (28). We used the platelet/spleen volume ratio (PSVR) to represent the severity of PHT as described in previous studies (3,31). The portal vein and spleen vein diameters were analyzed by color Doppler ultrasound. The clinical characteristics of the patients and healthy controls are summarized in Table 1. This study was approved by the Institutional Ethics Committee of the First Hospital of Zhengzhou University and the Second Affiliated Hospital of Xi'an Jiaotong University, and we had acquired the agreement and approval of patients' samples application.
The Clinical Characteristics of the Patients and Healthy Controls
Values are the mean ± standard deviation unless otherwise stated.
p < 0.05 compared with the B-CS group.
p < 0.01 compared with the B-CS group.
p < 0.01 compared with the control group.
ALB, albumin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; B-CS, Budd-Chiari syndrome; Dpv, portal vein diameter; Dspv, spleen vein diameter; Glb, globulin; HBV/PHT, hepatitis B virus-related portal hypertension; INR, international normalized ratio; PA, prealbumin; PSVR, platelet/spleen volume ratio; PT, prothrombin time; TB, total bilirubin; UGB, upper gastrointestinal bleeding; WBC, white blood cell.
Inclusion criteria
B-CS patients: membrane or occlusion of the inferior vena cava and/or hepatic veins and splenomegaly shown by ultrasound, CTA, or MRI; clinically manifested ascites; and abdominal wall varices and/or venous varicosities of the lower limbs.
HBV/PHT patients: history of chronic HBV infection and HBV infection confirmed in the serum; splenomegaly shown by ultrasound, CTA, or MRI.
Exclusion criteria
Thrombosis in the portal vein system shown by ultrasound, CTA, or MRI.
Portosystemic shunt or splenic surgery conducted before hospitalization.
Liver cancer.
HCV or HIV coinfection.
Autoimmune disorders.
Flow cytometry and ELISA
Two-milliliter peripheral blood samples were collected from 14 B-CS patients, 11 HBV/PHT patients, and 7 healthy controls within 24 h into EDTA-containing anticoagulant-coated tubes (Supplementary Fig. S1). One hundred microliters of plasma were collected after centrifugation (1,500 rpm, 5 min), and the plasma lipopolysaccharide (LPS) levels were measured by ELISA (Westang, Shanghai, China). Whole blood from each patient was divided into three tubes after removing red blood cells using tris-NH4Cl.
The samples were stained with CD3-APC, CD4-PerCP, and CD8-AmCyan antibodies in tube 1; CD4-PerCP, CD25-Blue, and FOXP3-FITC antibodies in tube 2; and LIN-FITC, HLA-DR-AmCyan, and CD33-APC antibodies in tube 3 (all antibodies were from BioLegend Company). Then, the samples were subjected to flow cytometry analysis using a four-color FACS Calibur flow cytometer (BD Biosciences) as follows: CD3-APC/CD4-PerCP/CD8-AmCyan in tube 1 for T cells; CD4-PerCP/FOXP3-FITC/CD25-Blue in tube 2 for regulatory T cell (Tregs); and LIN-FITC/HLA-DR-AmCyan/CD33-APC in tube 3 for myeloid-derived suppressive cells (MDSCs). The data were analyzed using the FlowJo software. CD3+CD4+ T cells, CD3+CD8+ T cells, CD4+CD25+FOXP3+ Tregs, and CD33+LIN−HLA-DR− MDSCs were expressed as cell percentages in the peripheral blood. The clinical characteristics of the patients and healthy controls are summarized in Supplementary Table S1.
Histological and immunohistochemical analyses
Sections of paraffin-embedded spleen tissues from 14 B-CS patients, 12 HBV/PHT patients, and 7 traumatic spleen patients fixed in 10% buffered formalin solution were stained with hematoxylin and eosin (H&E) and Masson's trichrome (Masson Kit, SBJ Bio, Nanjing, China), and assessed through immunohistochemistry (Supplementary Fig. S1) to detect CD4 (ProteinTech; diluted 1:200), CD8 (ProteinTech; 1:200), CD68 (ProteinTech; 1:100), CD86 (ProteinTech; 1:200), inducible nitric oxide synthase (iNOS) (ProteinTech; diluted 1:200), Toll-like receptor 4 (TLR4) (ProteinTech; diluted 1:200), Toll-like receptor 3 (TLR3) (ProteinTech; diluted 1:200), and tumor necrosis factor-α (TNF-α) (abcam, United Kingdom; 1:100).
After dewaxing, antigen retrieval was performed at 95°C for 20 min with citric acid hydrochloric acid antigen retrieval buffer. The slides were incubated in 3% H2O2 for 20 min to block endogenous peroxidase for immunohistochemistry (IHC). The tissue sections were incubated with blocking buffer containing 5% goat serum for 30 min, followed by a primary antibody (rabbit antihuman) at 4°C overnight and a secondary antibody (goat antirabbit) for 30 min. SABC (CWBIO, Beijing, China) was utilized to amplify the signal before hematoxylin and DAB (CWBIO) staining. The sections were visualized by light microscopy, and images were acquired on a NIKON camera (DS-Fi1, Japan). The digitalized images were analyzed using Image-Pro Plus 6.0. The clinical characteristics of the HBV/PHT and B-CS patients and spleen rupture patients are summarized in Supplementary Table S2.
Quantitative reverse transcription PCR
Total RNA was extracted with RNAprep Pure FFPE Kit (TIANGEN BIOTECH, Beijing, China) and then reverse transcribed to complementary DNA using a PrimescriptTM RT reagent kit (Takara). Quantitative reverse transcription PCR was then performed using SYBR Premix Ex Taq II and an ABI7500 fast instrument (ABI Life technologies). The relative abundance of the target genes was determined by the comparative cycle threshold Ct method (2−ΔΔCt) and normalized to glyceraldehyde phosphate dehydrogenase (GAPDH) levels. The primers are shown in Supplementary Table S3.
Statistical analysis
SPSS 24.0 was used for the statistical analysis. One-way ANOVA and the least significant difference (LSD) test were used for mean value comparisons among the three groups, and Pearson's test was used for the correlation analysis. Statistical significance was established at p < 0.05.
Results
HBV/PHT patients have more severe hypersplenism and liver dysfunction than B-CS patients
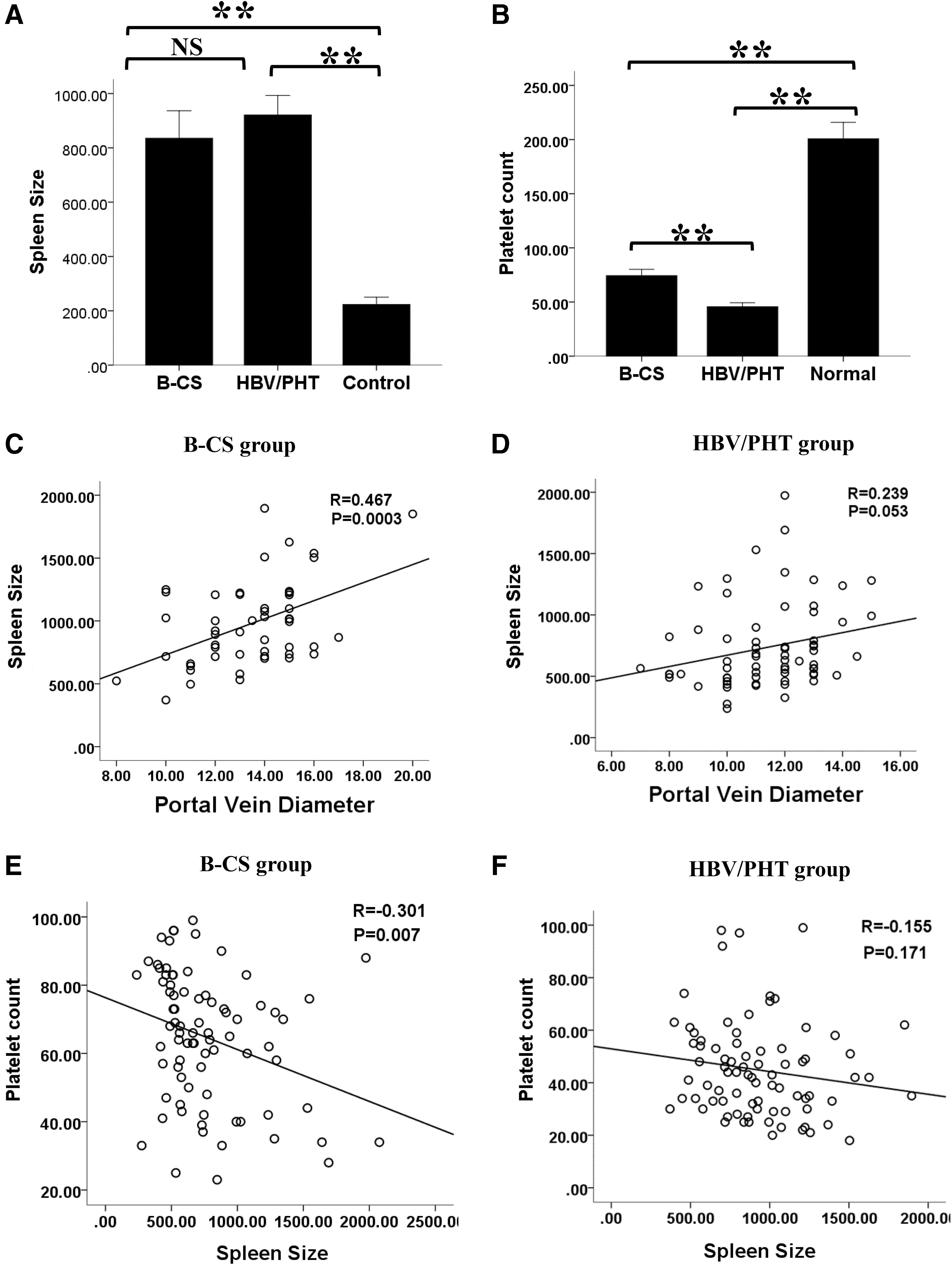
No differences in age and gender were found among the three groups (Table 1). Compared with those of B-CS group, HBV/PHT group had lower WBC and platelet counts but similar spleen sizes (835.3 ± 392.2 cm3 vs. 920.9 ± 327.7 cm3, p = 0.158). Furthermore, the platelet count was negatively correlated with the spleen size (R = −0.301, p = 0.007) in B-CS group but not in HBV/PHT group (R = −0.155, p = 0.171) (Fig. 2). The spleen size correlated better with the portal vein diameter in B-CS group (R = 0.467, p = 0.0003) than in HBV/PHT group (R = 0.239, p = 0.053).
Comparison of clinical data among the three different groups.
Furthermore, the clinical data in HBV/PHT group, such as the portal vein diameter (13.6 ± 2.1 vs. 11.4 ± 1.8 mm, p < 0.0001) and spleen vein diameter (11.4 ± 2.5 vs. 10.1 ± 3.1 mm, p = 0.0003), were greater than those in B-CS group, but the PSVR (0.05 ± 0.03 vs. 0.11 ± 0.06, p < 0.0001) was smaller than that of B-CS group. Compared with HBV/PHT group, the patients in B-CS group had lower serum ALT, AST, prothrombin time, and globulin levels but higher serum ALB and PA levels. However, no differences in total bilirubin and alkaline phosphatase were found between the two groups (Table 1).
HBV/PHT patients show more severe immunosuppression and immune dysfunction than B-CS patients
In HBV/PHT group, the percentages of Tregs (15.1% ± 6.2%) and MDSCs (2.8% ± 1.4%) were higher than those in B-CS (vs. 8.1% ± 4.3%, p = 0.007; vs. 0.8% ± 0.2%, p = 0.003) and control groups (vs. 2.2% ± 0.9%, p = 0.0007; vs. 0.9% ± 0.2%, p = 0.013). Conversely, the percentages of CD3+CD4+ T (24.8% ± 10.4%) and CD3+CD8+ T cells (6.8% ± 3.5%) were lower in HBV/PHT group than in B-CS (vs. 43.6% ± 14.6%, p = 0.008; vs. 18.5% ± 7.1%, p = 0.006) and control groups (vs. 41.8% ± 10.3%, p = 0.001; vs. 23.1% ± 3.4%, p < 0.0001). Compared to control group, the B-CS group had a higher percentage of Tregs (8.1% − 4.3% vs. 2.2% − 0.9%, p = 0.011) but similar percentages of MDSCs, CD3+CD4+ T cells and CD3+CD8+ T cells (Fig. 3).
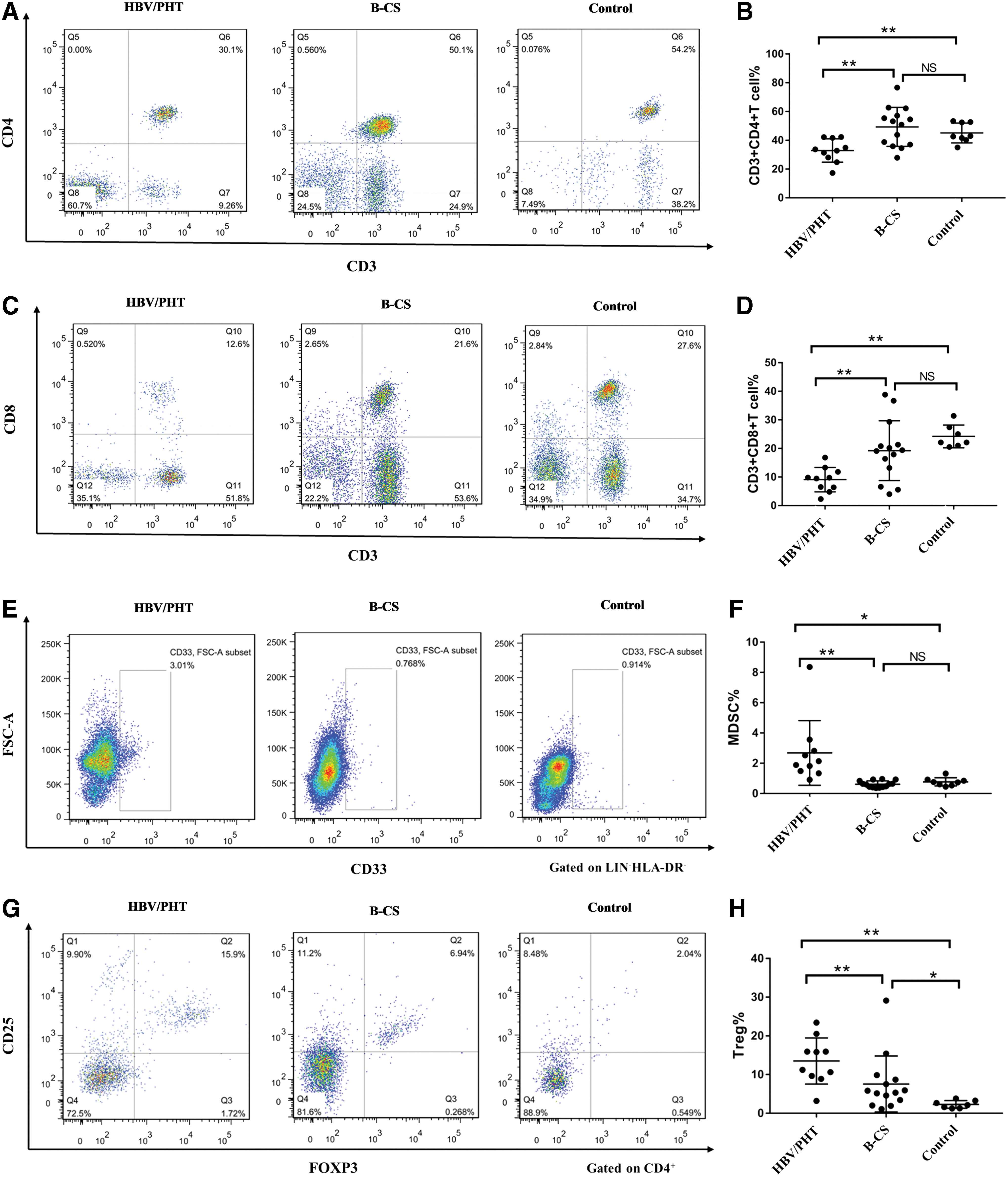
Flow cytometry analysis results for the peripheral blood and comparisons among the B-CS, HBV/PHT, and control groups.
The splenic pathology and immune state between HBV/PHT group and B-CS group
The red pulp area was enlarged, and the white pulp area was reduced in both B-CS and HBV/PHT groups. Substantial hyperplasia of the splenic nodules was found in HBV/PHT group but not in B-CS and control groups. The germinal center percentage in the splenic nodules was greater in HBV/PHT group (27.9% ± 11.2% vs. 17.1% ± 7.4% vs. 7.3% ± 3.5%, p = 0.00001) than in B-CS and control groups. Moreover, substantial splenic fibrosis was found in both B-CS and HBV/PHT groups, although the fibrotic area was larger in the former (0.5% ± 0.2% vs. 0.3% ± 0.2%, p = 0.029) (Fig. 4). The IHC results showed that the splenic CD4+ cell (7.3% ± 2.4%) and CD8+ cell percentages (6.2% ± 2.1%) were dramatically lower in HBV/PHT group than in B-CS (vs. 15.0% ± 5.2%, p = 0.0083; vs. 20.1% ± 6.1%, p = 0.0021) and control groups (vs. 15.1% ± 3.6%, p = 0.0071; vs. 19.7% ± 6.4%, p = 0.0004), whereas the percentages of CD4+ and CD8+ T cells in B-CS group are similar to control group (Fig. 5). Moreover, the splenic CD68+ macrophages percentage was dramatically lower in HBV/PHT group (4.5% ± 0.8%) than in B-CS group (vs. 7.7% ± 0.9%, p = 0.0122) and control group (vs. 15.3% ± 1.5%, p < 0.001). And the B-CS group also had lower percentage of CD68+ macrophages than control group (7.7% ± 0.9% vs. 15.3% ± 1.5%, p = 0.0003) (Fig. 6).
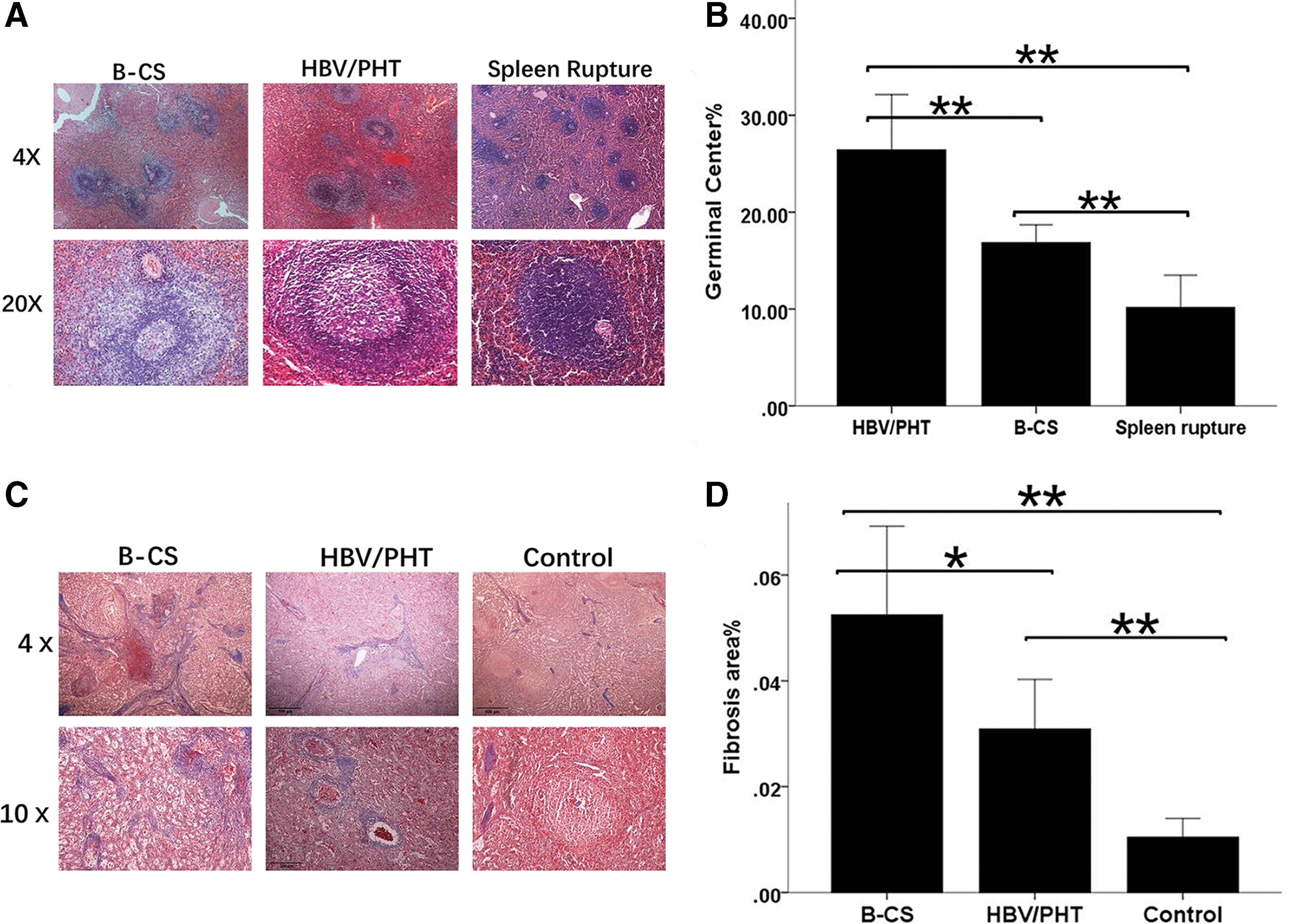
The splenic pathology in the three different groups.
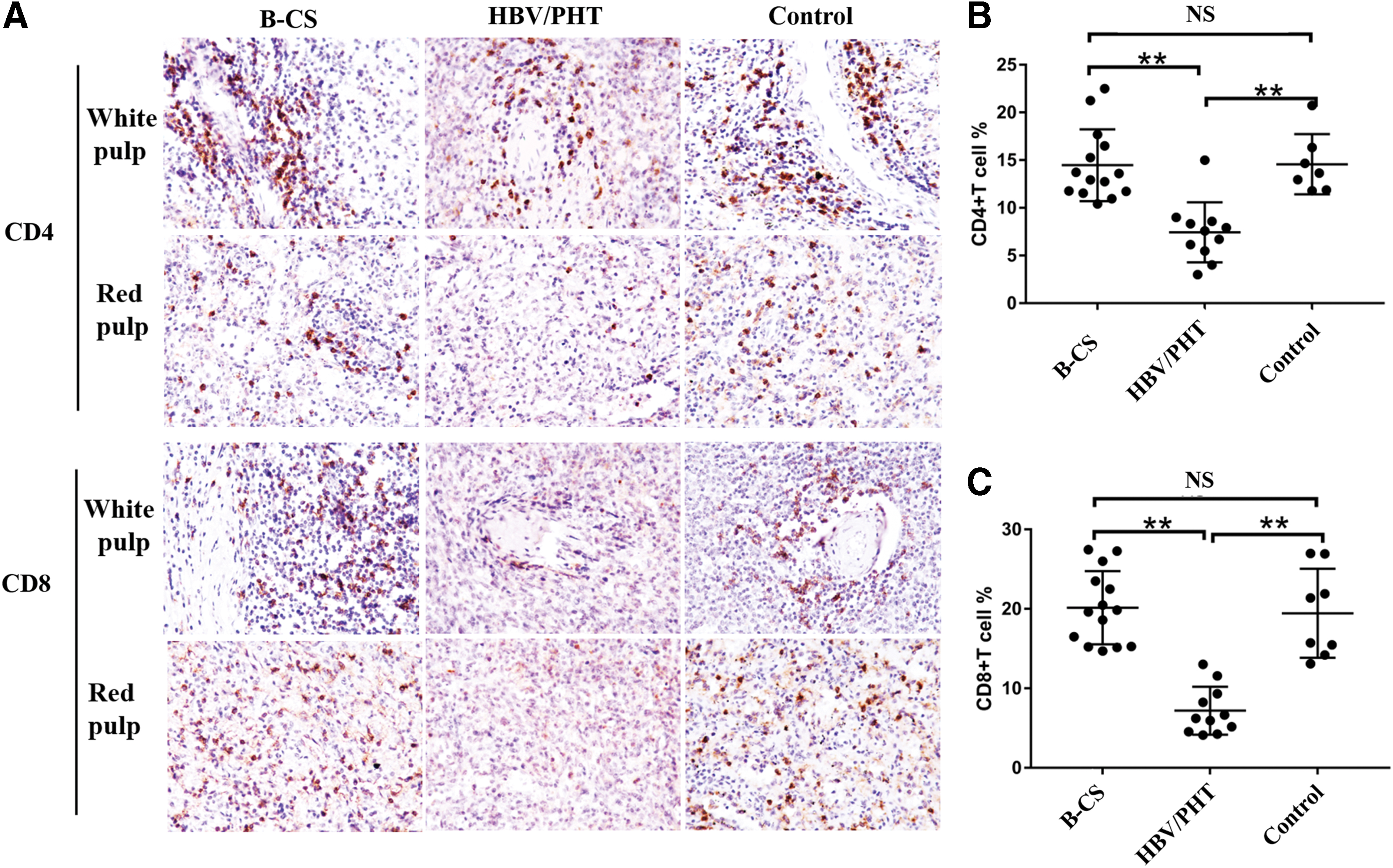
Immunohistochemical staining results of CD4 and CD8 of paraffin-embedded splenic tissue sections from the three different groups.
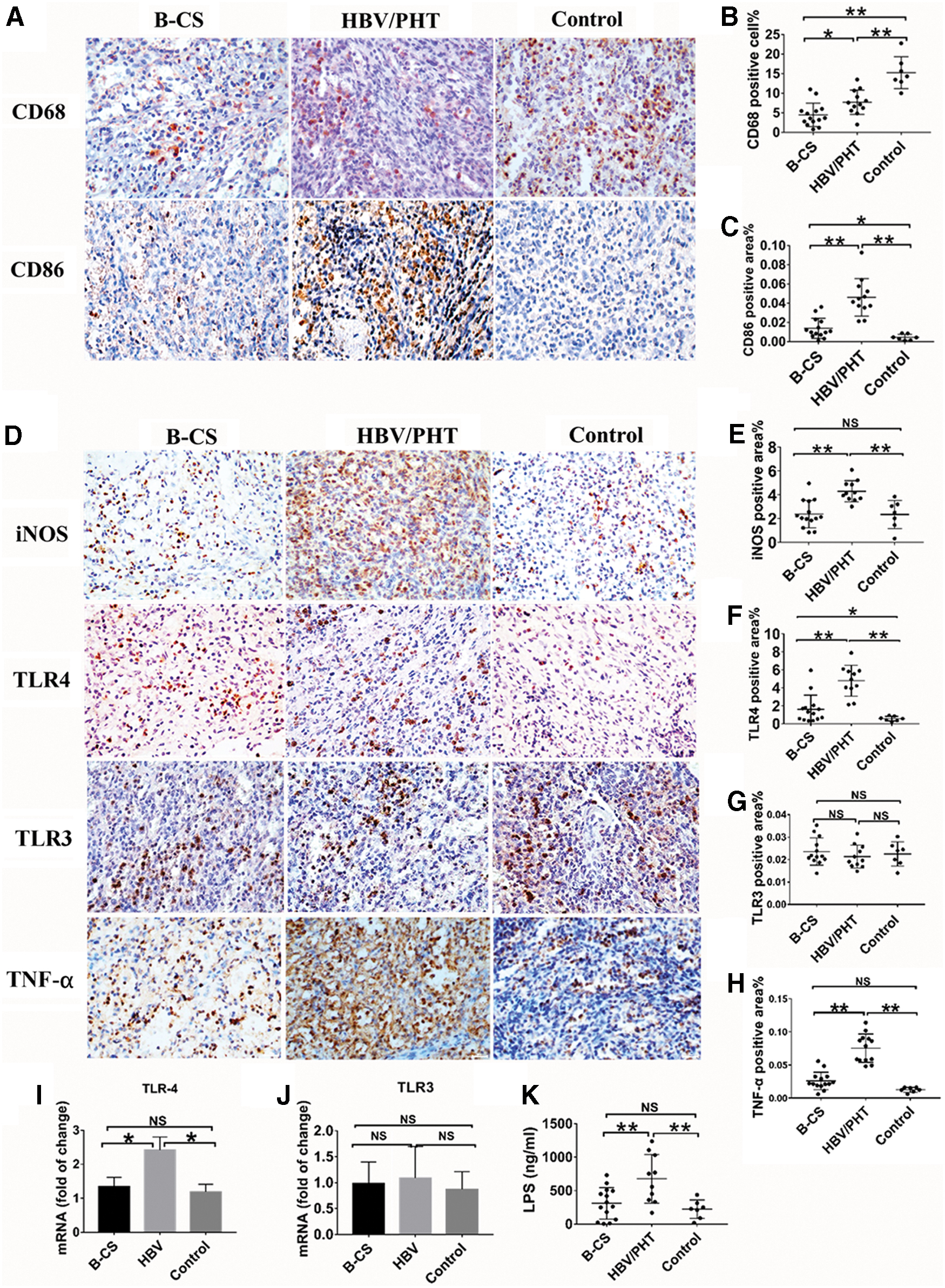
Immunohistochemical staining results of paraffin-embedded splenic tissue sections from the three different groups.
LPS-TLR4 signal pathway is significantly enhanced in spleen from HBV/PHT group but not in B-CS group
The CD86 and iNOS, which were mainly expressed in M1 phenotype macrophages, showed more positive areas in the spleen from HBV/PHT group than B-CS group. TLR4-positive areas not TLR3 in the spleen significantly increased in HBV/PHT group. Also, we detected the plasma LPS level, the ligand of TLR4. The HBV/PHT group showed consistent higher LPS level (677.7 vs. 311.1 vs. 222.1 ng/mL, p = 0.0022) than B-CS and control groups. HBV infection may induce predominant M1 phenotype macrophages by influencing LPS-TLR4 signal pathway but not TLR3 (Fig. 6).
Discussion
China has the highest number of HBV-related cirrhosis patients worldwide. As a severe complication, the mechanism of hypersplenism is complex (5,24). However, most studies have focused on HBV/PHT. To the best of our knowledge, no study has focused on B-CS, which is a special type of PHT without HBV infection. Chinese primary B-CS is quite different from that of Western countries (7,30), including the clinical presentations, etiology, and pathology (29,34,36). Splenomegaly in these cases is the result of high portal pressure in the absence of infection and inflammation (21,35,42). This condition is quite different from HBV/PHT, in which the spleen exhibits both high portal pressure and HBV infection.
Our results support the notion that the mechanism of splenomegaly and hypersplenism in B-CS patients may be somewhat different from that in HBV/PHT patients. Traditionally, the degree of hypersplenism of HBV/PHT does not correlate with the degree of PHT or the spleen size (27). Moreover, the effect of portosystemic shunt in hypersplenism remains controversial (23,27). Our data regarding portocaval shunts showed an efficient increase in the platelet count in B-CS but not in HBV/PHT patients (unpublished data), which suggested that splenomegaly-induced sequestration might contribute more to hypersplenism in B-CS than in HBV/PHT patients. The spleen is deemed to be the main cause of hypersplenism in terms of both sequestration and phagocytosis.
We previously found that the degree of hypersplenism positively correlated with the serum endotoxin and TLR4 levels in macrophages in HBV/PHT patients, suggesting LPS-TLR4 activation in splenic macrophages and subsequently enhanced splenic phagocytosis as well as increasing platelet destruction (18). We emphasize the splenic immune function in the hypersplenism of HBV/PHT. In this study, we found dramatically increased TLR4 expression in spleen and plasma LPS levels in HBV/PHT patients, which showed different splenic platelet destruction mechanisms in HBV/PHT and B-CS patients. In PHT patients, LPS are produced by PHT-related intestinal flora disorder, and its degradation mainly happens in liver. HBV/PHT patients had worse liver function than B-CS patients, which may cause reduction of serum endotoxin degradation, causing higher plasm LPS level in HBV/PHT patients. These results showed hypersplenism in B-CS patients mainly caused by splenic sequestration instead of TLR4-related destruction.
In addition, our study showed entirely different immune statuses between the two groups. Several studies reported that immune function disorders contributed to persistent HBV infection and the immunosuppression status in HBV/PHT (4,6,17). HBV not only causes inflammation but also immune dysfunction and tumors (1). And splenectomy can improve immune dysfunction and benefit bone marrow hematopoiesis (10,11,37). In our study, Tregs and MDSC percentages in the peripheral blood were greater, but CD3+CD4+ and CD3+CD8+ T cell percentages were lower in HBV/PHT patients compared with B-CS patients, which suggested obvious immunosuppression and disordered immune function in HBV/PHT patients (14).
Our previous studies showed differential cytokine expression in portal hypertensive hypersplenic and normal splenic tissues by protein arrays (9). We also found that splenic lymphocytes and macrophages in HBV/PHT patients with hypersplenism had higher absolute numbers and enhanced functions, including phagocytosis and secretion (15,19). iNOS is a major contributor to inflammatory diseases, and macrophages are thought to be the most representative iNOS-expressing innate immune cells (8,20). In this study, we found that HBV/PHT patients had lower percentage of CD68-positive macrophages than control people but higher than B-CS patients. And the IHC results showed that CD86- and iNOS-positive areas in spleen from HBV/PHT patients were dramatically larger than those in B-CS patients, indicating more cell activation and inflammation happened in spleen from HBV/PHT patients.
The limitations of this study include the lack of fresh spleen tissues from B-CS patients for assessing immune functions, because almost all B-CS patients receive transjugular intrahepatic portosystemic shunt or percutaneous transluminal angioplasty treatment at present. Instead, we had paraffin-embedded tissue of spleen to evaluate immune function by IHC. Moreover, hepatic venous pressure gradient (HVPG) may be considered as the gold standard for the degree and severity of PHT. However, as a retrospective study, HVPG was not measured routinely, especially those who underwent open surgery. So we use portal vein diameter and splenic vein diameter as well as PSVR to evaluate the severity of PHT. Although we included 93 B-CS patients' clinical data for analysis, we only had the spleen tissue from 14 B-CS patients, which may cause selection bias. Moreover, even the degree of hypersplenism of HBV/PHT does not correlate with the degree of PHT, the different degrees of PHT between B-CS and HBV/PHT may also cause bias. Our results show different immune functions in the peripheral blood and spleen. The difference may be mainly attributed to HBV instead of PHT. However, the mechanism by which HBV influences splenic immune function requires further clarification.
In summary, the B-CS and HBV/PHT patients had different features of hypersplenism. And HBV/PHT patients had more severe immune disorders in both the peripheral blood and spleen. Regarding the complexity of the mechanism of hypersplenism, the exact mechanism of hypersplenism depends on the etiology. As we all know, treatments for hypersplenism including splenectomy, partial splenic embolization, and splenic artery ligation are common in HBV/PHT patients but rarely in B-CS patients in China (2,36,41). The splenic pathology and immune state change in HBV/PHT patients remind us that treatment for spleen such as splenectomy should be concerned in addition to the treatment of PHT and viral replication.
Footnotes
Authors' Contributions
S.X.L., J.Y., and Z.F.L. designed the research; S.X.L., N.H., Z.Z.L., and C.Z. performed the research; S.X.L. and X.W.D. collected the clinical data and samples; S.X.L., L.L., A.J., and G.Y.K. analyzed the data; S.X.L. and X.W.D. wrote the first draft of the article; F.P.J., G.Y.K., J.Y., and Z.F.L. revised the article; all authors have read and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study is supported by grants from the National Natural Science Foundation of China (91842307) and Key Research and Development Projects of Shaanxi Province (2017ZDCXL-SF-02-05).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.