
Abstract
Pakistan is ranked second highest after Egypt in hepatitis C virus (HCV) infection. Accurate typing is mandatory to be compliant with the World Health Organization strategy to eliminate HCV infection in 2030. We characterized the HCV genotypes using Abbott real-time polymerase chain reaction assay and indeterminate samples were sequenced. We also investigated the distribution of HCV genotype among different age groups and gender in chronic HCV patients. One thousand thirteen samples were tested for HCV genotyping using Abbott real-time HCV genotyping assay. RNA extraction from plasma was done using the m2000sp platform. The amplification and detection of genotypes was done on m2000rt instrument. The lower limit of detection assay is 500 IU/mL. The indeterminate genotypes were analyzed by sequencing of the NS5B region. We found genotype 1 in 1.68%, genotype 1b in 0.89%, genotype 1a in 0.79%, genotype 2 in 0.6, genotype 3 in 94.37%, genotype 4 in 0.4%, genotype 5 in 0.09%, and indeterminate genotype result were found in 1.18%. Abbott assay could not identify 12 samples of genotype 3 (1.18%) and gave the indeterminate result. It also fails to assign some of the samples of genotype 1 into 1a and 1b. The indeterminate genotypes were resolved by sequencing followed by phylogenetic analysis. Genotype 3 is the predominant genotype and significantly higher in females as compared with males. Genotype 1a is more common in males than in females. Indeterminate HCV genotypes on sequencing analysis identify as genotype 3a and likewise subtype of genotype1 as 1a.
Introduction
Hepatitis C virus (HCV) was first recognized in 1989 and emerged as a serious health problem around the globe. The most prevalent areas are central and East Asia, the Middle East, and North Africa. HCV spreads through blood and body fluids, and is responsible for chronic liver disease, cirrhosis, and hepatocellular carcinoma (22,42). World Health Organization reported that ∼399,000 HCV-infected persons died annually due to cirrhosis and hepatocellular carcinoma (27). In Pakistan, eight million people have exposure to HCV and showed second-highest number of HCV infections in the world (15). It represents family flaviviridae and genus Hepacivirus. HCV is an RNA virus with a mutation rate due to replication errors by RNA-dependent RNA polymerase (6,14,40).
Variability of HCV genome classifies into different genotypes and subtypes. Different genotypes have <70% nucleotide homology that leads to the difference in the structure of the encoded protein. Genotype distribution of HCV varies geographically as suggested by epidemiological data. The management of HCV patients has revolutionized with the use of direct antiviral therapy as it increases the sustained response and reduces the risk of developing liver cirrhosis. However, HCV genotypes identify as a key determinant of antiviral efficacy (33,39). Therefore, knowledge of a genotype before initiation of antiviral treatment of an infected individual has importance for the clinician because it helps in deciding for treatment duration and stratification of HCV groups (13). Moreover, the genotype is also useful for investigating outbreaks of infection and for understanding the epidemiology, virologic features of the virus, and improvement of HCV diagnostic tests (5).
HCV is also a major risk factor for HCC as chances of HCC increase 17-folds in HCV-infected patients as compared with HCV-negative patients (11). A number of studies reported that a liver cirrhotic patient infected with HCV genotype 1b has high risk of developing hepatocellular carcinoma than a patient infected with other HCV genotypes (9). In contrast, some studies reported no clear relationship between genotype and hepatocellular carcinoma (30,32).
The worldwide distribution of HCV genotypes is variable. HCV genotype 1 and 3 collectively causes 67.0% infection worldwide (31). These two genotypes are prevalent globally. Genotype 3 has significant growth and appears as the second most common genotype in Europe, except Italy and Romania (3). In Latian America, North America, and in Europe genotype 1 is predominant ranging from 64.4% to 83%. While African and middle eastern population is infected with genotype 4 (65.3%). In Asia, two genotypes are commonly found, genotype 3 (22.4%) and genotype 1 (46.6%). However, South East Asian region, including Pakistan and India, has higher percentage of HCV genotype 3 (79.0%) and genotype 1 (54.4%). In Australasia genotype 1 is higher (55.0%) followed by genotype 3 (25.5%) (31). Genotype 2 is found in West Africa (62.9%) and some parts of South America. Possible entry of genotype could be through transatlantic slave trade in the 18 century. Genotype 5 is found in the northern part of South Africa (39%). Sporadic cases were also found in France, Syria, Saudi Arabia, and Canada. Genotype 6 is found in South East Asia and genotype 7 was reported in immigrants in Canada from Central Africa. (24).
Different methods for genotyping are available. In our study, we used real-time (Abbott) HCV genotype assay based on the probe that targets the noncoding region along with nS5b region. However, it has the drawback of giving a small percentage of indeterminate results due to the presence of mutation at the binding site of genotype-specific probes. These indeterminate genotypes analyzed by sequencing of the NS5b region, were considered gold standard and a reliable method for accurate prediction of HCV genotypes (12,25). The aims of our study were: (1) to figure out the distribution of HCV genotypes and probe its association with gender and age; (2) to find success and failure of HCV genotyping method in terms of indeterminant results; and (3) to perform NS5B Phylogenetic analysis of indeterminate HCV genotypes.
Materials and Methods
Patient selection
Patients >18 years of age with positive polymerase chain reaction (PCR) for HCV were enrolled in the study. None of the patients had antiviral therapy. Patients who were positive for hepatitis surface antigen, and negative for HCV RNA were excluded. A total of 1,013 PCR-positive samples were recruited at NORI Hospital from January 2017 to June 2018. Out of total study population, 422 subjects were male and 591 were females. Most of the patients were in the >40–50 years of age range (Table 1). The study was approved by the Ethics Committee of the institute. The laboratory is ISO 9001 2015 certified and HCV genotyping test is accredited with ISO 15189:2012. Moreover, our laboratory is enrolled in external quality control program QCMD Glassgow UK and the eluates are transferred.
Basic Characteristic of the 1,013 Patients Infected with Hepatitis C Virus
ALT, Alanine Aminotransferase.
Sample collection and HCV RNA extraction
Three milliliters of venous blood was collected in a vacutainer tube having EDTA. Plasma was separated after centrifugation at 4,000 rpm and stored at −80°C until tested for genotyping. RNA extraction from plasma was done using the m2000sp (sample preparation system platform). In this procedure, magnetic particles were used to capture HCV RNA. Unbound components are removed by washing the microparticle. Bound HCV RNA is eluted from the particles and collected in 96-well plates. Moreover, m2000sp prepare & dispense master mix (amplified reagents) to the extracted RNA in deep 96-well plates. Internal control sequence not related to HCV genome added to each sample amplified to confirm the extraction has been processed correctly for samples and control.
HCV genotype detection
HCV genotyping performed by using the Real-Time HCV Genotype Kit. Abbott real-time HCV genotyping is a reverse transcriptase-based assay performed according to the manufacturer's instructions. It has a unique feature to determine the subtype of genotype 1. Four sets of primes are used, one set of primer amplified 5′UTR (untranslated region) of all HCV genome and confirmed the presence of RNA, second set was used to amplify an NS5b region of genotype 1a, a third set amplified NS5b region of genotype 1b of the HCV genome, and the fourth set of primer amplified internal control sequence. The deep 96-well plate was transferred to the m2000rt instrument for amplification and detection of genotypes (Table 2). Product and internal control both amplified in m2000rt (thermal cycler). Positive and negative control samples were processed in the same manner as the clinical sample.
Assay Probes and Detection of Fluorescence
The assay has three separate reaction tubes for the detection of HCV genotype 1 to 6 and subtype 1a and 1b. Reaction in tube A detect all HCV isolates on FAM, genotype 1a on VIC, and genotype 3 on NED channel or dye. Reaction in tube B detects genotype 2 on FAM, genotype 1b on VIC, and genotype 1 on NED channel. Reaction in tube C detects genotype 2 on FAM, genotype 1b on VIC, and genotype 1 on NED channel. Probes at 5′ end labeled with fluorescent moiety and hybridized with their respective amplification target. During the polymerization step of PCR rTth polymerase perform exonuclease activity, degrading the probe result in separation of quencher and fluorophore ultimately allows the detection and emission of resultant fluorescence on their respective channel in m2000rt system.
HCV, hepatitis C virus; PCR, polymerase chain reaction.
The lower limit of detection assay was 500 IU/mL. It is defined as an assay that has a probability of 95% of viral load concentration and accurate HCV genotype detection (viral load for accurate HCV detection). Genotypes were detected in three separate reactions as shown in Table 2. Indeterminate genotype results were noted. It means that the assay detects the HCV or the clinical sample is HCV positive, but does not give specific genotype results. The indeterminate result ensured the sample has an HCV concentration of 500 IU/mL. The assay manufacturer reported an accuracy of the assay as 98.28% when compared with nucleotide sequencing. Agreement in assay and nucleotide sequencing for genotype 1a is 97.27% and for genotype 1b is 96.55%.
Sequencing and phylogenetic analysis
The sequence of indeterminate genotypes was also analyzed by the blast to identify the correct genotype and subtypes based on the percentage identity of the blast. The sequence of the NS5B gene of different HCV genotypes was retrieved from GenBank and compared with sequence reported from HCV genotype indeterminate results and genotype 1. Sequences were first aligned and then further used for phylogenetic analysis using CLC workbench software. Phylogenetic analysis segregates the sequence into a distinct type. The tree was drawn using the neighbor-joining method. No one sequence has a percentage blast identity <90%.
Statistical analysis
SPSS V. 16 was used for analysis. Percentages and frequency of HCV genotypes were calculated. Age of population was presented as mean ± standard deviation. Distribution and frequencies of HCV genotypes and age of HCV-infected patients were determined using descriptive statistics. Chi-square test was used to find the association of age of patients with HCV genotypes. P-value <0.05 was considered significant.
Results
HCV genotypes were conducted among 1,013 specimens who were HCV infected. Among them, 592 (58.4%) are female and 421 (41.6%) are male. The Abbott real-time GTII Kit gives analytically accurate and sensitive result for all virus types at 500 IU/mL, which is the detection limit of the assay. Frequency of HCV genotype 3 (94.37%), genotype 1 (1.68%), genotype 1a (0.79%), genotype 1b (0.89%), genotype 4 (0.4%), genotype 5 (0.09%), and 12 (1.18%) patients showed indeterminate genotype result. None of the sample showed coinfection.
To determine the distribution of HCV genotype according to age, patients were categorized into five age groups as shown in Figure 1. Genotype 3 was more common in females of age group >40–50 years (31.84% of 581) followed by >30–40 years (23.6% of 581). In males HCV genotype 3 is more frequent in age group >40–50 years (24.2%) and >50–60 years (24.8%) followed by >30–40 years (21.5%). Subtype 1a was common in male patients (71.42% of 26) than female patients (42.85% of 26, p = 0.043). Subtype 1a was found higher in the age group >30–40 years. According to gender and age, higher incidence of genotype 1a was found in females patients who were >30–40 years (44.4% of 9) than male (33.3% of 15, p = 0.045). Genotype 1b was observed higher in younger male patients. Genotype 4 and 5 were only observed in male patients. Genotype 4 was found only in age groups >40–50 years and genotype 5 was found only in the age group >60–70 years.
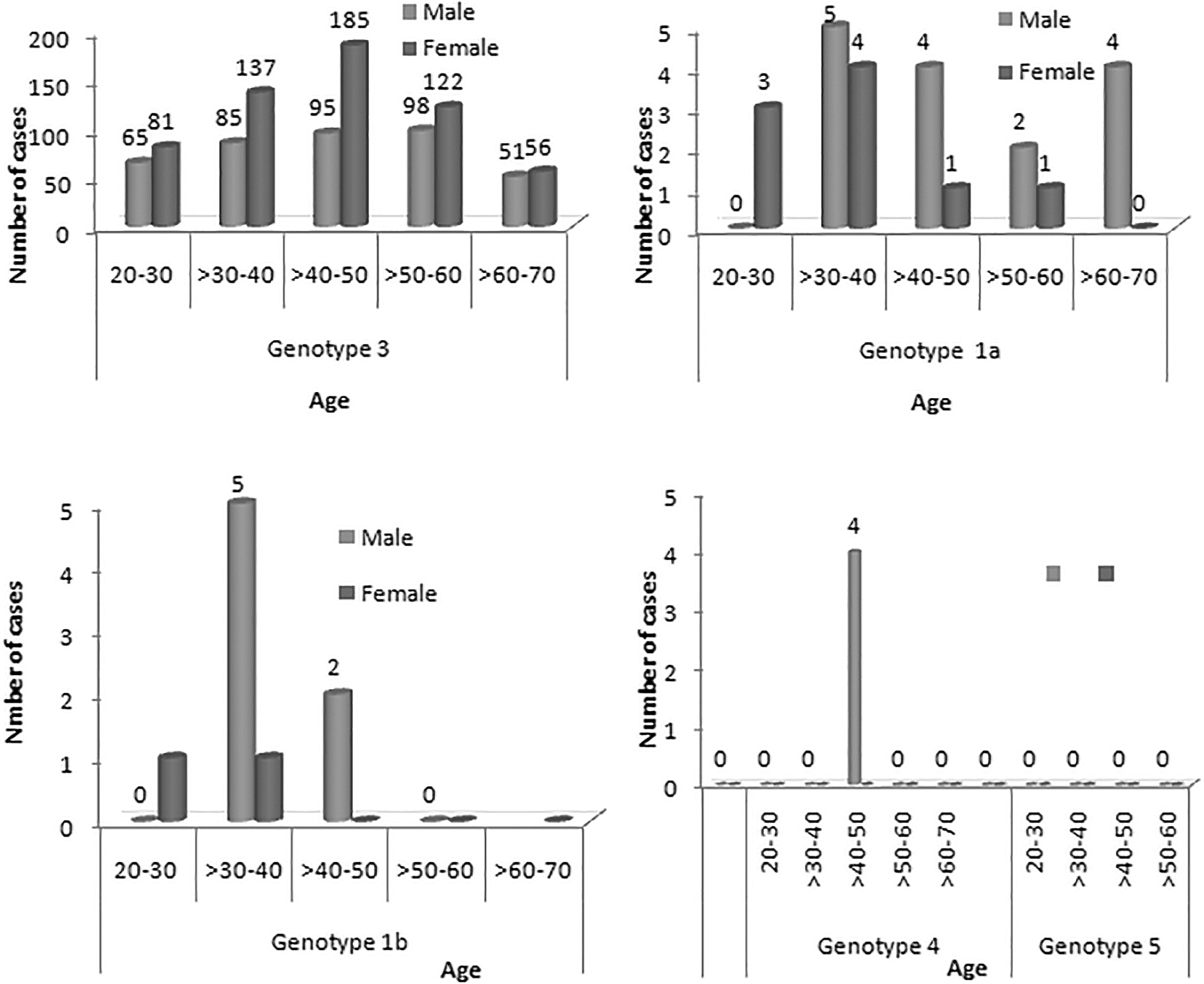
The distribution of HCV genotypes in different age groups and gender.
The disadvantage of genotype assay was that it gave indeterminate results. The patient's sample having indeterminate results were further tested by sequencing. All these samples showed results of the genotype 3a. Abbott test can identify subtypes of HCV genotype1 as 1a and 1b, whereas 17 (1.67%) samples identified as genotype 1 without assigning a subtype. It was also unable to identify the genotype result of 12 (1.18%) samples and gave an indeterminate result (Table 3). These samples had their viral load results in the range from 3 × 103 to >3 × 106 IU/mL, which is above the detection limit of the assay.
Distribution of Hepatitis C Virus Genotypes
Genotypes detected by Abbott real-time: Results of HCV genotypes determined by using Abbott real-time PCR.
Genotypes detected by NS5B sequence analysis: HCV genotype showed results indeterminate genotypes and HCV genotypes not differentiated into 1a and 1b by Abbott real-time PCR resolved by NS5B sequencing.
These samples were retested for subtype identification by sequencing. All the samples were successfully amplified for NS5b region and sequencing was performed, followed by phylogenetic analysis to determine the subtypes. Blast search against sequence result was done in the GenBank database for the NS5B-amplified region. The sequence showed >94% similarity retrieved from the database. All the sequences were aligned and genotyping classification was confirmed by phylogenetic analysis. The result indicates that the phylogenetic tree of NS5b sequences divided all the genotypes correctly. The analysis identifies the subtype of genotype1 as 1a (Fig. 2). Moreover, indeterminate HCV genotypes identify as genotype 3a using sequence analysis followed by phylogenetic analysis of the NS5B region of the HCV genome; moreover, their nucleotide similarity with GenBank sequence (accession nos. KY620642.1, GU814263.1, KF035125.1, JQ717256.1, GU814263.1, KP324141.1) revealed that they did not predict as new variants (Fig. 2). Patient sample classified as genotype 1 by Abbott real-time clustered with a sequence of genotype 1a from U.S. (accession nos. KC 127258.1, KC127412.1, HM746812, AY100118.1, HQ661847.1, AY682778.1, MG453599) and Brazil. No crossreactivity among genotype has been observed (Fig. 2).
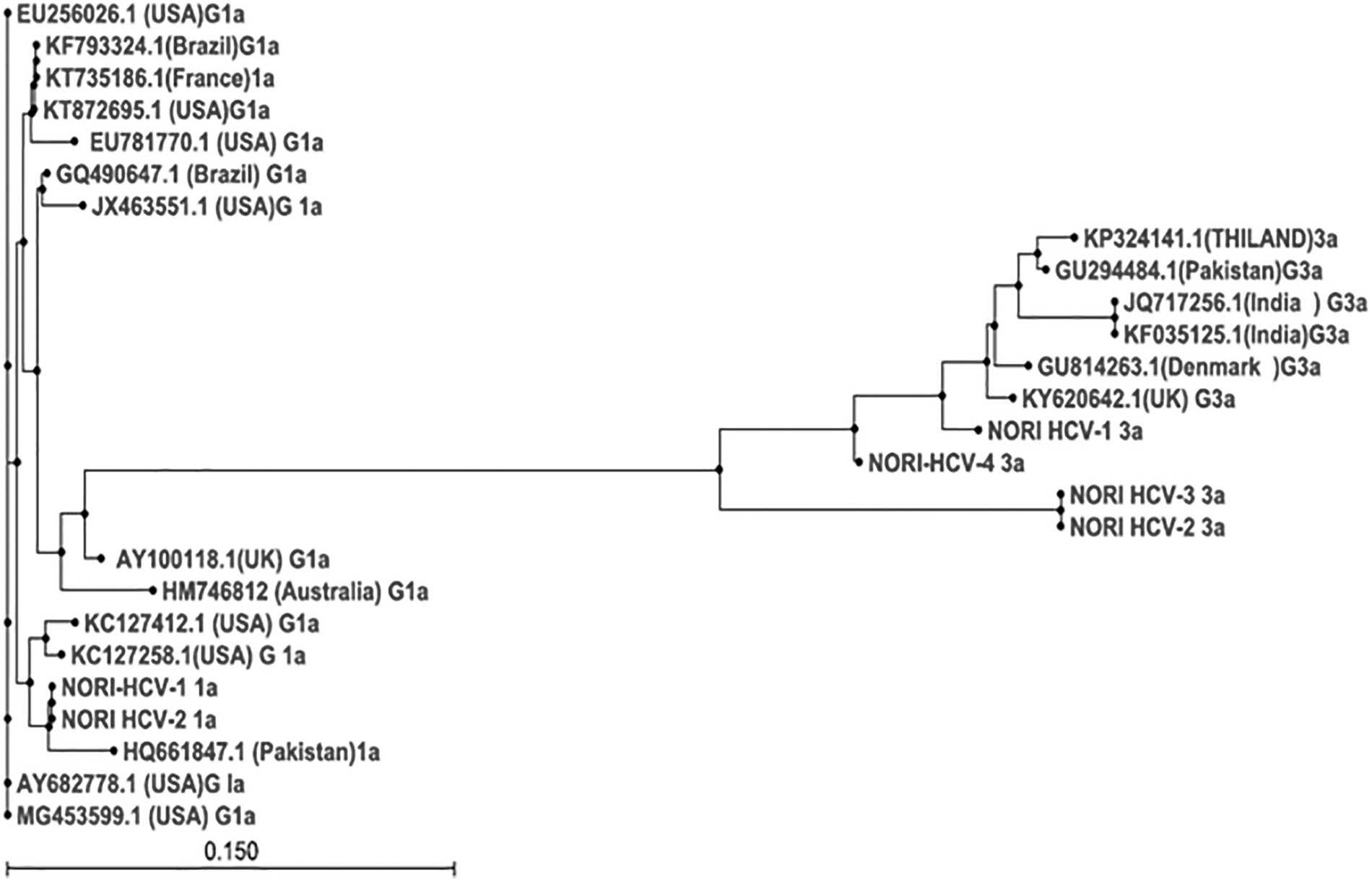
Phylogenetic analysis of HCV isolates collected from HCV-infected patients based on nucleotide sequences of NS5b region. The tree was constructed by a neighbor-joining method using program CLC workbench. Sequence of HCV isolates resulted by Abbott real-time into genotype 1 and indeterminate indicated by name as NORI HCV 3a and NORI HCV 1a. Reference sequences indicated by accession number and downloaded from NCBI database. HCV, hepatitis C virus.
Discussion
The major cause of chronic viral hepatitis is HCV, classified into genotypes and subtypes based upon their genetic sequence. The geographical distribution of HCV is distinct. The genotype is the key element of clinical management of HCV because the response to treatment varies according to genotypes (27). Knowledge of genotypes helps to understand the migration pattern and provide vital information to the resource-constrained health care system for the optimal management of HCV and implement policies and guidelines for the access of direct antiviral therapy globally. Moreover, knowledge of HCV genotype guides the physician to choose the right drug regimens as recommended by EASL (European Association for the Study of the Liver). World Health Assembly approved health strategy on a global level to eliminate HCV infection by 2030. Herein lies a key benefit; accurate identification of HCV genotype gives information about the burden of disease that helps the authorities in making a national strategy for eradication on the basis of the current distribution pattern of HCV genotype. Our objective was the determination of HCV genotype using Abbott real-time and disagreement observed was resolved by sequence analysis of NS5b of HCV. However, real-time genotype identification system has an advantage in terms of turnaround time and ease of genotype result interpretation as compared with sequencing (19).
Finding of the study showed that genotype 3 was the predominant genotype (94.3%), which is in accordance with the other studies that reported high endemicity of genotype 3 from Pakistan and neighboring countries like India, Nepal, Bangladesh, and Iran (10,17,21). Genotype 1 was found to be 3.3% (34/1,013), other studies from Pakistan also confirmed the presence of genotype 1 as the second-most genotype found in the HCV-infected population in the Punjab province of Pakistan (4,43). Subtype 1a (0.79%) and 1b (0.88%) of genotype1 has also been seen. The frequency of genotype 1, 1a, and 1b among HCV-infected patients is lower than that reported globally (21). Scientific data reported that mostly genotype 1 is prevalent (46%) followed by genotype 3 (22%), genotype 2 (13%), and 4 (13%) (15,36). Another study reported the distribution of genotype on a global level and showed that genotype 1 is dominant on other genotypes. Genotype 3 consisted of 25% and genotype 4 is 15% of the global burden of HCV genotypes (7). It has also been reported that genotype 3 is predominant in lower middle-income countries and genotype 1 is dominant in North America, Latin America, Europe, and Australia. The previous reports mentioned that it is responsible for chronicity and cirrhosis.
Reoccurance of HCV infection in liver transplant patient was also reported (16). Another report predicts the genotype 1 linkage with hepatocellular carcinoma (41,44). Subtyping of genotype 1 to differentiate 1a and 1b needs to be identified before starting direct antiviral because treatment regimens are still genotype specific (28,29). However, current treatment protocols have not considered subtype differentiation of HCV genotype as an important component. While the earlier report reflects that patients with HCV subtype 1b have a worse prognosis than those with type 1a. The addition of NS5B target region for genotype analysis improves subtyping of genotype 1 identification (20). In contrast with the previous report, we observed that assay is unable to identify subtypes 1a/1b of genotype 1 in 1.68% of patients. This finding is in agreement with Liu et al. (18) who reported assay failure to identify subtyping of HCV genotype 1 in 10% of cases. These sequences aligned with the sequence reported from Pakistan, U.S., UK, and Australia. This genotype may have entered in Pakistan through cross-border migration for jobs and trades. Our finding agreed with the statement that immigration and travel may alter the epidemiology of these uncommon genotypes (types 4, 5, and 6) (2).
We found HCV genotype 4 in 0.4% of the studied population, this genotype is uncommon and finding conforms with other reports (4). However, genotype 4 is highly prevalent in gulf countries such as the United Arab Emirates and Saudi Arabia, Egypt, Oman, and Yemen (1,34,38). The presence of genotype 4c has been reported in low-income countries, while in Europe its prevalence was higher in intravenous drug users (7,37). In Saudi Arabia, genotype 4 represents 74.2% of HCV-infected patients. The presence of genotype 4 in our study population can be attributed to the fact that a substantial number of expat work and stay for a longer period in middle eastern region. However, comparison data showed that the distribution of HCV genotype differs from Gulf countries.
Distribution of genotypes in different age groups contributes positively to refine preventive and therapeutic strategies. Studies from different countries reported the distribution of HCV genotypes in relation to gender and age. Brahim et al. reported that the distribution of HCV genotype 1 has an association with the male, whereas genotype 4 has been more commonly found in females (8). Niu et al. reported that some HCV genotypes are more prevalent in male than in the female. Some studies clearly showed that there is no variation among HCV genotype distribution in the male and female gender. In other words, the distribution of genotypes have a similar ratio in females and males (26). However, in the present study, the frequency of some genotypes is more prevalent in females compared with males. For instance, the frequency of HCV genotype 3 was higher in females than males. Moreover, genotype 1a distribution is higher among male than female patients. Female preponderance in our study population can be attributed to more exposure to blood or blood products and injection during their reproductive cycle, or piercing of nose and ears. Distribution of HCV genotype showed variation in different age groups. HCV genotype 3 was observed among all the five age groups of males and females. However, Niu et al. reported increased frequency of genotype 3 among the younger population. Other studies from the U.S. and Europe also reported the distribution of nongenotype 1 in younger patients (26).
HCV genome has high variability, however, reports are available that shed light on nonidentification of subtype 1a and 1b (23,35). These strains are correctly identified as genotype 1a through phylogenetic analysis of the sequence of NS5B region. One of the possible reasons for HCV indeterminate result may be that the probe binding site of the target sequence has some nucleotide variation. Additionally, high genetic variability of HCV compromises its detection on real-time assays. This warrants further re-evaluation by sequencing. The importance of sequencing needs to be highlighted as its detection will help in accurate clinical management by genotype and subtype-specific antiviral. Moreover, it helps to identify rare subtypes and missubtypes which helps in the identification of the target population for using pangenotyping therapy for the elimination of HCV. Thus, findings of our study confirm the accurate genotype and subtype identification crucial for treatment success and ultimately for the eradication of hepatitis C in the Pakistani population.
Conclusion
Genotype 3 is predominant among HCV patients. Genotype 4 and 5 have low prevelance, hence a low risk of transmission from high endemic areas. Our study also showed the limitation of Abbatt real-time system, as it fails to assign genotype to some of the samples of genotype 1 into 1a and 1b. It also gives indeterminate result for some of the genotype 3, which has to be resolved by sequencing. Therefore, sequencing of NS5B may be used as a supplementary approach for accurate genotyping and identification of rare subtypes.
Footnotes
Authors' Contributions
All authors contributed equally to the design and writing of this article.
Ethics Approval
The study was approved by Ethics Review Boards from Nuclear Medicine, Oncology, and Radiotherapy.
Informed Consent
Informed consent from each patient/relative of the patient was obtained during the collection of the sample.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.