
Abstract
Chikungunya fever, a disease caused by chikungunya virus (CHIKV), reemerged and affected over 52,000 people in southern Thailand in 2008 and 2009. The CHIKV strain involved in this outbreak was the East Central South African (ECSA) strain with the E1-A226V mutation. The prevalence of CHIKV-associated chronic discomfort varied by virus lineage. This retrospective cohort study aims to describe the CHIKV-related symptoms persisting in CHIKV-affected patients, related factors, and the presence of anti-CHIKV immunoglobulin G (IgG) antibodies 5 years after the onset of disease. From 5,344 of the study population screened, a total of 89 affected patients reported persistent arthralgia 5 years after the disease onset (nonrecovery rate = 1.7%). Of the 141 affected patients enrolled, 122 cases (86.5%; 77 cases with persistent arthralgia and 45 cases of fully recovered) still had detectable levels of anti-CHIKV IgG antibodies. Long-term persistence of chronic joint symptoms is associated with the severity of the disease during the initial phase of the infection, but not gender, age, or comorbidities. The common manifestations were arthralgia (75.3%), morning joint stiffness (39.0%), muscle pain (19.5%), and occasional joint swelling (16.9%). Chronic joint symptoms could occur in either a fluctuating or a persistent manner and usually caused moderate pain. The joints affected were mainly fingers (71.4%), wrists (51.9%), and knees (50.6%). Most patients had polyarthralgia with symmetrical joint involvement. In some cases with persistent arthralgia, atypical manifestations, including severe depression with suicide attempts, severe weight loss, and severe hair loss, were found, and some patients still experienced severe joint pain.
Introduction
Chikungunya fever is a reemerging disease caused by chikungunya virus (CHIKV) that is transmitted to humans by mosquitoes (8,33). In 2008–2009, an outbreak occurred in southern Thailand. By December 2009, CHIKV had spread to other parts of the country, affecting more than 52,000 people in 2009 (22). CHIKV infection results in an acute febrile illness. The classic clinical symptoms are high fever, severe polyarthralgia, myalgia, and fatigue. The other symptoms include headache, skin rash, nausea, and vomiting (6). Polyarthralgia is the most important feature of CHIKV infection and primarily affects not only the small joints of the wrists and fingers but also affects the large joints, such as the elbows, shoulders, and knees (6,36). Severe CHIKV infection can also result in nonspecific or atypical manifestations, including neurological, cardiovascular, renal, skin, and ocular manifestations. These atypical manifestations can have serious consequences for patients (32). Overall, the disease is self-limited. Most CHIKV-infected patients recover from severe joint pain within several weeks (6, 28). However, some patients have persistent joint pain, joint swelling, morning stiffness, and other nonspecific symptoms for months or years (3,6,10,13,18,28,37,38,40).
The CHIKV strain that was involved in the outbreak in southern Thailand during 2008–2009 is the East Central South African (ECSA) strains with the E1-A226V mutation (34). A systematic review and meta-analysis reported that the proportion of people who do not fully recover after chikungunya was high. After 12 months follow-up, the overall nonrecovery rate was 21% (95% confidence interval [CI]: 19–22%). In addition, the prevalence of CHIKV-associated chronic symptoms varied by virus lineage (28). While there are numerous reports of chronic CHIKV-related symptoms, little is known about long-term clinical manifestations in a group of patients infected with CHIKV from southern Thailand during 2008–2009, 5 years after the acute phase of CHIKV fever. The aim of this study was to describe the persisting clinical manifestations in CHIKV-infected patients, related factors, and the presence of anti-CHIKV immunoglobulin G (IgG) antibody 5 years after the acute phase of CHIKV fever in a group of CHIKV patients from southern Thailand.
Patients and Methods
Study design and participants
This was a retrospective cohort study conducted in CHIKV-affected patients during an outbreak in 2008–2009. Participants were recruited from patients diagnosed or suspected to be infected with CHIKV during the outbreak in Nakhon Si Thammarat province and Phatthalung province, southern Thailand, using convenience sampling. Ten primary health care services in these two provinces, where clinically suspected or diagnosed cases were reported during the outbreak, were included in this study covering a total of 35 villages in Nakhon Si Thammarat province and a total of four villages in Phatthalung province. All affected people in the responsibility of each primary health care services were screened. The clinical data and related factors were collected between April 2013 and September 2014, which was 56–60 months after the acute illness.
Selection criteria
All CHIKV-infected patients who still had CHIKV-related symptoms were invited into this study. In the context of the epidemic, patients had been suspected to be infected with CHIKV based on epidemic data and initial clinical symptoms during the outbreak, having both fever and severe joint pain at disease onset. The subjects were assigned to one of two groups: (1) persistent arthralgia and (2) full recovery. Subjects were considered to have persistent arthralgia if they claimed to still be having joint manifestations at the time of the interview or had experienced at least one relapse within the past 8 days (18), and were considered to be fully recovered if they did not have chikungunya complaints any more during the survey. The participants who had any history of chronic arthritis or joint manifestations before the outbreak were excluded from the study. The fully recovered subjects were matched for sex, age, comorbidities, and community with persistent arthralgia cases. The study was approved by the Ethics Committee of Walailak University. Written informed consent was obtained from all participants.
The characteristics of the patients and disease
The characteristics, CHIKV-related symptoms, and related factors of the patients were assessed. This included gender, age, time since acute chikungunya infection, past illness or known underlying chronic diseases, the initial clinical symptoms, and the persisting clinical manifestations. The pain scores were self-reported by the patients, and the severity of joint pain was assessed using a verbal numeric rating scale. The patients were asked to rate their experience of pain using numbers from 0 (no pain) to 10 (worst pain). Patients with persistent arthralgia were subdivided into severe and nonsevere pain groups. The subjects were classified as having severe pain if they claimed to have joint pain every day and had a pain score >6.
All patients included in this study were examined for the presence of anti-CHIKV IgG antibody using an indirect immunofluorescence technique (IIFT) with a commercial kit (Euroimmun Anti-CHIKV IIFT; Euroimmun) according to the manufacturer's protocols and as described previously (14,19,26,31). The cutoff point for positive was at an antibody dilution of 1:10.
Statistical analysis
The results for the continuous variables are expressed as the median ± standard deviation, median (interquartile range), range (minimum to maximum), or mean ± standard error according to data distribution. The categorical variables were expressed as percentages. The data were analyzed using SPSS 17.0 (SPSS, Inc., Chicago, IL). Statistical comparisons were performed using an independent t-test or one-way analysis of variance for continuous data with a normal distribution and using a Mann–Whitney U or Kruskal–Wallis test for continuous data with the nonnormal distribution. A Fisher's exact test or a chi-square test was used for the categorical variables. Significant differences were indicated when p < 0.05.
Results
In a total of 35 villages in Nakhon Si Thammarat Province and a total of 4 villages in Phatthalung Province, we found that nearly all of the affected patients during the outbreak were fully recovered. From 5,344 study population, a total of 89 patients (1.7%) claimed to still be having joint manifestations or CHIKV-related symptoms 5 years after the onset of the disease. The study population and the number of cases identified and enrolled are detailed in Figure 1.
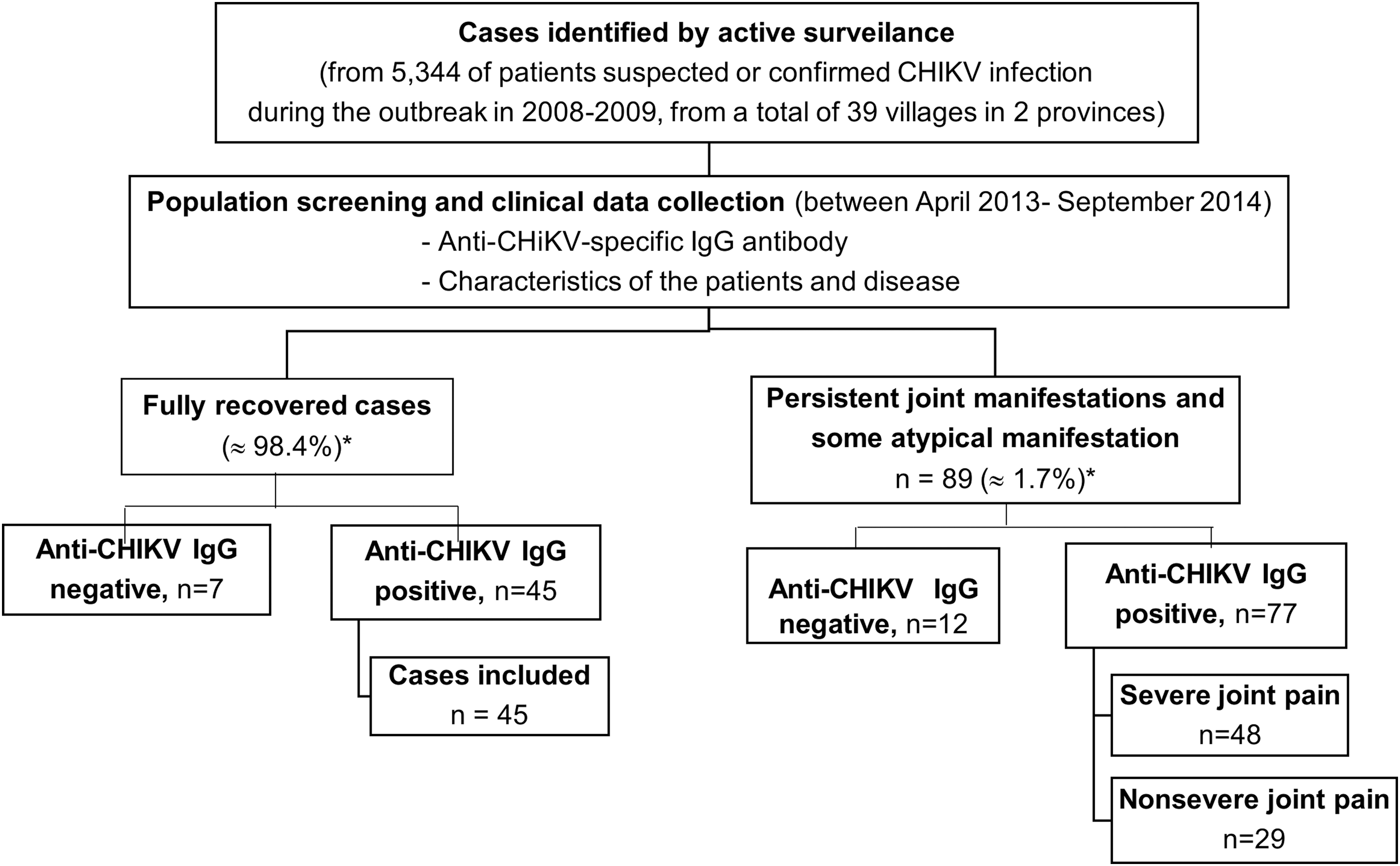
The study population. *As calculated from the total number of patients identified.
The presence of CHIKV-specific IgG antibody in serum at 5 years after the acute phase of infection
For the serological follow-up, sera from a total of 141 patients affected by CHIKV fever during the outbreak in 2008–2009 were examined for the presence of anti-CHIKV IgG antibody using the IIF technique (89 cases of persistent arthralgia and 52 cases of full recovery). Of the 141 affected patients examined, 122 cases (86.5%) were positive for the anti-CHIKV IgG antibody up to 60 months after CHIKV infection, 77 cases of persistent arthralgia and 45 cases of full recovery. Anti-CHIKV IgG antibody could be detected in both the persistent arthralgia and full recovery groups, and there was no significant difference in persistence between these two groups (Table 1).
Prevalence of Anti-Chikungunya Virus Immunoglobulin G Antibody in Patients Affected by Chikungunya Virus After 5 Years of the Disease Onset
The mean difference was significant at the 0.05 level.
The cutoff point was at an antibody dilution of 1:10.
CHIKV, chikungunya virus; IgG, immunoglobulin G.
The characteristics and clinical data collection
The characteristics of CHIKV-affected patients and CHIKV-related symptoms were analyzed and compared between persistent arthralgia and full recovery cases who were anti-CHIKV IgG positive.
The baseline characteristics of CHIKV-affected patients in both persistent arthralgia and full recovery group are shown in Table 2. The majority of CHIKV-affected patients who participated in this study were women. In terms of gender, age, and underlying diseases, no significant differences were observed among the persistent arthralgia group and the full recovery group. The median duration since acute CHIKV fever was 53.8 months with an interquartile of 56–60 months. There were statistically significant differences in pain intensity during acute illness between patients who still having joint manifestations and those who were fully recovered (p < 0.001). Moreover, nearly all (98.7%) of persistent arthralgia cases had severe joint pain during acute illness.
Baseline Characteristics of Anti-Chikungunya Virus Immunoglobulin G Positive Patients Comparison Between Persistent Arthralgia and Full Recovery Group
Significant differences were indicated when p < 0.05.
n, number of patients; SD, standard deviation.
The self-reported underlying chronic diseases in patients with persistent arthralgia are shown in Table 3. The most commonly reported comorbidities were hyperlipidemia and hypertension. Other included diabetes mellitus and allergic diseases. The known incidence of underlying chronic diseases or comorbidities was not significantly different between the persistent arthralgia and full recovery groups.
The Underlying Chronic Diseases Comparison Between Persistent Arthralgia and Full Recovery Group
Significant differences were indicated when p < 0.05.
Multiple answers were possible.
Baseline characteristics of persistent arthralgia patients were compared between the severe and nonsevere pain group. Of the 77 patients with persistent arthralgia, 48 cases (62.3%) had severe joint pain, and 29 cases (37.7%) had nonsevere joint symptoms. Gender, age, duration since the acute stage of CHIKV fever, and comorbid conditions were not significantly observed between the severe pain and nonsevere pain, as shown in Table 4.
Baseline Characteristics of Persistent Arthralgia Patients Comparison Between the Severe and Nonsevere Group
Significant differences were indicated when p < 0.05.
The musculoskeletal manifestations and some atypical manifestations reported by patients with persistent arthralgia after 5 years of the disease onset are shown in Table 5. The common manifestations consisted of joint pain, morning joint stiffness, muscle pain, and joint swelling. Of the 77 patients with persistent arthralgia, 5 cases (6.5%) had atypical manifestations. These atypical manifestations included severe depression with suicide attempts, severe weight loss, and severe hair loss. Notably, all five patients who had these atypical manifestations had severe joint pain or had joint swelling.
Disease Characteristics in Patients with Persistent Arthralgia at 5 Years After the Disease Onset
Multiple answers were possible.
In patients with persistent arthralgia, the main joints affected were the small joints in the fingers and wrists. However, the affected joints could also be large joints, such as the knees, ankles, elbows, hips, and shoulders, as shown in Table 6.
Frequency of Reported Anatomic Pain Locations in Persistent Arthralgia Patients at 5 Years After the Disease Onset
Multiple answers were possible.
The characteristic of persistent joint pain and pain intensity reported by CHIKV-infected patients 5 years after the disease onset are shown (Table 7). Most patients with persistent arthralgia had polyarthralgia (79.2%) with symmetrical joint involvement (98.7%). The pain usually persists every day (66.2%). The pain score ranged from 2 to 9. The pain intensity was often moderate (pain score 4–6; 62.3%), and the median and mode of the pain score were 5.0. All of our subjects reported less severe pain after infection than during the acute phase of CHIKV fever.
Characteristics of Persistent Joint Pain and Pain Intensity Reported by Persistent Arthralgia Patients at 5 Years After the Disease Onset
Pain intensity and joint swelling during acute illness related to age reported by persistent arthralgia patients at 5 years after the disease onset was compared and shown in Table 8. Of the 77 patients with persistent arthralgia, 69 cases (89.6%) were <60 years of age. Approximately 2/3 (48 cases/62.3%) of patients with persistent arthralgia had severe pain during acute illness, and most of them (64 cases/83.1%) had nonjoint swelling during acute illness. In addition, joint swelling during acute illness was mostly observed in patients <60 years of age.
Pain Intensity and Joint Swelling During Acute Illness Related to Age Reported by Persistent Arthralgia Patients at 5 Years After the Disease Onset
Calculated from a total of 77 cases.
Discussion
The long-term sequelae of CHIKV infection were systematically reviewed. The most frequently mentioned long-term sequelae of CHIKV infection were persistent arthralgia, arthritis, alopecia (hair loss), and depression (39). In this study, the long-term persistence of joint pain, joint swelling, morning joint stiffness, and/or myalgia were reported in 1.7% of patients enrolled at 60 months after the disease onset. Polyarthralgia was the most prominent symptom. Like those with acute CHIKV infection, most patients with persistent arthralgia had polyarthralgia with symmetrical joint involvement. Their joint symptoms could occur in either a fluctuating or persistent manner, and most reported moderate pain, which was lower than that during the acute phase of CHIKV fever. It primarily affected the small joints of the fingers and wrists, but the affected joints can also be large joints. The self-reported pain sites in this study were almost identical to those reported during the acute phase of the illness. Morning joint stiffness, myalgia, and joint swelling were also commonly observed. Some atypical manifestations included severe depression with suicide attempts, severe weight loss, and severe hair loss were also found in some patients who still experienced severe joint pain.
Recovery rate and musculoskeletal symptoms
In 2018, a systematic review and meta-analysis from a total of 38 studies reported that the proportion of people that do not fully recover after chikungunya was high. The overall nonrecovery rate at the first 3 months following disease onset was 43% (95% CI: 35–52%). After 12 months follow-up, the overall nonrecovery rate was 21% (95% CI: 19–22%). In addition, the prevalence of CHIKV-associated chronic symptoms varied by virus lineage, the highest prevalence in the ECSA-diverged genotype, followed by the Asian lineage genotype (28). The percentage of affected people and the disease activity gradually decrease until the complete resolution of symptoms occurs. The musculoskeletal symptoms may persist for up to 3 years after the onset of disease (35). Up to 80% of CHIKV-infected patients have persistent musculoskeletal manifestations for longer than 1–3 months after the acute fever (1,10). Approximately 60% of Chikungunya-infected patients suffer from musculoskeletal manifestations until 12–36 months after the onset of the acute infection (10,18,21,25,35,37). A study reported that 51.7% of patients had mild pain and 48.3% had moderate-severe pain 15 months after the acute illness (21). In the epidemic in India in 2006, Chopra et al. (6) showed that 4.1% and 1.6% of the patient population suffered from persistent rheumatic pain 1 and 2 years after acute infection, respectively.
Their symptoms included arthralgia, myalgia, and weakness (10,18,21,25,35,37). Long-term arthralgia is typically symmetrical (35) and characterized by polyarthralgia (1,10,25,35), and most patients report episodic relapse and recovery periods (35). In addition to arthralgia, 2–3 years after infection, patients often experienced morning joint stiffness lasting more than 30 min, local joint swelling, weakness, hair loss, or depression (4,5,18,35,39). Other studies have demonstrated moderate disease activity in patients 20 months after the initial CHIKV infection (5).
Related factors
The factors associated with persistent CHIKV-related joint symptoms are not well known. In this study, we found no differences in gender or underlying chronic disease among the groups. According to the self-reported anatomic pain sites and ages, the fingers, wrists, knees, and ankles were most frequently involved in the chronic stage, which is consistent with previous reports (1,4,5,18,21,35). The mean age was <60 years (4,10,21,24). The disease is often more severe in patients who have severe joint pain during acute illness. We propose the existence of a relationship between disease severity during the initial phase of the infection and the persistence of joint symptoms and/or nonrecovery. Our conclusion is consistent with those of previous studies (35,37,39,41).
Considering the underlying chronic diseases, in this study, there were no significant differences in the known incidence of underlying chronic diseases among the persistent arthralgia and full recovery groups. Thus, in our population, comorbidities might not be a risk of persistent arthralgia or severe outcome. In contrast to this study, earlier studies reported an increased risk of persistent arthralgia, when having comorbidities such as diabetes (25,35,37).
Atypical manifestations
In this study, we also reported some atypical manifestations of chikungunya infection, including two cases (2.6%) of severe depression with suicide attempts, two cases (2.6%) of severe weight loss, and four cases (5.2%) of severe hair loss. Remarkably, all the affected patients had severe joint pain. The long-term involvement of these atypical manifestations in patients with suspected CHIKV has been previously reported (2,25,35,38,41), and the association between these atypical manifestations and disease severity has also been mentioned (35,38,41). Soumahoro et al. (38) reported hair loss and depression in CHIKV-infected patients at 17 months after the acute phase, and they also reported more frequent of arthralgia, myalgia, fatigue, depression, and hair loss in patients who were CHIKV positive compared with patients who were CHIKV negative. Schilte et al. (35) reported a higher frequency of depression in patients with arthralgia compared with patients without arthralgia 36 months after the initial infection (50% [31/62 cases] versus 6% [2/33 cases], respectively [p < 0.001]). Moreover, Yaseen et al. (41) reported a higher risk of depression after CHIKV infection in a group suffering from arthritis compared with a group suffering from arthralgia (48.7% [19/39 cases] versus 33.3% [11/33 cases], respectively, p = 0.005). Overall, it appears that these atypical manifestations are related to severe disease.
CHIKV-specific antibodies
For the diagnosis of CHIKV infection, the detection of CHIKV RNA is more sensitive than antibody detection in early CHIKV infection. CHIKV RNA detection is the primary laboratory method used to diagnose CHIKV infection in serum collected <6 days after the onset of illness or during the viremic phase. CHIKV-specific IgM could be detected during the acute phase of infection. The detection of CHIKV-specific IgM antibody is a sensitive test for samples collected ∼>5 days after the onset of illness (14,15,31,34). The presence of IgM antibodies against CHIKV could be detected in all patients after >9 days of fever (34). Several studies have shown that CHIKV-specific IgM antibodies can persist in the sera of infected patients for months (7,16,30,31,34). The persistence of CHIKV-specific IgM in some subjects 1 year after the acute infection has been observed (3,9,12). In a cohort study among the 2007 outbreak in Italy, 82.7% of the IgM antibody disappeared within 12 months (30). A recent study showed the persistence of CHIKV IgM 2 years after the initial illness in some patients (20). CHIKV-specific IgG is usually measurable in the second week of infection or after the virus has disappeared from the blood and can persist for longer than 12 months (9,25,30). Neutralizing antibodies against CHIKV are generated early during infection. And neutralization activity study in serum samples collected from patients during the 2008–2009 CHIKV outbreak in Thailand revealed that all samples had neutralizing activity (17). In this study, we reported the presence of anti-CHIKV IgG at 5 years after acute CHIKV infection in a large percentage (86.5%) of the study population.
CHIKV infection seems to elicit long-lasting protective immunity (27,29). The issues resulting from a possible prolonged persistence of protective immunity or community immunity have also been discussed elsewhere (11,27). The long-term persistence of CHIKV-specific neutralizing antibodies was observed in the population of northeastern Thailand 19 years after a CHIKV outbreak in 1991 (27). Supported by epidemiological data and the history of Cambodia, Galatas et al. (11) proposed that the decreased risk of CHIKV infection in people older than 40 years in the Cambodian rural community was likely because of the fact that these people acquired protective immunity from CHIKV infection during the 1960s and 1970s. In addition, report by epidemic data from the ministry of public health, Thailand, no new CHIKV-suspected/confirmed cases or reinfected cases were reported in the study communities since 2009, whereas some new CHIKV-suspected or confirmed cases were reported in some provinces surrounding the study areas during small outbreak of CHIKV in 2018 (23). Overall, it is likely that these communities acquired immunity from the outbreak in 2008–2009.
Limitations
Our study had several limitations. First, this study relied on self-reported symptoms, and recall bias could have occurred (in particular, on pain score or pain intensity they had during acute illness). Second, the diagnosis during the acute illness of all patients included in the present study was primarily based on epidemic data and clinic symptoms during the outbreak. The presence of anti-CHIKV-specific IgG antibodies in these patients has been tested during population screening and clinical data collection period of this study (between April 2013 and September 2014 or ∼5 years later). In addition, this study has not included the kinetic parameters regarding IgG antibody titer or neutralizing potential of the antibody.
Conclusion
Infection by CHIKV, the ECSA strains, in the southern Thailand population during the outbreak in 2008–2009 resulted in persistent CHIKV-associated symptoms, including polyarthralgia, morning joint stiffness, joint swelling, muscle pain, and some serious unusual clinical manifestations, until 60 months after the acute phase (nonrecovery rate of 1.7%). Also, most (86.5%) of the affected patients still had detectable levels of anti-CHIKV IgG antibodies 5 years after acute CHIKV infection.
Footnotes
Acknowledgments
The authors thank Ms. Jiramit Muenwai (an advanced practice nurse of Paphayom Hospital, Paphayom, Phatthalung, Thailand), for target population screening assistance in Phatthalung Province.
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
This work was supported by the Thailand Research Fund (grant No. MRG5580070); Walailak University (grant No. WU54302); and the new strategic research (P2P) project, Walailak University, Thailand.