
Abstract
Due to the worldwide impact of SARS-CoV-2, people have carried out in-depth research on the virus to fight against this highly contagious disease. In this article, many articles published recently are summarized vertically, from the structure and sites of SARS-Cov-2, the mode of transmission, the mathematical model of transmission, the mechanism of the virus itself, the symptoms of patients after infection to medicine used in the early stage period and the prediction as well the analysis of probability in using new medicine.
Background
In January 2020,
Structure and Sites of SARS-CoV-2
SARS-CoV-2 is a new coronavirus. It is a single-stranded positive-sense RNA-enveloped β–coronavirus (13). Similar to SARS and MERS, its genome encodes nonstructural proteins, structural proteins, and helper proteins. Among them the structural proteins include the spike glycoprotein, which is an indispensable part of virus invasion of cells. The S protein can be divided into two functional domains: S1 and S2 (28). Scientists speculate that cell entry requires the activation of the S protein by a cellular protease and requires the cleavage of S protein at S1/S2 and S2’ sites, allowing the fusion of the virus membrane and cell membrane (24,51). This process is driven by the S2 subunit of the S protein. The S protein uses ACE2 as its entry receptor and is activated by TMPRSS2 (7).
Most of the articles have pointed out that the receptor-binding domain receptor-binding domain (RBD) site of SARS-CoV-2 is the human ACE2 receptor protein. The ACE2 receptor is a carboxypeptidase that can degrade angiotensin II into angiotensin 1–7 (55). In experiments, the ACE2 protein, which was observed on HeLa cells from human, Chinese horseshoe bats, civets, pigs, and mice, was used to study the infectivity of the virus, and it was proven that SARS-CoV-2 could use ACE2-expressing cells as sites of entry, but all cells except those expressing mouse ACE2 could not be entered without ACE2 expression (29). Only four of the five key amino acids binding to the ACE2 protein in the new coronavirus S protein have changed during infection, and the original structure of the interaction between the SARS virus S protein and ACE2 protein is still maintained (6).
The Pattern of the Transmission
Wuhan Jinyintan Hospital published in the Lancet that most of the early patients have a long-term or short-term history of contact with the seafood market in South China. In the first 99 patients, 47 had long-term contact and 2 had short-term contact. In one article, the Institute of Social and Preventive Medicine of the University of Berne proposed that there may be animal-to-human transmission of SARS-CoV-2, and human-to-human transmission (8,39).
It was also believed that the patients may be infected by zoonotic or environmental contact, and transmission between people has already occurred. According to the seventh edition, the mode of transmission is through droplets and respiratory tract aerosols, but digestive transmission needs further study (11). In March 2020, Chen Hualan and others found that cats can be infected with the novel coronavirus and that dogs are not easily infected. It is not clear whether cats can transmit to people. In addition, SARS-CoV-2 expression may be a potential risk factor for vertical transmission of the novel coronavirus (SARS-CoV-2), according to researchers from the China Academy of Medical Sciences.
Transmission and Control for that Population in China
Overall prevention tactics in China can be divided into 5 stages in 6 months (11). The first stage is the time before January 10, 2020, when no specific interventions were imposed. The second period was from January 10 to 22, 2020, when massive population movement occurred because of the Spring Festival and was expected to accelerate the spread of SARS-CoV-2 (33). During this period, the number of patients in the hospital increased, and the hospitals started to be overcrowded. The third period was from January 23 to February 1, when the local government first limited transportation in the city. Other social distancing measures were also implemented, including compulsory mask wearing in public places and limitation of gatherings (17).
Due to previous unknown phenomena and severe shortage conditions in this period, the total number of confirmations dramatically changed from 5,091 to 13,880. On February 2, with improvement in medical resources, the government implemented a policy of centralized quarantine and set up new hospitals for the treatment of all severe confirmed cases. On February 17, the government started door-to-door screening for all residents in Wuhan with support from thousands of community workers (22,43). At the same time, doctors from all over the country came to Wuhan for support. The effective reproduction number, R0, changed in phase one. After that, there was a consecutive increase in the second period, with a peak of 3.82 on January 24, which declined thereafter. The R0 fell below 1.0 on February 6, 2020, and further decreased to below 0.3 on March 1, 2020. In Wuhan, although at first medical supplies, effective drugs, and vaccines were lacking, the implementation of certain policies could effectively control the situation. The government exerted martial law in the third period, and the overall trend of SARS-CoV-2 is shown in Figure 1 (18,40,41).

The effect of martial law on SEIR model.
The Ability of the Infection
The above transmission pattern has a close relationship with ACE2.Some studies indicate that SARS-CoV has a strong affinity for the ACE2 receptor compared with that of SARS-CoV-2. Due to the change in amino acids in the RBD, some hydrogen bonds have been lost. The binding strength of the new coronavirus to its receptor is lower than that of SARS-CoV, indicating that its infection ability is weaker compared with SARS-CoV and that its binding domain structure is more easily disrupted (4,62). However, whether the insertions in the N-terminal domain of SARS- CoV-2 confer sialic acid-binding activity similar to that of MERS-CoV needs to be further studied.
An article preliminarily evaluated the transmission dynamics and epidemiological characteristics of novel coronavirus pneumonia (67). It was confirmed by the observed transmission mode to prove that the similarity between the current situation and the early spread of SARS-CoV in Beijing is not relevant to MERS-CoV in the Middle East, and the transmission mode of SARS-CoV-2 is also similar to that of 1,918 pandemic influenza (23).
A recent article showed that the median age of the cases was 44 years old. With the progress of the epidemic, the proportion of minors and elderly individuals 65 years of age and above has increased. Although ∼20% of China's total population are minors, only 5% of confirmed cases are minors (57,66). The above results do not show that minors have a lower risk of susceptibility or fewer clinical manifestations after infection. As the outbreak occurred in the winter holiday of 2020 and the Chinese Lunar New Year, Chinese schools are closed. The reduction in school-age children's exposure may be related to the lower risk of infection, but further research is needed (31).
Mathematical Model of the Coronavirus
The Center for Health Information, Computation, and Statistics, Lancaster Medical School, University of Lancaster, UK, published an article on January 27, 2020, using the SEIR model to fit the deterministic SEIR infection population transmission model within and between major cities in China with the number of days of 2019 cases of confirmed SARS-CoV-2 cases in Chinese cities and reported cases in other countries (34). The fitting method is as follows: the initial condition is n = 1,000, I = 1, r = 20, the probability of infection is β = 0.03, and R 2 = 20, After contact, the probability of infection is β 2 = 0.03, the probability of conversion from latent person to infected person is α = 0.1, and the probability of rehabilitation is γ = 0.1. The chart is shown in Figure 2.

The SEIR model of SARS-CoV-2.
According to an article published by Guangdong Provincial Center for Disease Control and Prevention (CDC), the average incubation period of SARS-CoV-2 infection is 4.8 days as of January 23, 2020. In 2019, the R values of SARS-CoV-2 were 2.90 (95% confidence interval [CI]: 2.32–3.63) and 2.92 (95% CI: 2.28–3.67), whereas those of SARS and SARS-CoV-2 were 1.77 (95% CI: 1.37–2.27) and 1.85 (95% CI: 1.32–2.49), respectively. It is concluded that the time and R value of SARS-CoV-2 and SARS-CoV from onset to separation in 2019 are all in a downward trend. Therefore, it can be concluded that the risk of SARS-CoV-2 is higher than that of SARS in 2003 (37).
Mohammed A. A. Al-qaness published an article in March utilizing the adaptive neuro-fuzzy inference system (ANFIS), flower pollination algorithm (FPA), and salp swarm algorithm (SSA) to predict the case number for COVID-19. FPASSA-ANFIS used the advanced FPA to train the ANFIS model by optimizing its parameters (26). FPASSA-ANFIS first formatted the input data in the form of a time series. In addition, the training data contained 75% of the data set, whereas the test data contained 25% of the data set. The fuzzy C-means method is used to define the number of clusters and construct the ANFIS model. On the other hand, the updating phase of the followers' positions in the SSA is applied to improve the global pollination phase in the FPA.
The maximum data of iterations are passed to train the parameters of the ANFIS model. When the training phase is finished, the testing phase is initiated with the best solution to compute the final output. Comparing the real data with the predicted data using the performance measures is the way to evaluate the effectiveness. Finally, the FPASSA produces a forecasted value for confirmed cases of COVID-19 in China the next day. The whole procedure is as follows: (25,38) (Fig. 3)
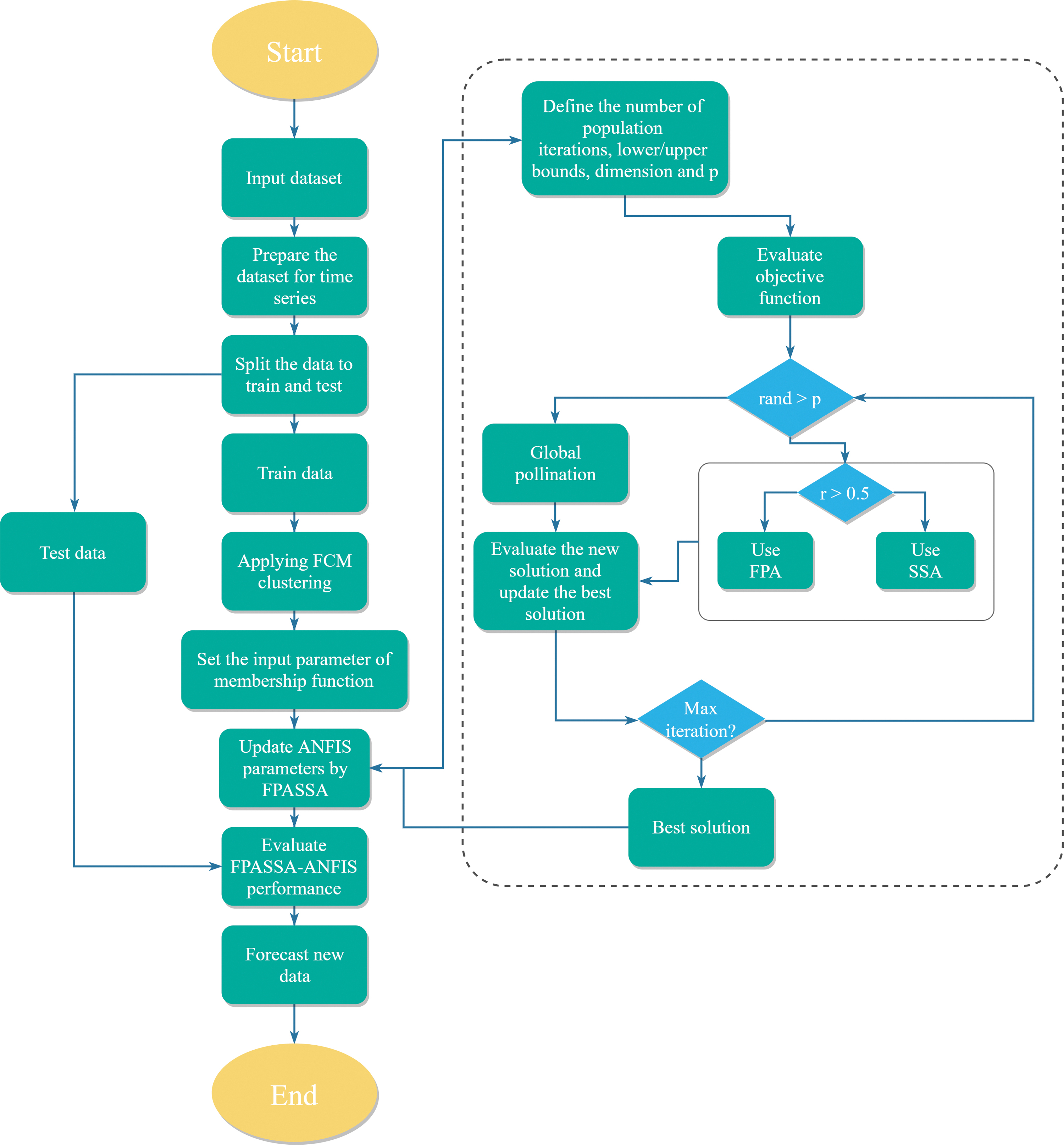
The flow chart of whole prediction process.
To evaluate the infectivity of a virus, a parameter called basic reproduction number (R0) should be introduced, which means how many people a patient will infect with the disease under natural transmission. In the case of no control, if isolated patients can effectively reduce R0, the R0 of SARS was 2–5. On January 28, Li et al. estimated R0 to be ∼2.2, which means that on average each patient was spreading infection to another 2.2 people. Generally speaking, as long as R0 is greater than 1, the epidemic will increase, and the purpose of control measures is to reduce the number of reproduction events to less than 1.
Recently, the University of Hong Kong (HKU) estimated that the new coronavirus R0 was 2.68, whereas the CDC estimated that the R0 was 2.2. At the same time, according to Wuhan, Chongqing, Beijing, Shanghai, Guangzhou, Shenzhen, and other cities, the epidemic situation in the future was predicted, and the epidemic situation will reach its peak around April.
Koch's Postulate
Traditional causative microbes as the agents of disease need to fulfill Koch's postulates. Koch's postulates are a hypothesis described in 1890 by the German physician and bacteriologist Robert Koch, who set out his celebrated criteria for judging whether a given bacteria is the cause of a given disease. Koch's postulates are as follows. The bacteria must be present in every case of the disease. In addition, the bacteria must be isolated from the host with the disease and grown in pure culture. Moreover, the specific disease must be reproduced when a pure culture of the bacteria is inoculated into a healthy susceptible host. Additionally, the bacteria must be recoverable from the experimentally infected host (16).
As of February of 2020, the SARS-CoV-2 has been isolated from patients, detected by specific techniques in patients, and cultured in host cells, starting to fulfill these standards (19).
Traditionally, the identification of microorganisms as pathogenic factors needs to meet Koch's postulates (44). However, at first, it is very difficult to establish a small animal model of coronavirus disease. Although SARS-CoV-2 easily infects laboratory mice, it will not cause major diseases unless it adapts to the mouse host through passaging. Therefore, before February of 2020, the research conducted by new coronavirus investigation and research teams in China did not conform to Koch's hypothesis.
In new studies, using currently isolated SARS-CoV-2 to infect transgenic mice, interstitial pneumonia could appear, which is similar to the preliminary clinical report of SARS-CoV-2 pneumonia. At the same time, virus replication can be detected in ace2-hb-01 mouse lung tissue. Therefore, as of April of 2020 the pathogenicity of SARS-CoV-2 in hACE2 mice was clarified, and Koch's postulates were fulfilled (57).
Clinical Feature of the Infected Patients in China
SARS-CoV-2 was confirmed by real-time reverse transcription-polymerase chain reaction (63). In the New England Journal of Medicine (NEJM), a research team led by the academician Zhong Nanshan reported the data of 1,099 COVID-19 patients diagnosed by the laboratory in 552 hospitals in China as of January 29, 2020 (53). The main composite end point was admission to the intensive care unit (ICU), use of mechanical ventilation, or death (21). The most common symptoms were fever (43.8% before admission, 88.7% at admission), cough (67.8%), and, rarely, diarrhea (3.8%). At the time of admission, ground glass opacities were the most common radiologic manifestation on computed tomography (CT) (56.4%). A total of 157 of 877 (17.9%) noncritical patients had no imaging or CT abnormalities, and 5 of 173 (2.9%) critical patients had no abnormalities.
Lymphocytopenia was present in 83.2% of patients at admission. Additionally, with the release of the seventh edition of the novel coronavirus pneumonia diagnosis and treatment program in China, we have obtained conclusions based on the current epidemiological survey (10). The incubation period is generally 3–7 days, the longest is not more than 14 days, and the incubation period is still infectious (58). According to the novel coronavirus pneumonia prevention and control program (Sixth Edition) issued by China, asymptomatic infections refer to no relevant clinical symptoms (such as fever, cough, sore throat, etc.), but nucleic acid tests or antibody tests are positive for respiratory tract specimens (60). Asymptomatic infections are not confirmed cases, so they are not new infections. Asymptomatic infection can also be a source of infection, with a certain risk of transmission (50,51).
Pathogenesis
As far as we know, both the novel coronavirus and SARS-CoV enter human cells through the ACE2 receptor on the surface of human cells, so in principle, tissue expressing ACE2 will be invaded by the novel coronavirus, and the tissue not expressing ACE2 will not be invaded by the novel coronavirus. In addition, ACE2 is expressed in different organs and tissues, especially in the lung and intestine (30,51). Specifically, the expression level of the ACE2 protein in alveolar epithelial cells and small intestinal epithelial cells is very high, so the novel coronavirus causes a disease of the lower respiratory tract, and some patients have diarrhea symptoms. In addition, ACE2 is also distributed on the aqueous humor, meaning it can transmit through eyes, leading to infection (59).
According to the autopsy results reported in the literature in 2009, 35% of the patients who died of SARS had SARS-CoV present in their hearts. It is suggested that SARS-CoV invades the heart and causes immune cells to appear in the heart muscle with inflammation. After SARS-CoV invaded the heart, ACE2 protein expression is decreased significantly. However, the significant downregulation of ACE2 in heart tissue can fully cause heart injury (64,65). Therefore, we also speculate that the mechanism of cardiopulmonary injury caused by the novel coronavirus is the same as that caused by SARS-CoV. The virus downregulates the expression of ACE2 and causes cardiopulmonary injury (9).
Medicine for Use Against SARS-CoV-2
Antiviral drugs
Oseltamivir
According to an article published by Wuhan Jinyintan Hospital in the Lancet, oseltamivir, an inhibitor of influenza virus neuraminidase, was used in combination with antibiotics to treat patients (42). Wuhan Union Medical College Hospital also proposed the use of oseltamivir, an influenza drug, to treat the novel coronavirus. From a medical point of view, there is great controversy about whether oseltamivir can be used to cure various diseases derived from SARS-CoV-2. This highly controversial treatment plan and results have been published in the international top medical journal The Lancet.
Oseltamivir, a neuraminidase inhibitor on the surface of influenza virus, can be used to treat virus infection. Many international laboratories have not found that oseltamivir can inhibit coronavirus when using a high-throughput drug screening platform to screen for anti-coronavirus drugs. For example, Emily. L.C. and others have published articles on SARS, indicating that oseltamivir, an anti-influenza drug, is ineffective. Oseltamivir, which targets the fusion of viruses and human cells, inhibits mainly neuraminidase on the surface of influenza virus. However, the mechanism of the novel coronavirus and SARS-CoV invading human cells is that the coronavirus spike protein recognizes the ACE2 receptor on the surface of human cells, which has nothing to do with neuraminidase.
Lopinavir/ritonavir
Some experiments show that lopinavir/ritonavir can produce effects on SARS-CoV and MERS-CoV, so it is speculated that lopinavir/ritonavir can also effectively treat SARS-COV-2 (1). As SARS coronavirus produces two polysomal proteins after translation, and the two polysomal proteins pl2 and 3CL have protease activity, pl2 will cut 3 sites in the polysomal protein, and 3CL will cut 11 sites in the polysomal protein to obtain all the functional proteins needed for SARS-CoV assembly and biological function. The medicines that have anti-AIDS activity are two protease inhibitors, lopinavir and ritonavir, which inhibit the multibody protein cleavage after RNA translation of the novel coronavirus. Because it is unable to produce all the functional proteins required for virus assembly and biological functions, the replication of coronavirus in human cells is inhibited. Three patients with mild novel coronavirus disease were cured in Shanghai and were discharged in 1 week (49).
Remdesivir
It is acknowledged that MERS-CoV, SARS-CoV, and SARS-CoV-2 are all coronaviruses, so we can to some degree predict new treatments based on the previous therapeutic schedules. It has been published in the literature that for MERS-CoV, remdesivir, lopinavir, and interferon have been used, and good effect has been achieved with the RNA polymerase inhibitor in a MERS-CoV animal model (69). The effect of treatment for the novel coronavirus has also been evaluated, and there are no instructions to use oseltamivir in treatment. The State Key Laboratory of Virology, Center for Biosafety, Wuhan Institute of Virology, Chinese Academy of Sciences, introduced that remdesivir can effectively inhibit SARS-CoV-2 infection in vitro.
The experimental results showed that remdesivir had a significant inhibitory effect on the infection of the SARS-CoV-2-sensitive human hepatoma cell line Huh-7. As far as we know, remdesivir is a recent antiviral drug that can be used to inhibit the infection of RNA viruses in cultured cells, including that by SARS/MERS-CoV (57). At present, it is used for the treatment of Ebola virus infection (54). As an adenosine analog, it binds to a new viral RNA chain, leading to early termination. Other experiments show that the antiviral mechanism of this kind of drug is consistent with that of nucleotide analogs. A cytology experiment proved that remdesivir was better than lopinavir. Animal experiments showed that remdesivir could significantly inhibit the replication of MERS-CoV and lung injury (59). In addition, new research results show that lopinavir cannot block the acute lung injury caused by MERS-CoV, whereas remdesivir, a broad-spectrum coronavirus inhibitor, can. According to the latest Lancet data published from China, the mortality rate of severe patients in the ICU with novel coronavirus pneumonia is close to one-third (55).
Therefore, for severe patients with novel coronavirus infection who have had acute lung injury, we speculate that the clinical effect of remdesivir is higher than that of lopinavir. On April 10, 2020, Jonathan Grein presented his research article in the NEJM, which analyzed the data of 53 severe patients. During the median follow-up period of 18 days, 36 patients (68%) had improved oxygen support levels, of which 30 patients (57%) received mechanical ventilation and 17 patients had been extubated. Clinical improvement was observed in 36 of 53 patients (68%) who were treated with remdesivir (51).
However, based on the emergence of children with novel coronavirus pneumonia in various provinces and cities, it is necessary for the clinical guidelines to address for the use of drugs in infants and children.
Ribavirin
In addition, ribavirin at a safe dose is ineffective against the novel coronavirus, and only high-dose ribavirin can be effective, which has been confirmed for SARS/MERS-CoV (2). Ribavirin at a regular dose is not effective for coronaviruses because SARS-CoV has a nuclease with a self-correction function. If ribavirin, a nucleotide analog integrated into RNA, is found, it will be repaired. When the dose is increased, the self-correction function is inhibited, and then the RNA virus produced is defective, which is the reason why ribavirin is effective in treating SARS.
Mycopenelate mofetil
It was proposed that the activity of mycopenelate mofetil was the best to inhibit MERS-CoV. Moreover, the blood concentration of the conventional dose of microphenolic acid is more than 60 times the effective inhibitory concentration in vitro, compared with the blood concentration of interferon being more than 3 times the effective inhibitory concentration in vitro (3). The reason for the failure of many antiviral drugs in the treatment of coronaviruses is that the blood concentration cannot reach the effective inhibitory concentration in vitro, but microphenolic acid does not have this problem. The mortality rate of coronavirus-induced MERS was 35–40%. In a clinical retrospective analysis, eight patients who received mycophenolate mofetil were all alive. Therefore, it is speculated that these drugs can inhibit SARS-CoV-2.
Chloroquine
Chloroquine, proposed by Wuhan virologists, has been widely used in the population as a drug against malaria and autoimmune diseases, but it has recently been reported that chloroquine is a potential broad-spectrum antiviral drug that can enhance its antiviral effect in vivo (69). It is well known that chloroquine can prevent virus infection and interfere with glycosylation of the SARS-CoV cell receptor by increasing the pH value of virus/cell fusion. Experiments show that chloroquine plays a role in the entry and postentry stages of SARS-CoV-2 infection in Vero E6 cells. As a drug that has been used for more than 70 years, it is expected to have a potential clinical application value in the treatment of the virus (48).
Imatinib
Imatinib, the leukemia ABL kinase inhibitor drug, can be used as one of the drugs during experimental phases for the treatment of severe patients with novel coronavirus pneumonia in Wuhan (45). In 2014, the National Institutes of Health's Institute of Allergy and Infectious Diseases published an article on drug screening. It was found that imatinib's EC50 to inhibit SARS was lower than 10 μm. Three ABL kinase inhibitors, imatinib, dasatinib, and nilotinib, were screened to inhibit SARS-CoV. When coronavirus enters human cells, it needs to fuse the outer membrane of the virus and human cell membrane. This fusion is mediated by the combination of the S protein of coronavirus and the receptor on human cells, while ABL kinase inhibitors can inhibit membrane fusion so that the virus cannot enter human cells.
As the virus enters the cell and fuses with the endosome membrane, imatinib, an ABL kinase inhibitor, also inhibits this process, thus inhibiting the replication of the virus in the cell. Moreover, imatinib can reverse the mechanism of pulmonary immune injury, which is of great significance for severe patients. Imatinib is a multikinase-targeting drug, and the inhibition of several kinases is the main mediating factor of alveolar cell boundary damage. Animal models have shown that imatinib can effectively alleviate acute lung injury caused by pulmonary inflammation and vascular leakage. Imatinib is not only an antiviral drug but also a drug that can repair acute lung injury, so it is important to test this drug for the treatment of severe patients with novel coronavirus pneumonia (32).
Interferon
Interferon beta (IFN β) 1a has been proven to be effective in the treatment of SARS (15). The receptor of coronavirus is ACE2. When coronavirus invades alveolar cells, it will downregulate the expression of ACE2 to destroy the boundary of alveolar cells. In an animal model experiment, the use of recombinant ACE2 protein effectively reduced the lung damage caused by SARS-CoV and compensated for the downregulation of ACE2 caused by SARS-CoV. Therefore, IFN β 1a, which has been proven to be effective in the treatment of SARS, can protect the boundary of alveolar cells (61).
Anti-inflammatory drugs
Interleukin
Patient progress can be divided into three periods (early, middle, and late). In the early stage, the patients have detectable viral nucleic acids, and the lungs showed symptoms, but there is no irreversible lung injury; at this stage, lopinavir can work. In the middle stage, the lung begins to exhibit irreversible damage, but it is not very serious and requires remdesivir and even immunotherapy (69). However, in the late stage, it is necessary to use remdesivir combined with immunotherapy. For novel coronavirus pneumonia immunotherapy drugs, we need to consider the treatment of interleukin (IL)-6/IL-6 receptor monoclonal antibodies, which is the treatment plan for CAR-T therapy for cancer patients and is also one of the standard treatment plans for immunopneumonia caused by anti-PD1/anti-CTLA-4 antibody immunotherapy (14).
Glucocorticoids
The Lancet published a critical article from Clark D Russell and three other people from the infection research center of the University of Edinburgh in the United Kingdom, arguing that the clinical evidence does not currently support the hormone treatment of lung injury caused by the SARS-CoV-2 for the time being. In the interim, guidelines for the treatment of severe acute respiratory infection suspected to be caused by SARS-CoV-2 were issued on January 28, 2020, which does not recommend the use of glucocorticoids, unless there are other indications for the use of hormones. However, according to the degree of dyspnea and the progress of chest imaging, glucocorticoids can be used in a short time period (3–5 days) according to the seventh edition of treatment guidelines issued in China (11,47).
Other drugs
Losartan
In 2005, HKU published a review article in Nature Medicine on the positive and negative effects of ACE on lung injury caused by SARS-CoV. SARS-CoV downregulated ACE2, increased angiotensin II expression, activated the AT1R receptor, and caused pulmonary edema and injury. However, the use of recombinant ACE2 protein in the lung can reduce the lung injury induced by SARS-CoV. Alternatively, an AT1R inhibitor, losartan can alleviate the acute lung injury caused by the downregulation of the ACE2 protein by the spike protein of coronavirus (58). However, as a basic drug that is not used clinically, we need to consider whether the drug will affect the lung injury of patients through ace-ang ii-at1r.
The AT1R inhibitor can be used as a choice for the clinical treatment of virus-induced lung injury of patients. In addition, patients with hypertension who use ACE2 inhibitors will have a very high mortality rate after being infected with coronavirus, because ACE2 inhibitors will accelerate the destructive effect of coronavirus on the lung, resulting in rapid deterioration of patients' condition (36). Therefore, when choosing this kind of medicine, we should consider hypertension patients (35).
Lianhuaqingwen
As a traditional Chinese medicine, Lianhuaqingwen has broad-spectrum antiviral and immunomodulatory effects on a series of influenza viruses. At the mRNA level, it significantly inhibited the replication of sars-cov-2 in Vero E6 cells, and significantly reduced the production of proinflammatory cytokines (TNF-α, IL-6, CCL-2/MCP-1, and cxcl-10/IP-10). In addition, when taking this kind of medicine, the particle morphology of virus particles in cells was abnormal (46).
Summary
We initially suspected that the virus came from the wild game outbreak in the South China seafood market of Wuhan. However, a description of the first clinical cases published in The Lancet challenges that hypothesis, and it is suspected that SARS-Cov-2 is not from the South China seafood market. At present, we know that SARS-CoV-2 has 96% similarity with bat coronavirus and 79.5% similarity with SARS-CoV. However, the “intermediate host” from bats to humans remains unclear.
By April 19, 2020, the number of confirmed cases has reached over 2 million worldwide, and most patients that died had basic diseases (27). New vaccines and new clinical use of drugs have been developed through dedicated research institutes of various centers across the country (5). As this article mentioned, SARS-CoV-2 share some common features with SARS-CoV and MERS-CoV. Since some medicines can have some effects on SARS and MERS, we predict that there is a high possibility to find the medicines that also have effects on COVID-19 (48,52).But when we use the drug, it is better to consider about other diseases, such as diabetes (12).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.