
Abstract
The aim of this study was to analyze the correlation between dynamic changes in the nasopharyngeal viral load of patients infected with the new coronavirus causing pneumonia and lymphocyte count disease severity. Cases newly diagnosed with COVID-19 at the First Affiliated Hospital of Nanchang University from January 2020 to February 2020 were analyzed retrospectively. Quantitative real-time polymerase chain reaction was used to determine severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from throat swab sample ΔCT values; lymphocyte and lymphocyte subset counts, coagulation system factor levels, myocardial injury indexes, and laboratory biochemical indicators were compared between the mild group and the severe group. The correlation between the relative load of nasopharyngeal SARS-CoV-2 RNA and severe disease symptoms was analyzed. Of the 76 patients, 49 were male and 27 were female. The lymphocyte, CD4+ T lymphocyte, and CD8+ T lymphocyte counts all differed significantly between the two groups (p < 0.001), as did differences in interleukin (IL)-2R, IL-6, and IL-8 levels (p = 0.022, 0.026, and 0.012, respectively). Moreover, there were significant differences in prothrombin time, D-dimer, and fibrinogen levels between the mild group and the severe group (p = 0.029, 0.006, and <0.001, respectively), and in lactate dehydrogenase and troponin (p < 0.001 and p = 0.007, respectively). SARS-CoV-2 RNA load and lymphocyte count, CD4+ T lymphocyte count, and CD8+ T lymphocyte count were linearly negatively correlated (p < 0.001). SARS-CoV-2 RNA load was positively correlated with IL-2R, prothrombin time, lactate dehydrogenase, and hypersensitive troponin T (p = 0.002, p = 0.009, and p < 0.001, respectively). In addition, the time that it took for the nucleic acid test to turn negative was significantly shorter for patients in the mild group than for those in the severe group (Z = −6.713, p < 0.001). In conclusion, relative SARS-CoV-2 RNA load in the nasopharynx is closely related to COVID-19 severity. If the relative RNA load was higher, the lymphocyte count was lower, organ damage was greater, and the time it took for the nucleic acid test to turn negative was longer.
Introduction
Since December 2019, pneumonia (COVID-19) caused by infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has occurred in Wuhan, Hubei, with huge detrimental effects on the lives and health of individuals (14,16). SARS-CoV-2 is a newly discovered coronavirus that can infect humans. Populations are generally susceptible, the disease is highly contagious, and there is no clear or specific treatment proposal (6,8). As of February 23, 2020, there were 76,396 confirmed cases and 5,365 suspected cases of infection nationwide in China (information from the official website of the National Health and Health Commission;
Materials and Methods
Clinical inclusion criteria
From January 2020 to February 2020, 76 patients with COVID-19, comprising 49 males and 27 females aged 18–78 years (median age = 45 years), were admitted to the First Affiliated Hospital of Nanchang University. Patients were diagnosed according to the new diagnosis and treatment protocol for coronavirus infectious pneumonia (6th trial version) (10), which involved matching clinical manifestations of COVID-19 infectious pneumonia, epidemiological history, and a positive result for SARS-CoV-2 nucleic acid from respiratory or blood specimens by qRT-PCR analysis, or viral gene sequencing results from respiratory or blood samples revealing high homology with the known SARS-CoV-2 virus sequence. Depending on symptom severity, patients were classified into mild or severe COVID-19 groups. The severe COVID-19 group was defined when the following clinical criteria were met: (a) respiratory distress (respiratory rate ≥30 beats/min); (b) resting-state oxygen saturation ≤93%; (c) arterial partial pressure of oxygen/oxygen concentration ≤300 mm Hg; or (d) respiratory failure, mechanical ventilation, shock, or other functional organ failure requiring intensive care unit monitoring and treatment. Of the 76 cases included in this study, 46 were in the mild group and 30 were in the severe group.
Data collected
Demographic data, epidemiological history, clinical manifestations, and laboratory results of patients diagnosed with COVID-19 infection at the First Affiliated Hospital of Nanchang University were collected retrospectively.
Specimen collection
From January 22, 2020, to February 15, 2020, researchers collected throat swab specimens from 76 patients admitted to the First Affiliated Hospital of Nanchang University at least once. Throat swab samples were collected three or more times at different time points after disease onset from half of all the patients. All the samples were tested for SARS-CoV-2 using nucleic acid real-time fluorescence qRT-PCR.
Nucleic acid detection
(a) Disposal and inactivation of throat swab specimens: Throat swab eluates (3 mL) were incubated in a 56°C water bath for 40 min, and then nucleic acid was extracted from the throat swab eluate samples.
(b) Nucleic acid extraction and qRT-PCR: A Daan gene smart32 automatic nucleic acid extraction instrument and auxiliary extraction reagent were used for nucleic acid extraction from 200 μL throat swab eluate per sample. qRT-PCR was conducted using a dual-target gene detection kit (Guangzhou Daan Gene Co. Ltd.), and the difference (ΔCT) between the sample cycle threshold (CT) and the positive quality control CT value was calculated (2,13)..
Statistical methods
GraphPad Prism v8.0 (GraphPad Software) was used for statistical analyses. The Mann–Whitney U-test was used to evaluate non-normally distributed data, which are shown as the median (interquartile range [IQR]). Spearman's rank correlation analysis was used to evaluate relationships with different sample ΔCT values, and Bland–Altman plots were used to analyze CT value consistency. A p-value of <0.05 was considered statistically significant.
Ethics statement
The study was evaluated by the Ethics Committee of the First Affiliated Hospital of Nanchang University. Patients involved in the study were anonymized. No informed consent was acquired because this was a retrospective study.
Results
Epidemiological and clinical characteristics
This study included 76 patients with COVID-19 hospitalized at the First Affiliated Hospital of Nanchang University. Time from onset to admission ranged from 1 to 11 days (median = 4 days). Five cases had a history of smoking, and 26 cases had underlying health conditions, including seven with essential hypertension, seven with chronic liver disease, and three with diabetes.
Of the 76 patients, 63 (82.9%) had a fever, 36 (47.4%) had a cough with sputum, 13 (17.1%) had fatigue and muscle soreness, 12 (15.8%) had chest tightness and dyspnea, and 12 (15.8%) experienced dizziness. There were 10 (13.2%) cases of headache and 4 (5.3%) of vomiting and diarrhea. Further, 66 (86.8%) cases had normal or reduced white blood cell counts, and 43 (56.6%) had decreased lymphocyte counts. There were no significant changes in hemoglobin or platelets in any patient. C-reactive protein (CRP) was elevated in 54 (71.2%) cases, while calcitonin levels were normal in all the patients. Serum lactate dehydrogenase levels were increased in 48 (63.2%) cases, serum high-hypersensitivity troponin T was increased in 14 (18.4%) cases, D-dimer was elevated in 38 (50%) cases, and interleukin (IL-6) was elevated in 37 (48.9%) cases. However, liver function (alanine aminotransferase, aspartate aminotransferase, total bilirubin) and renal function (blood urea nitrogen, serum creatinine) were normal in most (89.5%; 68/76) patients. Among inflammatory factors, IL-2R, IL-6, and IL-8 levels were significantly higher in the severe group than they were in the mild group (Z = −2.288, −2.227, and −2.298, respectively; p = 0.022, 0.026, and 0.012, respectively). In terms of coagulation system factors, prothrombin time, D-dimer, and fibrinogen were significantly higher in the severe group than they were in the mild group (Z = −2.282, −2.754, and −4.382, respectively; p = 0.029, p = 0.006, and p < 0.001, respectively) (Table 1). Further, lymphocyte, CD4+ T lymphocyte, and CD8+ T lymphocyte counts in the severe group were significantly lower than they were in the mild group (Z = −5.889, −4.932, and −5.505, respectively; p < 0.001). In terms of myocardial injury indexes, lactate dehydrogenase and troponin were significantly higher in the severe group than those in the mild group (Z = −4.273 and −2.693, respectively; p < 0.001 and p = 0.007, respectively) (Table 2).
Comparison of Inflammatory Factors and Coagulation System Indexes Between Patients with Mild and Severe COVID-19
Data shown are median (interquartile range).
IL, interleukin; PT, prothrombin time; APTT, activated partial thromboplastin time; Fib, fibrinogen.
Comparison of Lymphocyte Counts and Myocardial Injury Markers Between Patients with Mild and Severe COVID-19
Data shown are median (interquartile range).
CK, creatine kinase; CK-MB, creatine kinase myocardial band; LDH, lactate dehydrogenase;
Correlation between nasopharyngeal virus load and disease severity in patients with COVID-19
Of the 46 cases in the severe group, the median SARS-CoV-2 RNA ΔCT value from nasopharynx samples was −1.25 (IQR −5.21, 1.78), while the corresponding ΔCT value of the 30 cases in the mild group was 4.48 (IQR 2.42, 6.43), and the difference in relative RNA load between the two groups was significant (Z = 5.53, p < 0.001).
As shown in Figure 1, the nasopharyngeal SARS-CoV-2 RNA ΔCT value from the patients with COVID-19 was positively correlated with lymphocyte, CD4+ T lymphocyte, and CD8+ T lymphocyte counts (r = 0.548, 0.478, and 0.525, respectively; p < 0.001). Further, the nasopharyngeal SARS-CoV-2 RNA ΔCT value from the patients with COVID-19 was negatively correlated with IL-2R, lactate dehydrogenase, and high-sensitivity troponin T levels (r = −0.323, −0.339, and −0.537, respectively; p = 0.002, p = 0.004, and p < 0.001, respectively; Fig. 2).
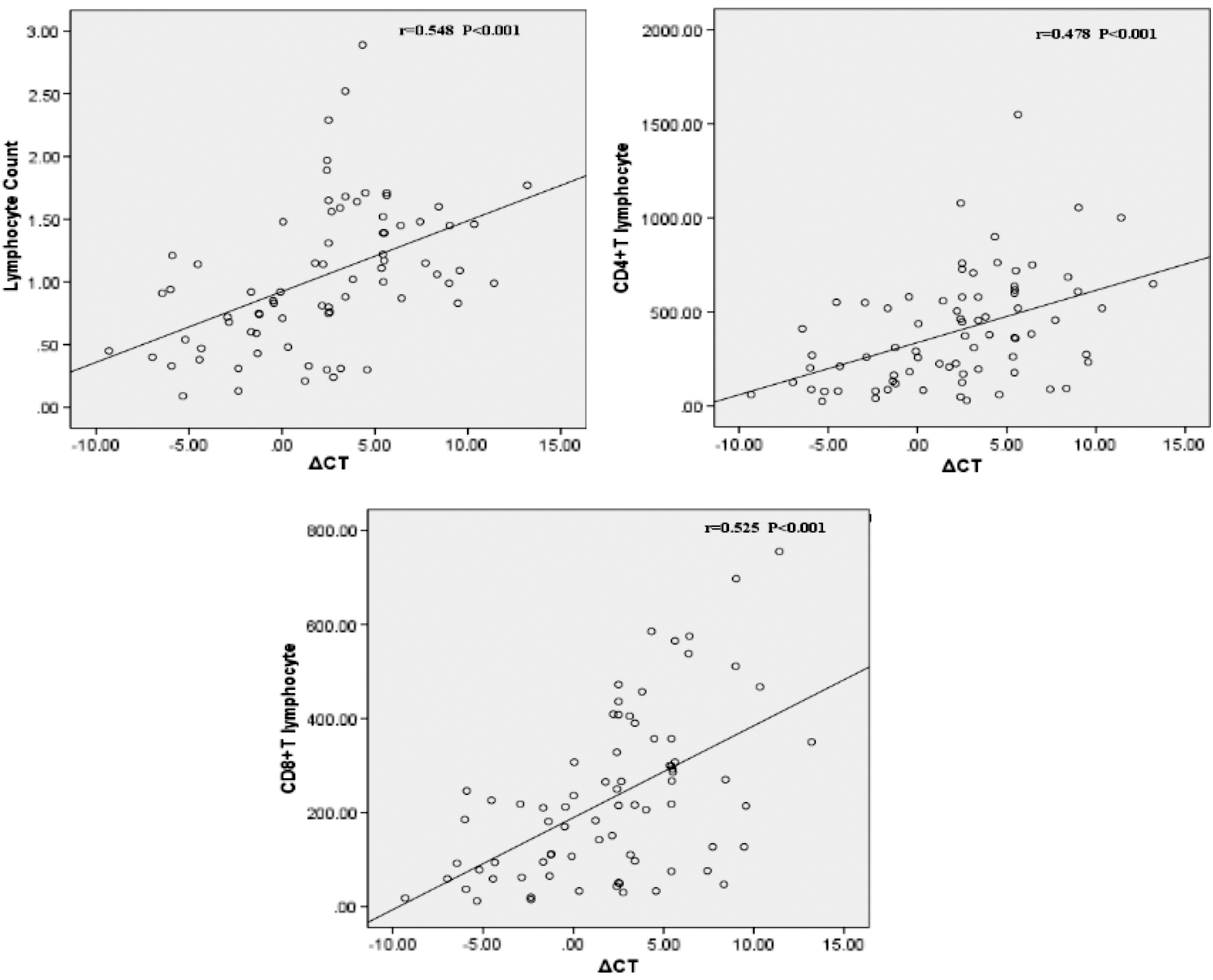
Correlation between the nasopharyngeal severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA ΔCT values from patients with COVID-19 and lymphocyte, CD4+ T lymphocyte, and CD8+ T lymphocyte counts.
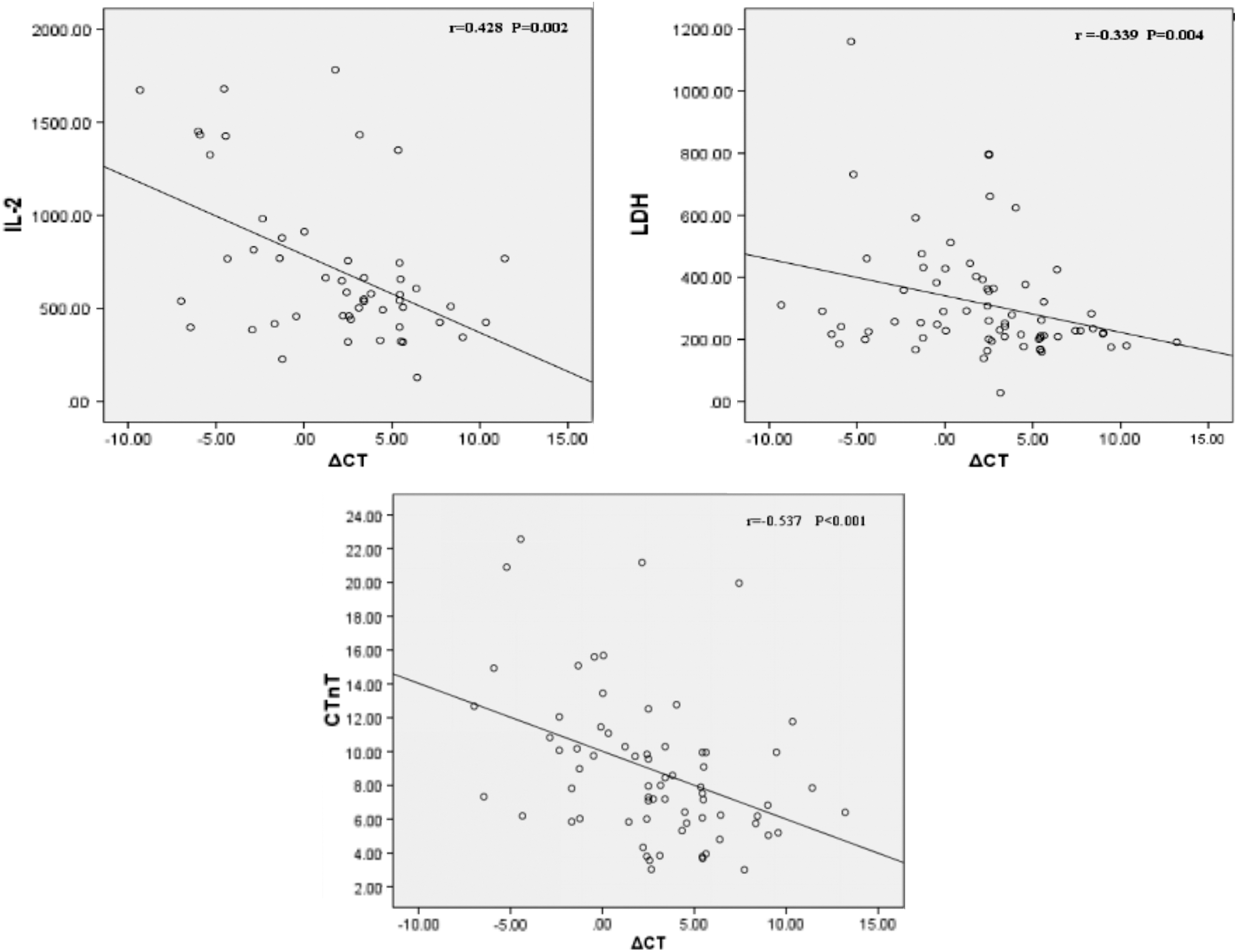
Correlation between the nasopharyngeal SARS-CoV-2 RNA ΔCT values from patients with COVID-19 and interleukin 2R, lactate dehydrogenase, and troponin T levels.
Dynamic monitoring of nasopharyngeal SARS-CoV-2 RNA load in half of all the patients with COVID-19
Three days after onset, the viral load of partial patients began to decline, and 15 days after onset, the test results of all the patients from the mild group were negative. The median time that it took for the nucleic acid test to turn negative was 4 days in patients from the mild group, while it was 10 days in patients from the severe group. The difference was significant (Z = −6.713, p < 0.001).
Discussion
COVID-19 is a novel public health emergency that arose toward the end of 2019. The virus has a wide range of transmission channels, is highly contagious, and poses a serious threat to the life and health of people across China and the wider world (7). Currently, the prevention and control measures for pneumonia caused by COVID-19 are focused on early diagnosis, early isolation, and early treatment. The diagnosis of patients with COVID-19 requires laboratory testing for SARS-CoV-2 RNA. After effective symptomatic treatment, most infected individuals achieve remission and rehabilitation (15). However, a few patients develop severe or even critical illness. To date, we do not fully understand why most infected people exhibit mild symptoms or are asymptomatic, while others have severe or critical symptoms. This is because we do not have sufficient information about the amount of time that SARS-CoV-2 RNA can survive in the nasopharynx or the relationship between viral load and factors contributing to disease severity and progression. Here, we found that the detection of nasopharyngeal SARS-CoV-2 RNA and dynamic observation of the SARS-CoV-2 RNA load was highly relevant to monitoring disease changes in COVID-19, which can provide important evidence contributing to the diagnosis and surveillance for the development tendency of COVID-19.
There were more male than female patients in this study. The median time from onset to admission was 4 days, suggesting that most patients were able to seek medical attention promptly. Therefore, most patients had a mild illness, which is consistent with a previous report (1). Clinical manifestations were mainly fever, which was often accompanied by a cough. Other symptoms, such as chest tightness, dyspnea, dizziness, and headache, mainly occurred in patients with severe disease. Laboratory tests showed that most patients had normal or decreased peripheral white blood cell counts, a more pronounced reduction in lymphocyte counts, slightly elevated CRP, and normal procalcitonin levels. More than half of the patients had elevated serum lactate dehydrogenase, and some had elevated troponin, indicating that a proportion of patients had myocardial damage (18). In addition, half of the patients exhibited elevated D-dimer levels.
In this study, the nasopharyngeal SARS-CoV-2 RNA load was significantly higher in the severe group than it was in the mild group. In the severe group, lymphocyte, CD4+ T lymphocyte, and CD8+ T lymphocyte counts were generally significantly reduced and were negatively correlated with SARS-CoV-2 RNA load, which suggested that the reduction of lymphocytes and their subpopulations directly affected by viral load was closely related to disease progress (12). In addition, the patients from the severe group in this study showed increased levels of inflammatory factors (such as IL-2, IL-6, and IL-8), significant increases in coagulation indicators (such as prothrombin time, D-dimer, and fibrinogen), and increases in lactate dehydrogenase and myocardial injury markers (such as troponin), which suggested that the occurrence of severe COVID-19 was closely related to the inflammatory release, coagulation dysfunction, and myocardial injury, consistent with a previous report (9). In addition, we also found that the SARS-CoV-2 RNA load was positively correlated with IL-2R, prothrombin time, lactate dehydrogenase, and high-sensitivity troponin T in patients with COVID-19, which may indicate nasopharyngeal SARS-CoV-2 viral load can directly affect the damage of organ function.
We also observed that from 3 days after onset, viral load in most patients with COVID-19 gradually decreased to none, and in all patients from the mild group, nasopharyngeal samples became negative for the virus by 15 days after onset, while in some patients from the severe group, nasopharyngeal SARS-CoV-2 RNA could be present for more than 15 days. Therefore, we speculate that SARS-CoV-2 RNA may not persist for more than 2 weeks in the nasopharynx of patients from the mild group, while it remained significantly longer in patients from the severe group. The length of time the virus remains in the body is related to the viral load. This suggests that the viral nucleic acid shedding pattern of SARS-CoV-2 is similar to that of influenza, which differs from that of SARS-CoV (9,11). The median time that it took for the nucleic acid test to turn negative in patients with severe disease was significantly longer than it was in patients with mild symptoms, indicating that elimination of SARS-CoV-2 RNA in the nasopharynx may influence the disease severity of patients with COVID-19 (5).
This study has certain limitations. First, we performed a retrospective analysis of only a proportion of COVID-19 patients admitted to our hospital. The First Affiliated Hospital of Nanchang University is the provincial designated treatment hospital in Jiangxi Province, especially for critically ill patients. Consequently, the case selection was limited. Second, since absolute quantification of the SARS-CoV-2 virus is not yet available, we used ΔCT values for relative quantification. Hence, more accurate quantitative data are needed for further in-depth analysis and to avoid data bias. Third, because most patients had mild symptoms such as a dry cough without sputum, bronchoalveolar lavage tests could not be performed widely. We could only conduct nucleic acid tests using nasopharyngeal swab samples to reflect patient SARS-CoV-2 viral load, which may deviate from the actual viral load in the lung to some extent.
In summary, the SARS-CoV-2 RNA test is an important tool for the diagnosis of COVID-19. Higher SARS-CoV-2 nasopharyngeal RNA loads are more common in patients with severe disease. On the one hand, high virus loads may directly damage tissues and cells; on the other hand, a strong immune response to high viral loads in the human body can also seriously damage cells and organs. Moreover, high viral loads directly influence disease progression and the time it takes for the nucleic acid test to turn negative.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Financial support was provided by the National Natural Science Foundation of China (81860368), the National Mega-project for Innovative Drugs (2019ZX09721001), and Anti-Infective Drug Research (2019BJZDS003).