
Abstract
Hand, foot, and mouth disease (HFMD) is a pediatric public health concern in Asia. Surveillance data on the circulating serotypes of HFMD suggest that Enterovirus A71 (EV-A71) and coxsackieviruses A6, A10, and A16 (CVA6, CVA10, and CVA16) are the major serotypes causing HFMD. Asian countries, including Korea, are currently developing a multivalent vaccine targeting these serotypes. However, the immunity of children against specific serotypes, indicating past infection, should also be considered while selecting candidate serotypes for vaccine development. Therefore, we aimed to identify the age-stratified serological statuses of Korean children to determine candidate serotypes for HFMD vaccine development. This study included 220 participants, categorized into four age groups, 7 months–2 years, 3–5 years, 6–10 years, and 11–15 years. A neutralization test was performed to quantitate the neutralizing antibodies (NtAbs) in the sera of the participants. Only EV-A71 and CVA6 were found suitable as candidate serotypes for vaccine development, whereas further study is needed for CVA10 and CVA16. The highest seropositivity and NtAb titer ranges were observed for CVA6 in all age groups, suggesting that the participants had been predominantly exposed to CVA6. For EV-A71, seropositivity and NtAb titer ranges steadily increased with age, suggesting that children were currently exposed to EV-A71. For CVA10, the 3–5 years group showed the highest seropositivity rate and higher NtAb titer ranges than the older age groups, indicating that the exposure to CVA10 had mainly occurred in recent years. Future studies will identify whether the exposure to CVA10 was transient or will continue. For CVA16, seropositivity and NtAb titer ranges were generally low, indicating that only a few participants had been exposed to CVA16. We identified discrepancies between the sentinel surveillance data and our findings. This study provides a new perspective for HFMD vaccine development and policy making in Asian countries.
Introduction
Hand, foot, and mouth disease (HFMD) is a major pediatric infectious disease in Asian countries. It usually occurs in children <5 years old. It is self-limiting in most cases; however, complications such as encephalitis, acute flaccid paralysis, or pulmonary edema may result in fatality. HFMD is a very contagious and high-incidence disease that affects millions of children across Asia annually (4,18). The outbreaks tend to occur every year or every 2–3 years, but can also be sporadic. Overall, HFMD is an important public health concern in children in Asian countries (4,16).
Viruses of the genus Enterovirus (EV) are the common cause of HFMD. Among the hundreds of EV serotypes, Enterovirus 71 (EV-A71) is the major pathogen causing HFMD. This serotype is genetically subgrouped into strains A–F, whereas C4 or C4a is the predominant strain in countries with temperate climates, such as Korea, China, and Japan, and B4 or B5 is predominant in tropical countries, such as Taiwan, Singapore, and Malaysia (5). Due to the lack of antiviral agents, researchers have focused on developing vaccines against EV-A71 to prevent HFMD. Inactivated EV-A71 vaccines based on the C4a genotype have been developed, and production licenses for these vaccines were approved in China in 2015 (1,20,23). However, the circulating serotypes of EV became diverse in the 2010s, as Coxsackievirus (CV) serotypes A6, A10, and A16 (CVA6, CVA10, and CVA16) also emerged as the main causative agents of HFMD. In Asia, the development of a multivalent HFMD vaccine capable of eliciting a protective response against EV-A71, CVA6, CVA10, and CVA16 is currently the main goal in research on HFMD (1,3,9).
In Korea, HFMD epidemics occur every summer, and ∼180,000–400,000 children <5 years of age are affected annually, which represents 10–20% of the <5-year-old pediatric population (10). HFMD has emerged as the most common and most contagious childhood disease for which vaccination is not available. The Korea Centers for Disease Control and Prevention (KCDC) has undertaken case-based sentinel surveillance for EV since 1999. It reported that EV-A71 was predominantly isolated from children with HFMD during 1999–2011, whereas EV-A71, CVA6, CVA10, and CVA16 were most frequently isolated from children with HFMD during 2010–2016 (7,11). Based on published data and sentinel surveillance reports on serotype circulation, the KCDC proposed that EV-A71, CVA6, CVA10, and CVA16 are the candidate serotypes that should be included in HFMD vaccine research. The KCDC has developed two vaccines—one containing inactivated EV-A71 based on C4a genotype and another containing inactivated CVA6, CVA10, and CVA16—and has evaluated their immunogenicity and safety in a mouse model (8,14).
To select candidate serotypes for HFMD vaccine development, serotype-related disease burden should be investigated. The case-based sentinel surveillance only accounts for symptomatic cases and thus presumably underestimates the incidence of disease burden. The immunity among children should also be considered as it provides information about the exposure history (2,12). However, in Korea, the serologic status of children against specific EV serotypes has not been studied. The aim of this study is to investigate age-specific immune status in Korean children by measuring seropositivity rates and neutralizing antibody (NtAb) titers against the candidate serotypes EV-A71, CVA6, CVA10, and CVA16. The data presented in this study will be informative for determining whether these serotypes are suitable for developing an HFMD vaccine.
Methods
Study participants and sample collection
This study was conducted from 2013 to 2018 at St. Paul's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. In April 2019, the hospital was moved to a new location in Seoul, and it was renamed as Eunpyeong St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Pathogen-specific transplacental maternal antibodies mostly decline to undetectable levels within 6 months after birth (15). Considering this fact, this study included children older than 7 months. We used residual serum obtained from children 7 months to 15 years of age who had participated in clinical trials of newly developed vaccines and had undergone health examinations, such as anemia screening, hepatitis B viral marker testing, lead level screening, and allergy testing in this study. Serum samples were centrifuged, aliquoted, and stored at −70°C until testing. The sera of children known to be immunocompromised, receiving immunosuppressive drugs, or suspected of having infectious diseases were excluded from the study. Likewise, sera from children presenting fever, febrile sensation, respiratory symptoms, or gastrointestinal symptoms were also excluded as these children might have an ongoing EV infection and might be at the stage of antibody production. By excluding these children from the study, we aimed to measure only the postinfection antibody levels. Written consent for using residual serum for further research was obtained from parents or legal representatives of all children included in the study. The anonymity of children was assured by permanent removal of any personal identification information, other than data, such as age, sex, and serum collection date, which were retained, and a new survey number was assigned to each serum sample. The consent forms and study protocols were approved by the Institutional Review Board of the study site (PC18TESI0073).
Neutralization test
The neutralization test was performed as previously described (6,17) with minor modifications. The serum samples were inactivated by incubating at 56°C for 30 min, serially diluted two-fold from 1:4 to 1:2,048 and added to 96-well plates. These diluted sera were mixed with equal volumes of test virus (either EV-A71, CVA6, CVA10, or CVA16) suspension with a tissue culture infective dose 50 of 100. The virus–serum mixtures were incubated at 37°C for 2 h. Then, rhabdomyosarcoma cell suspension (1 × 105 cells/mL) was added to each virus–serum mixture. These virus–serum mixtures were incubated in carbon dioxide incubators at 37°C for 7 days. In each batch, cell control, positive serum control, and negative serum control were included. The cytopathic effect (CPE), which indicates viral infection, was observed by microscopy. The NtAb titer was defined as the highest dilution of the serum sample that could inhibit >50% of CPE. The samples with NtAb titer of ≥1:4 were considered seropositive (6,17).
For test virus EV-A71, vaccine strain C4a (8) was used for antibody testing. Unlike EV-A71, CV strains distributed in Korea have not been highly investigated. The CV strains used for the vaccine developed by the KCDC have not been reported yet. Thus, CVA6, CVA10, and CVA16, which are the most widely distributed CV strains in Northeast Asia, were used for test viruses E2, E, and B1b, respectively (19).
Statistical analyses
All statistical analyses were performed using the MedCalc statistical software (version 17.6; MedCalc Software, Ostend, Belgium). Summary statistics were used for analyzing demographic information. Chi-square test was used for the calculation of the seropositivity rates with 95% confidential intervals (CIs) and for comparing the seropositivity rates between the age groups. Chi-square test was also used for the calculation of the proportions of NtAb distributions with 95% CIs and for comparing the NtAb distributions between the age groups. For all statistical analyses, p < 0.05 was considered statistically significant.
Results
The serum samples were collected from 233 participants, but 13 participants (∼5.6%) suspected of having infectious diseases were excluded. Consequently, this study included 220 participants. They were categorized into four age groups: 7 months–2 years, 3–5 years, 6–10 years, and 11–15 years. The number of males and females in each group and mean age of each group are shown in Table 1.
Demographic Characteristics of the Study Participants
SD, standard deviation.
Age-specific seropositivity rates
The overall seropositivity rates of EV-A71, CVA6, CVA10, and CVA16 were 64.1% (95% CI: 57.4–70.4), 73.6% (95% CI: 67.3–79.3), 47.7% (95% CI: 41–54.5), and 34.5% (95% CI: 28.3–41.2), respectively.
The age-specific seropositivity rates of each serotype are shown in Figure 1. For EV-A71, the seropositivity rates increased significantly with age (p < 0.05) in a gradual pattern in the following manner: 42.6% (95% CI: 29.2–56.8) in the 7-month–2-year age group; 64.4% (95% CI: 50.9–76.4) in the 3–5-year age group; 71.1% (95% CI: 57.7–83.2) in the 6–10-year age group; and 77.8% (95% CI: 64.4–88.0) in the 11–15-year age group. The seropositivity rates for CVA6 also steeply and significantly increased with age (p < 0.05), that is, 48.1% (95% CI: 34.3–62.2) in the 7-month–2-year age group, 61% (95% CI: 47.4–73.5) in the 3–5-year age group, 92.5% (95% CI: 81.8–97.9) in the 6–10-year age group, and 94.4% (95% CI: 84.6–98.8) in the 11–15-year age group. For CVA10, participants in the 3–5-year age group presented a significantly higher seropositivity rate than those in other age groups, even the older age groups (p < 0.05). It was 11.1% (95% CI: 4.2–22.6) in the 7-month–2-year age group, 74.6% (95% CI: 61.6–85.0) in the 3–5-year age group, 47.2% (95% CI: 33.3–61.4) in the 6–10-year age group, and 55.6% (95% CI: 41.4–69.1) in the 11–15-year age group. The seropositivity rates for CVA16 were also significantly higher in older age groups (p < 0.05). They were 16.7% (95% CI: 7.9–29.3) in the 7-month–2-year age group, 27.1% (95% CI: 16.4–40.3) in the 3–5-year age group, 41.5% (95% CI: 28.1–55.9) in the 6–10-year age group, and 53.7% (95% CI: 39.6–67.4) in the 11–15-year age group. However, overall seropositivity rates for CVA16 were low.
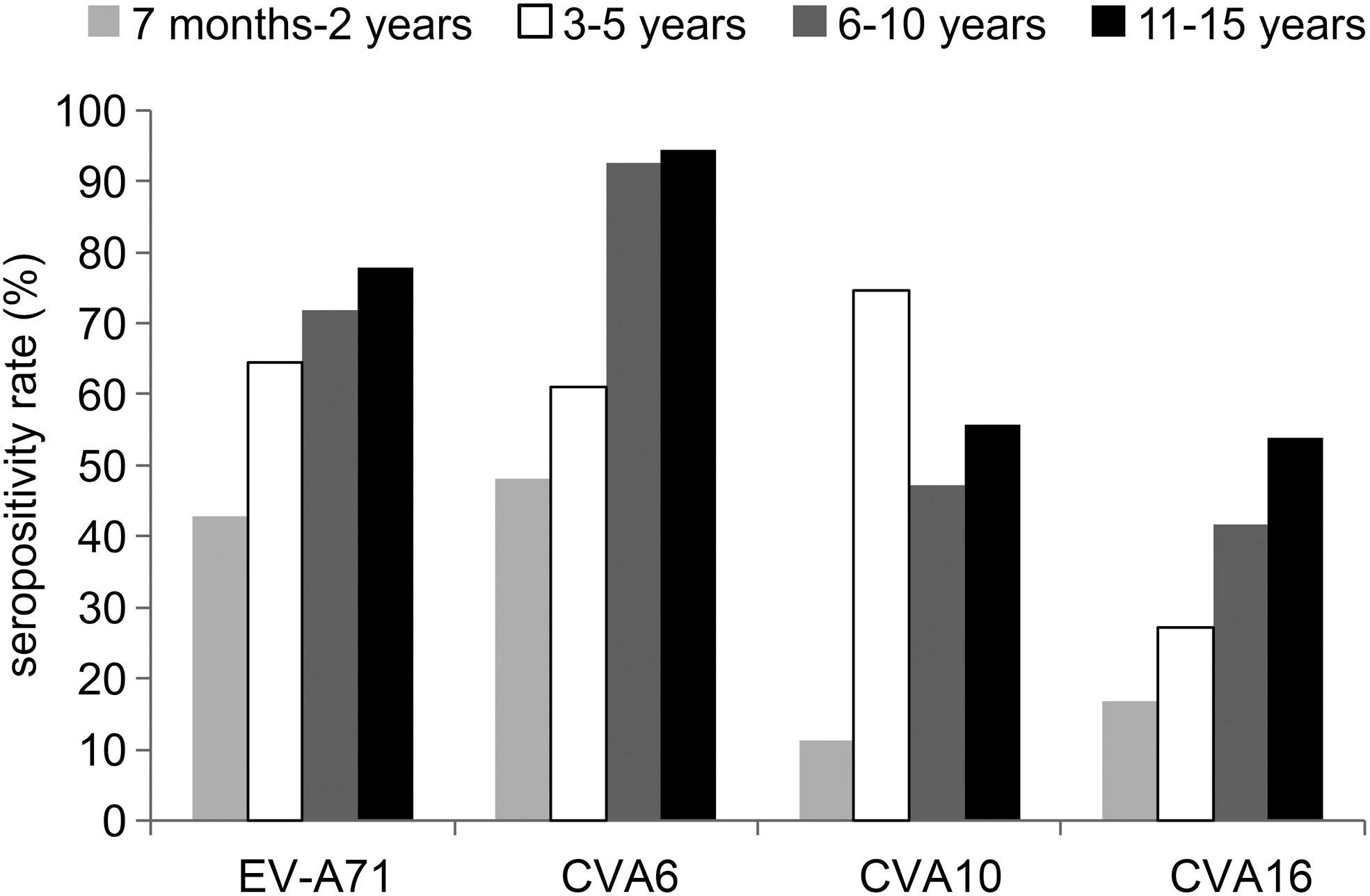
Age-stratified seropositivity rates against EV-A71, CVA6, CVA10, and CVA16. EV-A71, Enterovirus A71; CVA6, Coxsackievirus A6; CVA10, Coxsackievirus A10; CVA16, Coxsackievirus A16.
Distributions of NtAb titers among seropositive participants
Distributions of NtAb titers in EV-A71 seropositive participants are shown in Figure 2, the older children presented with higher NtAb titers.
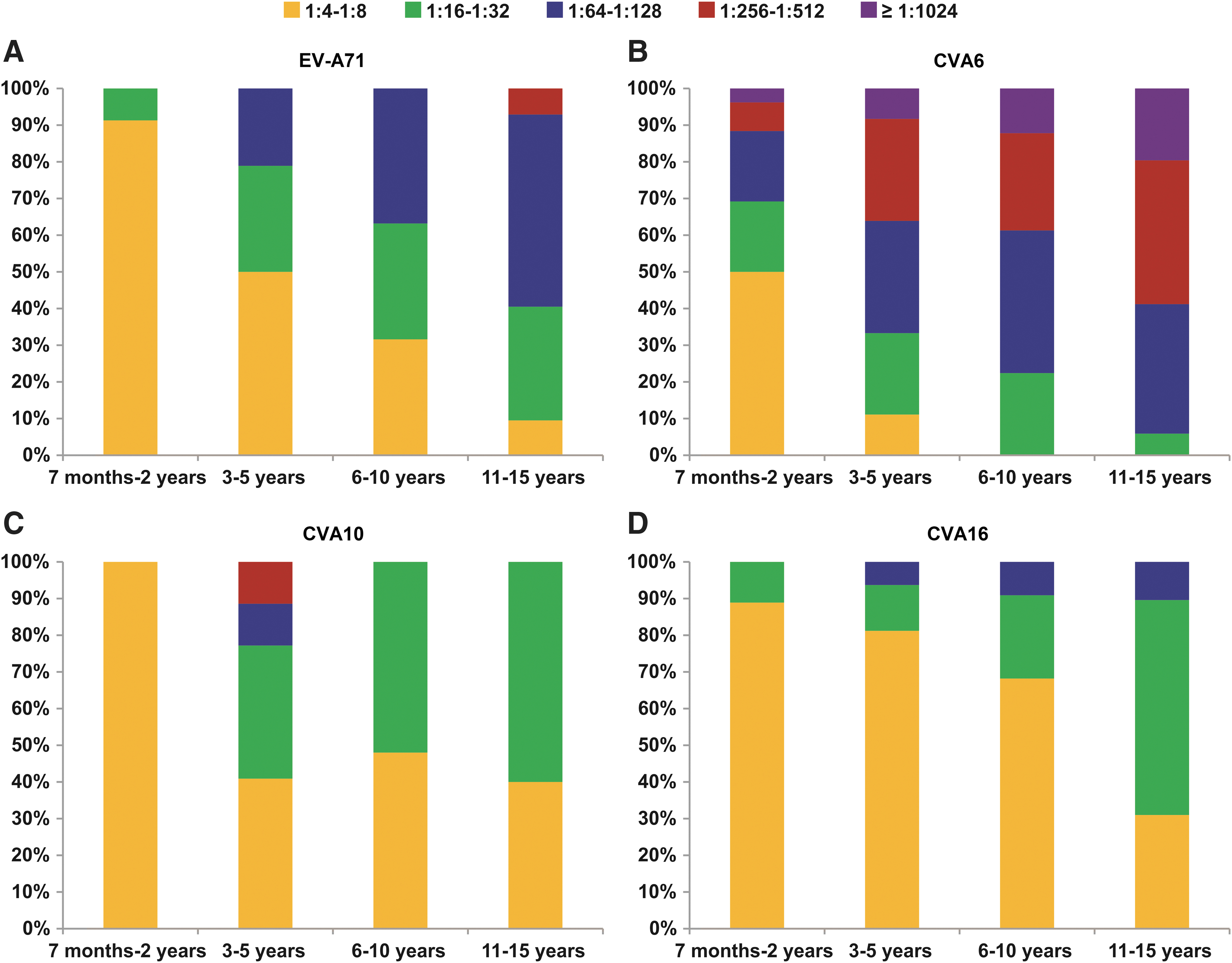
Age-stratified distribution of NtAb titers against
Overall, CVA6 demonstrated higher NtAb titer distributions than EV-A71, CVA10, and CVA16, and the titer ≥1:1,024 was only observed in CVA6. The proportion of the titer ≥1:1,024 among CVA6-seropositive participants also increased with age (p < 0.05) as follows: 3.8% (95% CI: 0.1–19.6) in the 7-month–2-year age group, 8.3% (95% CI: 1.8–22.5) in the 3–5-year age group, 12.2% (95% CI: 4.6–24.8) in the 6–10-year age group, and 19.6% (95% CI: 9.8–33.1) in the 11–15-year age group (Fig. 2).
The distributions of NtAb titers in CVA10-seropositive participants are presented in Figure 2. Participants in the 3–5-year age group showed not only the highest seropositivity rate but also higher NtAb titers. In the 3–5-year age group, more than 10% of the seropositive participants showed titers in the range of 1:64–1:128 and 1:256–1:512 (each). On the contrary, all of the seropositive participants in the 7-month–2-year age group showed titers in the range of 1:4–1:8. All of the seropositive participants in the 6–10-year and 11–15-year age groups showed titers in the range of 1:4–1:8 or 1:16–1:32.
The distributions of NtAb titers in CVA16-seropositive participants are illustrated in Figure 2. The older children presented higher NtAb titers, which is similar to the trend observed in case of EV-A71 and CVA6. However, the NtAb titers in CVA16-seropositive participants were in low ranges, mostly in 1:4–1:8 or 1:16–1:32. Furthermore, none of the seropositive participants demonstrated the titer of ≥1:256–1:512.
Discussion
In this study, age-stratified seropositivity rates and NtAb titer distributions of EV-A71, CVA6, CVA10, and CVA16 in Korean children were investigated. Our findings showed that EV-A71 and CVA6 are optimal candidate serotypes for the development of HFMD vaccine, whereas further data are needed for CVA10 and CVA16.
For EV-A71, the overall seropositivity rate was 64.1%, which is the second highest among the candidate serotype rates. The seropositivity rates and NtAb titer ranges showed an increasing trend with age, indicating that children are being continuously exposed to EV-A71 over time, and they often experience repetitive infections. Older children may have increased chance of having been exposed. This serological finding suggests that EV-A71 is the major pathogen of HFMD and that its inclusion in vaccines is suitable.
For CVA6, in comparison to other serotypes, higher seropositivity rates and higher NtAb titer ranges were observed in all age groups. These results indicate that children were predominantly exposed to and repeatedly infected with CVA6. The results further highlight that inclusion of CVA6 in the HFMD vaccine is a suitable strategy in vaccine development.
For CVA10, participants in the 3–5-year age group showed higher seropositivity rates and higher NtAb titer distributions than participants in the older age groups. This observation indicates that children 3–5 years of age are frequently exposed to CVA10, but those from other age groups are not. As far as HFMD incidence is concerned, children <5 years of age are most commonly affected by the EV serotypes. This observation presumably suggests that the exposure has occurred only in recent years. Further study is needed to analyze whether the exposure of children to CVA10 is transient or recurrent.
For CVA16, seropositivity rates and NtAb titer ranges increased with age; however, these rates and titer ranges were generally low. This finding indicates that very few children were exposed to CVA16. Further study is needed to show if children were frequently exposed to CVA16.
Discrepancies were observed between the results of case-based surveillance and serological investigation, but both methods have advantages and disadvantages with respect to estimating serotype-related disease burden for vaccine development. Case-based surveillance is the fastest way of identifying circulating serotypes and is useful for monitoring the trends. Real-time polymerase chain reaction (PCR) performed on swab samples is less laborious and less costly. However, case-based surveillance does not include asymptomatic cases and tends to include only severe cases, and thus, lacks representativeness. Ranking of serotypes based on quantities may skew the delicate circulating pattern of serotypes. A serological investigation reflects past exposure regardless of the degree of symptoms. However, it requires blood samples and an appropriate antibody detection assay, which is more costly than PCR. An integrated approach of the two methods is required for estimating the disease burden (2,12).
The serological survey performed in this study improved the estimation of the disease burden associated with CVA6. CVA6 was ranked in five most frequent serotype first in 2010 and then was retained at the rank five since 2012, but it was not the topmost common serotype every year (7,11,21,22). This study showed that seropositivity rates and NtAb titer ranges for CVA6 were higher than expected. Thus, many children are presumably asymptomatic for CVA6 infection.
The age-specific serological result of this study contributes to the recognition of the delicate circulation patterns of serotypes. For CVA10, the observation of the highest seropositivity rates and NtAb titer ranges in the 3–5-year age group—among all the age groups—seems to reflect a recent emergence of CVA10. This observation prompted us to assess whether CVA10 circulation is transient or recurrent. For CVA16, the participants generally exhibited low seropositivity rates and NtAb titer ranges, suggesting limited circulation of CVA16 and prompted us to investigate whether CVA16 continuously circulates. According to the results of the case-based surveillance, CVA10 and CVA16 are the most frequent serotypes alongside EV-A71 and CVA6 based on quantity. However, at the granular level, EV-A71 and CVA6 are frequently detected every year, unlike CVA10 and CVA16. CVA10 circulates in 2–3-year cycles, and it was predominant in 2015, 2017, and 2018. CVA16 circulates in 2–3-year or 3–4-year cycles (7,11,21,22). Delicate circulation patterns have been overlooked as a result of just summing the quantities.
There are differences in serological results among Asian regions. Lerdsamran et al. (13) have assessed the immune statuses of Thai children against EV-A71 and CVA16. The authors have reported increasing trends of seropositivity rates and NtAb titer ranges for EV-A71 (C4a), consistent with the results presented in this study. For CVA16 (B1b), Thai children exhibit higher seropositivity rates and NtAb titer ranges than Korean children (13). In a study conducted on Chinese children, an increasing seropositivity pattern of EV-A71 has been observed, in line with our results. The same report also mentions the overall low seropositivity for CVA16. However, the reported seropositivity for CVA6 is not as high as what we observed. Unlike the participants in our study, Chinese children exhibit increased seropositivity rates for CVA10 as they grow (24). For EV-A71, which has circulated in Asia for more than a decade, similar serological patterns have been observed among different regions and populations. In contrast, recently emerged serotypes show different serological patterns based on the region or population. Such region-specific immunity is important in the selection of the candidate serotypes for vaccine development. Thus, selecting candidate serotypes based on reported data pertaining to other regions is inappropriate.
To our knowledge, this is the first study to investigate the immunity of Korean children against EV. It is also the first to focus on the serological status of children against emerged candidate serotypes for developing a multivalent vaccine. More importantly, when selecting the candidate serotypes for HFMD vaccine development, we noted inconsistencies between the data from case-based surveillance and our findings. However, certain limitations, such as the small number of participants and the choice of a single region to conduct the study, need to be addressed. Due to scarce data on CV strain distribution of Korea, we used the most widely distributed strain in Asian region in CV antibody testing. Crossreactivity among various strains of the same serotype has been reported (1,11); thus, we believe that the estimation of serotype-related past infections was not influenced.
To develop an HFMD vaccine, further studies evaluating the immune statuses of larger study populations are needed. The search for target serotypes should be widened to identify whether there are more suitable candidate serotypes among the newly emerged serotypes. The sentinel surveillance should be enhanced to include a large number of samples from a large number of hospitals, and the strain distribution of CV needs to be evaluated.
Conclusions
The process of serotype selection for developing HFMD vaccine for children should involve consideration of the circulating serotypes of the causative agents of HFMD as well as the immune status of the children indicating past infections. This study elucidated the age-stratified serological status for candidate serotypes (EV-A71, CVA6, CVA10, and CVA16) among Korean children. These serotypes serve as candidates for the development of HFMD vaccine. Although inclusion of these serotypes in the HFMD vaccine is trending in Asian countries, including Korea, the results of seropositivity and NtAb titer ranges in this study showed that EV-A71 and CVA6 are the suitable candidate serotypes, and further study is needed for CVA10 and CVA16. The findings of this study provide a novel perspective regarding HFMD vaccine development. Additionally, this study emphasized that an integrated approach based on case-based surveillance data and age-specific immunity data is essential for estimating disease burden. The report presented in this study is expected to serve as reference material when making policies for HMFD in Korea and other Asian countries.
Footnotes
Acknowledgments
The authors acknowledge the financial support from the Catholic Medical Center Research Foundation provided in the program year of 2019. The study was partially supported by the corresponding author.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Catholic Medical Center Research Foundation provided in the program year of 2019 (grant number: 5-2019-0001-00238).