
Abstract
The spectrum of coronavirus disease 2019 (COVID-19) severity, related to cellular immune functions, has not been fully clarified yet. Therefore, this study aimed to investigate the alteration of peripheral blood cells in patients with COVID-19. The flow cytometric characterization of immune cell subset was performed on 69 COVID-19 patients and 21 healthy controls. These data were evaluated based on the disease severity. A total of 69 patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) were classified as asymptomatic infection (n = 14), nonsevere (n = 39), and severe (n = 16) groups. Decreased lymphocytes and increased CD14 + 4- monocytes are found in patients with severe COVID-19. Decreased CD4 expression level was observed in the monocytes of patients with severe COVID-19. The total lymphocytes, B and T lymphocytes, CD4+ cells and CD8+ cells, and natural killer (NK) and natural killer T (NKT) cells were found to be decreased in patients with severe COVID-19. The CD4+/CD8+ ratio was not significantly different between patients with COVID-19 and healthy controls. The percentage of activated T cells (CD3+HLA-DR+) and B cells (CD19+CD38+) was lower in patients with severe COVID-19. Age and CD4− monocytes were independent predictors of disease severity. The SARS-CoV-2 infection may affect lymphocyte subsets, resulting in decreased T and B cells, monocytes, and NK and NKT cells. Decreased CD4 expression level by monocytes was significantly correlated with disease severity. Further studies on the host immune response to SARS-CoV-2 infection are necessary to predict the disease severity and protect against the virus.
Introduction
In December 2019, cases of pneumonia of unknown etiology were reported in China, and the epidemic disease was named as coronavirus disease 2019 (COVID-19). The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of the disease, was identified in January 2020. This novel coronavirus has rapidly spread and become a worldwide pandemic (14,32). Patients with COVID-19 have been reported to experience a range of clinical manifestations, from no symptoms to critical illness. Since then, classifications based on disease severity have been widely used during the follow-up and treatment of patients with COVID-19 (3,16).
The COVID-19 classification was mainly based on the diagnostic evaluation and laboratory as well as clinical features. Pulmonary imaging (chest X-ray, or if indicated, computed tomography [CT], and laboratory evaluation including complete blood count [CBC]) with differential and metabolic profile, including liver and renal function tests, was performed for the patient evaluation. Measurements of inflammatory markers such as C-reactive protein (CRP), D-dimer, and ferritin, might be performed for prognostic value in patients with COVID-19. Since the first COVID-19 case was reported in Turkey, each patient with COVID-19 has been evaluated based on medical history, symptoms, severity assessment on admission, laboratory findings, and chest CT.
Up to the present, some laboratory features such as lymphopenia, elevated CRP, D-dimer, and liver enzymes have been associated with severe illness (7). Moreover, disease severity in patients might be due to not only viral infection but also the host immune response (21). Secretions of some cytokines (such as interleukin (IL)-6, IL-8, IL-2, IL-10, IL-1β, IL-18, and tumor necrosis factor-α) have been reported to attract immune cells and play an important role in poor disease outcome (15,18,22,27,29). Lymphopenia, inefficient T and B cell immunity, and cytokine storm may cause severe disease (1). However, only a few studies of SARS-CoV-2 infection from China found that decreased total lymphocytes, T lymphocyte, and B lymphocyte were associated with severe illness (10,25). Furthermore, the full spectrum of COVID-19 severity, related to cellular immune functions, has not yet been clarified.
A flow cytometry analysis was performed to investigate peripheral white blood cell changes particularly in lymphocytes and monocytes, which are important for immune protection against viral infections, among patients with COVID-19 admitted to our hospital (the Ankara City Hospital in Turkey). Then, patients were divided into groups according to disease severity, and results were compared with that of healthy controls.
Materials and Methods
Study design and participants
The study group enrolled patients with COVID-19 (aged 16–82 years) who were hospitalized in a tertiary hospital from April 25 to May 25, 2020. A total of 21 healthy individuals and 69 patients with COVID-19 were included in the study. Diagnosis was confirmed by detecting SARS-CoV-2 RNA in oro/nasopharyngeal swab samples.
Data were collected from each patient with COVID-19 using the data collection form. The following variables were recorded for each patient: age, sex, medical history, symptoms, severity assessment on admission, laboratory findings, chest CT, and treatment. On admission, patients were categorized into three groups: asymptomatic (asymptomatic infection), nonsevere (mild and moderate illness), and severe (severe and critical illness)) according to the National Institutes of Health (NIH) classification based on COVID-19 severity (3).
The asymptomatic infection was defined as follows: positive test for SARS-CoV-2 by PCR in oro/nasopharyngeal swab samples, but no symptoms and no abnormal chest imaging.
Severe illness was defined as follows: respiratory frequency of >30 breaths/min, SpO2 of ≤93% on room air at sea level, ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) of <300, or lung infiltrates of >50%.
In addition, healthy individuals without any chronic disease and tested negative for SARS-CoV-2 by PCR in oro/nasopharyngeal swab samples were selected as the control group.
The ethics committee of the Ankara City Hospital approved this study design (confirmation date and number: 21.05.2020/E1-20-618). This study was conducted in accordance with the principles of the Declaration of Helsinki.
Immunophenotyping of monocytes and lymphocytes
Venous blood samples were collected from the participants on hospital admission. The time from onset of symptoms of the patients to admission was 4.5 ± 3.8 days. CBC was performed in a hematology analyzer, the ADVIA ® 2120i (Siemens Healthineers, Germany). Immunophenotyping of leukocytes was performed using a 10-color flow cytometer Navios (Beckman-Coulter). All ethylenediaminetetraacetic acid-anticoagulated blood samples were analyzed on the day of collection. Sample preparation and analyses were performed according to the manufacturer's instructions. The leukocyte count of patients was obtained from CBC results and adjusted to be <104 cells/μL. The median (min–max) number of cells acquired on the flow cytometer from 100 μL blood samples was 6050 (3210–9840) cells/μL. About 100 μL aliquots of blood were vortexed and incubated in the dark with combinations of the following fluorochrome-conjugated monoclonal antibodies for 15 min at room temperature: CD3-FITC (fluorescein-5-isothiocyanate, Clone UCHT1), CD14-PE (phycoerythrin, Clone RM052), CD4-ECD (PE-Texas Red, Clone RMD52), CD19-PC5 (phycoerythrin-cyanin5; Clone J3-119), CD8-PC7 (phycoerythrin-cyanin7, CloneSFC121Thy2D3), CD38-APC (allophycocyanin, Clone LS198-4-3), CD56-A700 (APC-Alexa Fluor 700, Clone N901), CD16-A750 (APC-Alexa Fluor 750, Clone 3G8), HLADR-PB (Pacific Blue, Clone Immu-357), and CD45-KO (Krome-Orange, Clone J33). After incubation, red blood cells were lysed with the addition of 1 mL of VersaLyse Lysing Solution (Beckman-Coulter), and samples were analyzed using flow cytometry (Beckman-Coulter Navios) after a 10-min incubation at room temperature. Data analyses were performed with the Kaluza software.
After selecting the viable cells, physical gating was performed on CD45 and side scatter (SS). CD14 positivity was used for monocyte gating, and the lymphocyte population was identified to be low SS and bright CD45 expression. Then, different lymphocyte subpopulations were identified by immunophenotyping markers. Gating strategy of the three monocyte subsets was based on relative CD14 and CD16 expression. In flow cytometry analysis, classical monocytes express high CD14 levels but no CD16, intermediate monocytes express high CD14 and low CD16 levels, whereas nonclassical monocytes express low CD14 but high CD16 (15). During the analyses, a group of monocytes were observed to lose their CD4 expression, especially in patients with severe COVID-19. Therefore, CD4+ and CD4− monocyte groups were gated and compared between patients. The gating strategy of the studied parameters is shown in Supplementary Figure S1.
Internal quality control check was performed at a daily basis according to the manufacturer's instructions, and the UK NEQAS External Quality Assessment program was used for the external quality assessment.
Statistical analysis
Continuous data were presented as median with IQR, and categorical data were presented as percentages. Differences between groups were compared using the nonparametric Kruskal–Wallis test, and for the significant (p < 0.05) results, the Mann–Whitney test was performed. Moreover, a binary logistic regression analysis was performed to define independent predictors of disease severity. In the analysis, a forward (Wald) method was used. The odds ratio was calculated for significantly associated variables. Multivariate correlation analysis was performed between parameters and clinical outcomes of the disease. All statistical calculations were made using the “SPSS for Windows version 26” software program (SPSS Inc., IBM Corporation, Chicago, IL).
Results
Baseline characteristics and CBC analysis of healthy individuals and patients with COVID-19 are shown in Table 1 and Figure 1, respectively.
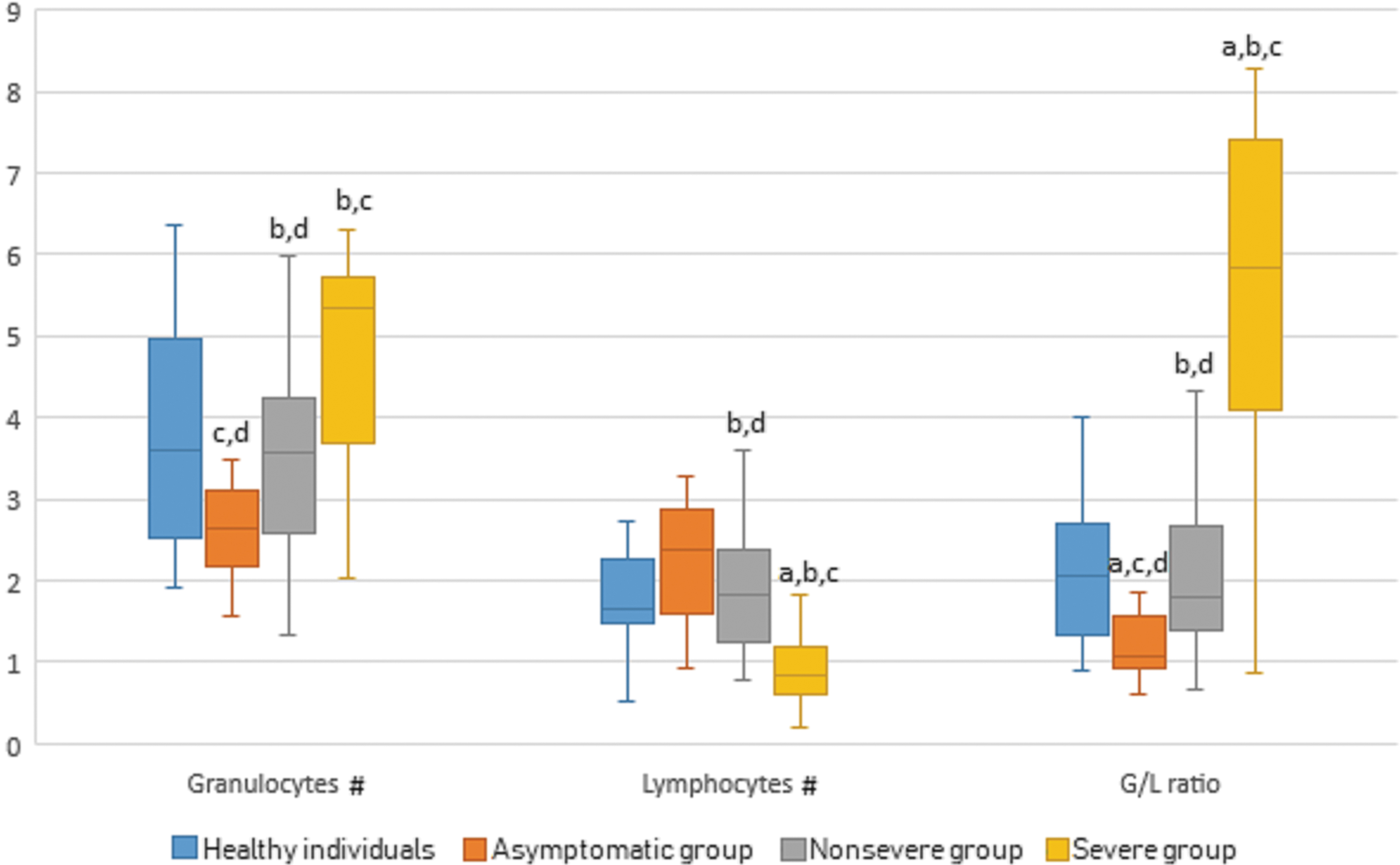
Granulocyte and lymphocyte counts and granulocyte/lymphocyte ratio in CBC analysis of healthy individuals and patients with COVID-19. #, 1 × 109/L.
Demographics and Baseline Characteristics of Healthy Individuals and Coronavirus Disease 2019 Patients
Data are median (IQR) or (min–max); #, 1 × 109/L.
Statistically significant than healthy individuals group.
Statistically significant than asymptomatic group.
Statistically significant than nonsevere group.
Statistically significant than severe group.
Bilat., bilateral; CBC, complete blood count; COPD, chronic obstructive pulmonary disease; G/L ratio, granulocyte/lymphocyte ratio; IQR, interquartile rage.
Data on cell proportions are summarized in Table 2 and Figure 2 (gating strategy shown in Supplementary Fig. S1). Granulocyte, monocyte, and lymphocyte cell populations were analyzed and compared between the groups and subpopulations as follows.
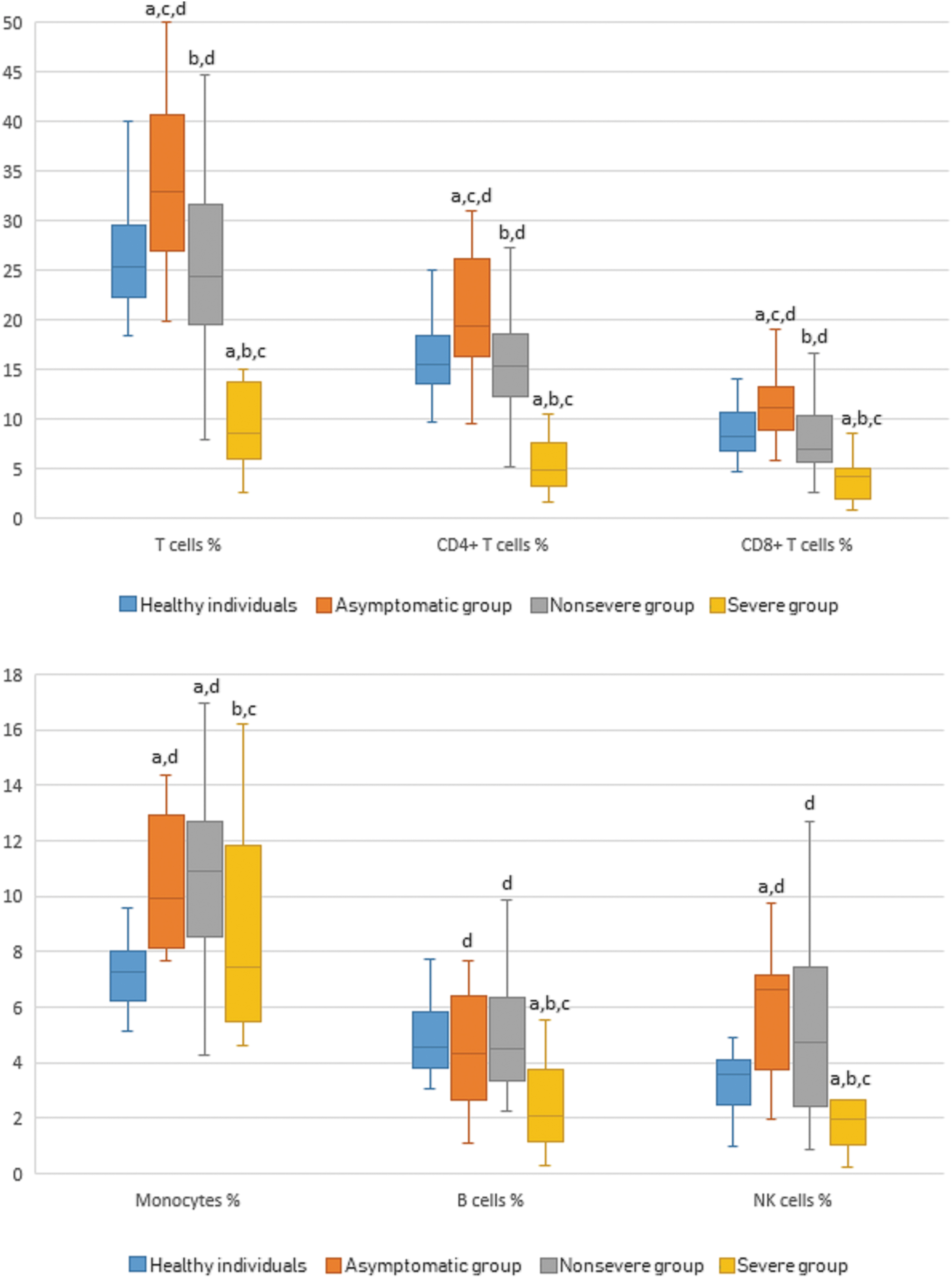
Peripheral lymphocyte subsets' and monocytes' percentages* in flow cytometric analysis (gating strategy shown in Supplementary Fig. S1) of healthy individuals and COVID-19 patients. *In percentage of leukocytes.
Percentage Values for Lymphocyte Subsets and Monocytes in Adult Peripheral Blood of Healthy Individuals and Coronavirus Disease 2019 Patients (Gating Strategy Shown in Supplementary Fig. S1)
Data are median (IQR), *in percentage of leukocytes.
Statistically significant than healthy individuals group.
Statistically significant than asymptomatic group.
Statistically significant than nonsevere group.
Statistically significant than severe group.
Classical m., classical monocytes; G/M ratio, granulocyte/monocyte ratio; Interm. m., intermediate monocytes; L/M ratio, lymphocyte/monocyte ratio; n, number of participants; NK, natural killer; Non-clas.m., nonclassical monocytes.
Granulocytes
According to the results, the percentage of granulocytes was found to increase in the severe group (p < 0.001), whereas it was found to decrease in the asymptomatic group (p < 0.001) when compared with healthy individuals. The asymptomatic group had a significantly lower percentage of granulocyte levels than both nonsevere (p = 0.020) and severe groups (p < 0.001).
Monocytes
The percentage of monocyte levels was higher in asymptomatic and nonsevere groups than both healthy individuals (p < 0.001, p < 0.001; respectively) and severe group (p = 0.029, p = 0.014; respectively).
Monocytes were further divided into three subgroups according to CD14 and CD16 expression levels. Classical monocytes were higher in the asymptomatic and nonsevere groups than healthy individuals (p = 0.002, p < 0.001; respectively). The nonsevere group had a higher classical monocyte ratio than the severe group (p = 0.013). No significant difference was observed between the asymptomatic and nonsevere groups (p = 0.732) and between the asymptomatic and severe groups (p = 0.058). Intermediate monocyte ratios were lower in healthy individuals than that in the nonsevere group (p = 0.001). No significant difference was observed between the other groups. Nonclassical monocytes were lower in the severe group than both healthy individuals and asymptomatic group (p = 0.011, p = 0.041; respectively.)
An interesting finding was monocytes decreased the mean fluorescent intensity of CD4 expression correlated with disease severity (Fig. 3, gating strategy shown in Supplementary Fig. S1). Minimum and maximum values of the median fluorescent intensities (MFIs) were 1.70–5.93, 2.65–5.97, 1.36–5.69, and 0.43–3.80 for healthy individuals, asymptomatic, nonsevere, and severe groups, respectively. The percentage of CD4− monocytes based on CD4 MFIs was significantly higher in the severe group than healthy individuals, asymptomatic group, and nonsevere groups (p < 0.001, p < 0.001, p < 0.001; respectively). The nonsevere group had a higher CD4− monocyte ratio than healthy individuals and asymptomatic group (p < 0.001, p = 0.016; respectively).
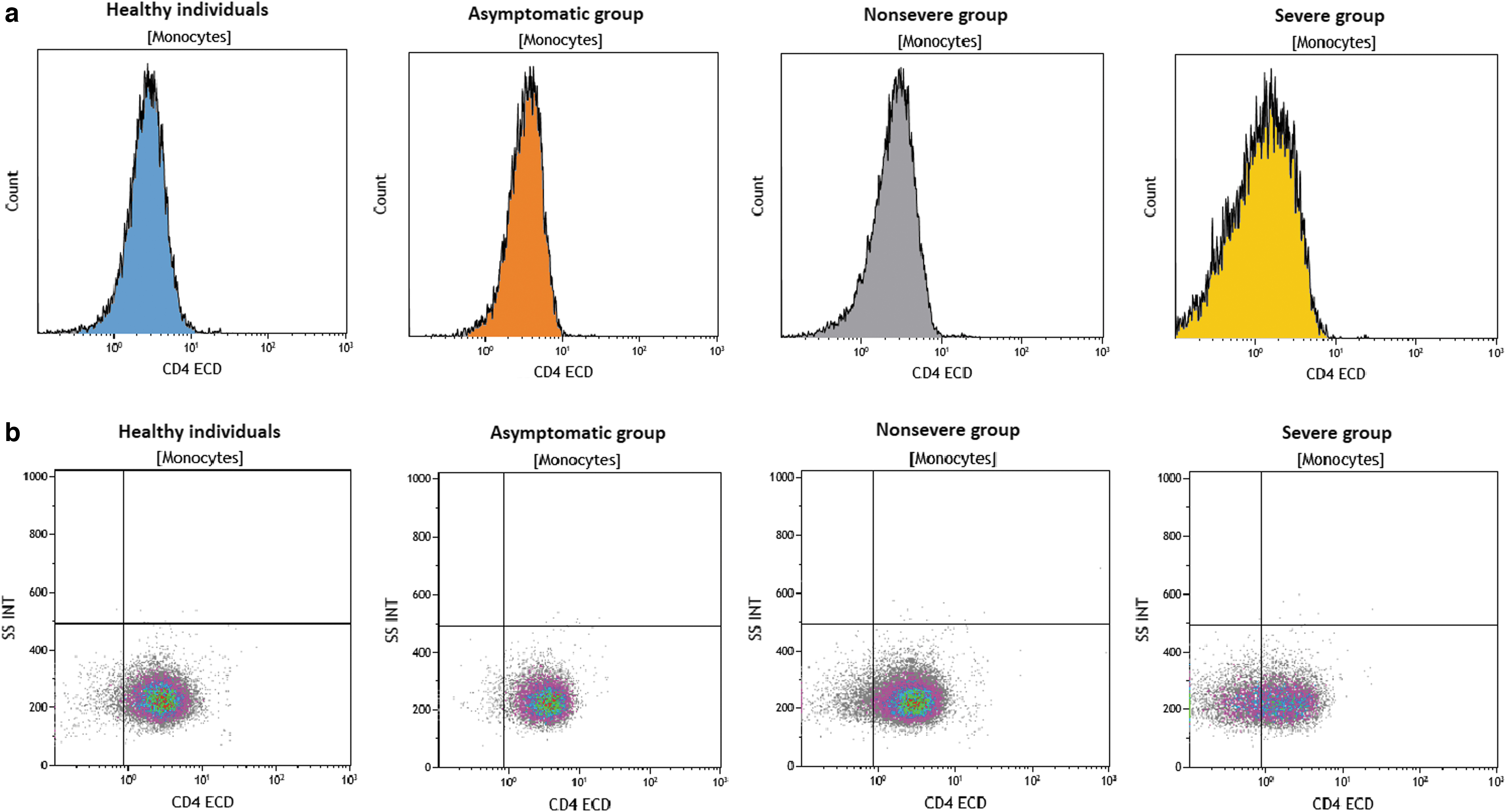
CD4 collective MFI results of monocytes in flow cytometry analyses (gating strategy shown in Supplementary Fig. S1).
Lymphocytes
The percentage of lymphocytes, B lymphocytes, and T lymphocytes was significantly lower in the severe group than healthy individuals, asymptomatic group, and nonsevere group (p < 0.001, p < 0.001, p < 0.001; respectively). The percentage of lymphocytes was significantly lower in the nonsevere than in the asymptomatic group (p = 0.028). The percentage of T lymphocytes was significantly higher in the asymptomatic group than that in healthy individuals (p = 0.010) and nonsevere group (p = 0.006). Activated B cells (CD19+CD38+) were significantly lower in the severe group than that in the asymptomatic and nonsevere groups (p = 0.010, p = 0.002; respectively), but were higher in the asymptomatic and nonsevere groups than healthy individuals (p = 0.015, p = 0.001; respectively). CD4+ T cells and CD8+ T cells were also significantly lower in the severe group than healthy individuals, asymptomatic, and nonsevere groups (p < 0.001, p < 0.001, p < 0.001 for both; respectively). The asymptomatic group had higher CD4+ T cells and CD8+ T cells than the nonsevere group (p = 0.016, p = 0.003; respectively) and healthy individuals (p = 0.026, p = 0.015). CD4/CD8 ratio was not statistically different between groups (p > 0.05). Activated T cells (CD3+HLA-DR+) were significantly lower in the severe group than healthy individuals, asymptomatic group, and nonsevere group (p < 0.001, p < 0.001, p < 0.001; respectively).
The percentage of natural killer (NK) and natural killer T (NKT) cells was significantly lower in the severe group than healthy individuals, asymptomatic group, and nonsevere group (p = 0,010, p = 0,001, p = 0.001 for NK cells and p = 0.001, p = 0.001, p < 0.001 for NKT cells; respectively). Asymptomatic group had a higher percentage of NK cells than healthy individuals (p = 0.003).
Granulocyte/lymphocyte (G/L) ratio was significantly higher in the severe group than healthy individuals, asymptomatic group, and nonsevere group (p < 0.001, p < 0.001, p < 0.001; respectively). The asymptomatic group had a significantly lower and the nonsevere group had a significantly higher G/L ratio than healthy individuals (p = 0.002, p = 0.025; respectively).
Granulocyte/monocyte ratio was significantly higher in the severe group than asymptomatic and nonsevere groups (p < 0.001, p < 0.001; respectively). Asymptomatic and nonsevere groups had a significantly lower granulocyte/monocyte ratio than healthy individuals (p < 0.001, p < 0.001; respectively).
Lymphocyte/monocyte ratio was significantly lower in the severe group than healthy individuals, asymptomatic group, and nonsevere group (p < 0.001, p < 0.001, p < 0.001; respectively).
All of the studied parameters were compared according to the age and sex differences. To compare the groups according to the age, five groups were organized (<30; 31–40; 41–50; 51–60; >60) and compared. Results showed that age was a contributory factor to parameter levels (B cell p = 0.010, NKT p = 0.002, T cell p < 0.001, activated T cell p = 0.013, CD4+ T cell p < 0.001, CD8+ T cell p < 0.001, CD4− monocyte p < 0.001, and G/L p < 0.001). However, gender did not affect the parameters significantly. Age and gender have been known to affect the disease severity significantly; therefore, to determine the independent predictors of disease severity, a binary logistic regression analysis (forward) was performed. The model correctly classified 91.3% of cases. The binary logistic regression model included age, gender, CD4− monocytes, T cells, and G/L ratio. The model showed that age and CD4− monocytes were independent predictors of disease severity. The logistic regression model was statistically significant with χ 2 = 34,490; p < 0.001. Increasing age and CD4− monocyte percentage were independent predictors of disease severity with odds ratios of 1.123 and 7.186, respectively. Based on this statistical analysis, the most significant parameter was found to be CD4− monocytes, independent of the effect of age and gender.
Disease severity was significantly correlated with age (r = 0.637, p < 0.001), B cell (r = −0.278, p = 0.008), T cell (r = −0.406, p < 0.001), CD4+ T cell (r = −0.372, p < 0.001), CD8+ T cell (r = −0.385, p < 0.001), CD4− monocytes (r = −0.587, p < 0.001), and G/L ratio (r = 0.397, p < 0.001).
Discussion
This study investigated the peripheral blood cell distribution in patients with COVID-19 by flow cytometry analysis. Our results show that in patients with COVID-19, peripheral white blood cells, especially decreased lymphocytes and monocytes, were shown in severe COVID-19, and CD14 + 4- monocyte increase related to the disease severity.
The control of viral infections involves complex interactions between immune system cell types. Lymphocytes and subsets, including CD4+ T cells, CD8+ T cells, B cells, and NK cells, play an important role in the maintenance of immune system function. Previous studies reported that decreased CD3+ T cells, CD4+ T cells, CD8+ T cells, and NK cells in SARS-CoV-2 infection are related to disease severity (10,18). One of the most important issues in this novel coronavirus infection is that some people do not have any symptoms, whereas others experience acute respiratory distress syndrome. In this study, changes in peripheral blood cells were evaluated by the disease severity and to contribute to understanding the SARS-CoV-2 infection immunity. Patients with symptoms were divided into two groups according to disease severity and compared with asymptomatically infected patients and healthy controls. The cohort of 69 patients has been reported with SARS-CoV-2 infection and 21 healthy controls in this study. Based on the results obtained from study groups, the granulocyte level was found to be higher in patients with severe COVID-19, whereas lower percentages were found in the asymptomatic group.
Monocytes/macrophages participate in both expressions of innate immunity and in the development of adaptive immune responses (19). Pence reported that monocytes would be principal players of cytokine storm in COVID-19 (18). Moreover, monocytes and T lymphocytes have been known to immigrate into the infected site in immunopathogenesis of COVID-19 (22,27). Higher granulocyte level and lower monocyte and lymphocyte levels in the blood of patients with severe COVID-19 were found in the study, supporting these early findings. Zhou et al. showed that monocytes were lower in both ICU and non-ICU patients than healthy controls (31). Based on these findings, monocytes of both nonsevere and asymptomatic groups were significantly higher than that of healthy controls. Conversely, the severe group had lower monocytes than the nonsevere and asymptomatic groups. Such increase in monocytes, which constitute the first step of antiviral immunity, may be associated with good disease prognosis.
Three distinct blood monocyte subsets were identified in three major populations based on CD14 and CD16 expression: classical (CD14+CD16−), intermediate (IM; CD14+CD16+), and nonclassical (NCM; CD14dimCD16+). Increased IM and NCM percentages have been reported under inflammatory conditions; however, little is known about monocyte subsets at the onset of inflammation (11,26). Classical monocytes were found to be primed for phagocytosis, immune responses, and migration (28). Intermediate monocytes are specialized in antigen presentation, whereas nonclassical monocytes are responsible for the antiviral responses (11). Hoeve et al. showed a decreased percentage of CD14-positive cells and an increased percentage of CD14dim cells (CD14+CD16++) after an influenza A infection but was not statistically significant (8). Zhou et al. showed that the percentage of inflammatory monocytes (CD14+CD16+) is higher in patients with severe COVID-19. They also found that a significant expansion of populations with CD14+CD16+ monocytes producing IL-6 was also observed in the peripheral blood of ICU patients with COVID-19 than of those who did not require ICU hospitalization (31). In this study, monocytes were classified as classical, intermediate, and nonclassical according to CD14 and CD16 expression levels, and nonclassical monocytes found to be associated higher CD16 intensity were lower in patients with severe COVID-19 rather than intermediate monocytes with CD16-positive monocytes. In accordance with this study, Gatti et al. showed decreased nonclassical monocytes in patients with severe SARS-CoV-2 infection (5). A study of a Spanish cohort suggested that inflammatory transitional (CD14+CD16+) and nonclassical monocytes migrate from the blood to lungs in patients with severe COVID-19 (20).
The correlation between total CD16+ monocytes consisting of the total of intermediate and nonclassical monocytes was also investigated, and no significant correlation was observed between disease severity and total CD16+ monocytes.
An interesting finding for monocytes was that decreased mean fluorescent intensity of CD4 expression was correlated with disease severity. To our best knowledge, CD4 expression on monocytes in SARS-CoV-2 infection has not been characterized previously. Moreover, a significantly reduced CD4 expression is found in patients with severe COVID-19. Although the role of the CD4 molecule in human monocyte development and function is not yet fully understood, a novel differentiation pathway mediated by activating the CD4 expressed on peripheral monocytes has been reported and CD4 activation has triggered monocytes to differentiate into macrophages that contribute to two key innate immune functions: cytokine secretion and phagocytosis (30). The rationale behind testing the expression level on monocytes in this study was an observation during the data analysis that patients with severe COVID-19 had significantly decreased CD4 expression. This observation might be a reason for these patients not to provide the necessary immune response because the CD4-mediated activation of monocytes is decreased.
NK cells are a type of innate lymphoid cells that contribute to the cytolytic killing of virus-infected cells. Whether NK cells also play a direct antiviral role in coronaviruses is still unknown (23). NKT cells also promote antibody responses during viral infection (7). Results of this study show that the percentage of NK and CD3+CD56+ NKT cells is significantly lower in patients with severe COVID-19 than that in other groups. Similarly, the asymptomatic group had higher NK cells than healthy controls. Jiang et al. reported decreased NK cells in severe patients, which is similar to the results of this study (10).
Data from other analyses showed that total lymphocytes, B lymphocytes, and T lymphocytes were significantly lower in severe disease, as previously reported (24). Furthermore, CD4+ T cells and CD8+ T cells decreased in patients with severe COVID-19 in accordance with the recent studies (2,9,13). No differences in CD4+/CD8+ ratio were observed between groups in this cohort, such as those in previous studies (4,25). Wang et al. reported that no difference was observed in CD4+/CD8+ ratio with severity and found no changes in this ratio at post-treatment (25).
A decreased percentage of activated T cells (CD3+HLA-DR+) was observed in patients with severe COVID-19. Wang et al. reported an increased activation marker (HLA-DR) of T cells, but a decreased costimulatory molecule CD28 with severe illness (24). These early data, in contrast to the actual data, might show that existing activated lymphocytes appear to be increased, but might not be functional. Simultaneously, activated B cells (CD19+CD38+) were lower in patients with severe COVID-19. Therefore, whether active B cells are sufficient or functional or can synthesize neutralizing antibodies for protection against the virus remains to be elucidated.
In the study, some ratios were evaluated. According to the results, higher G/L and granulocyte-to-monocyte ratios and lower lymphocyte-to-monocyte ratio were observed in patients with severe COVID-19. These findings were in accordance with previous studies in which lymphopenia and high neutrophil-to-lymphocyte ratios were found to be associated with disease severity (7,12,18).
In conclusion, peripheral lymphocyte subset alteration was clearly associated with SARS-CoV-2 infection. Results demonstrated that increased granulocytes and decreased total lymphocyte count, CD +3 T cells, CD4+ T cells, and NK cells and monocytes were associated with severe SARS-CoV-2 infection. To the best of our knowledge, this is the first study that described the CD4 MFI expression on monocytes in patients with COVID-19; the decrease of CD4 MFI expression on monocytes was found in severe patients. According to the study findings, altered lymphocyte and monocyte subsets can be considered prognostic factors for severe COVID-19. The association between immune cells and disease severity should be considered data in therapeutic options of COVID-19.
Footnotes
Authors' Contributions
S.K. conceived the idea of the study and coordinated the data collection. G.Y. and F.M.Y. performed flow cytometric analyses, statistical analyses, and interpretation of the results. G.Y. and S.K. contributed to literature search, discussing the results, and writing the article. A.B., F.M.Y., and H.B. helped in drafting and revising the article. C.B., B.O.O., and A.S. participated in data collection and analysis. All authors have read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.