
Abstract
The ability to detect antibodies to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is currently under investigation with various performance characteristics and indications for use. In this article, we analyzed the ability of the Abbott SARS-CoV-2 immunoglobulin class G (IgG), EuroImmun SARS-CoV-2 enzyme-linked immunosorbent assay (ELISA) IgG, and EuroImmun SARS-CoV-2 ELISA immunoglobulin class A (IgA) kits to detect evidence of previous infection with SARS-CoV-2. We tested 49 known coronavirus disease-19 (COVID-19) patients and 111 prepandemic stored serology specimens. This resulted in a sensitivity of 95.9%, 100.0%, and 91.3% and a specificity of 98.2%, 98.2%, and 90.8% respectively, using manufacturer recommended cutoffs after inconclusive results (one for EuroImmun IgG and five for EuroImmun IgA) being excluded in the final statistical analyses. Cross-reactivity of hepatitis C virus seropositive specimens was observed resulting in false positives (p < 0.05). If a two-tiered algorithmic approach was applied, that is, testing with Abbott SARS-CoV-2 assay followed by EuroImmun SARS-CoV-2 IgG, 100% specificity and sensitivity could be obtained after six inconclusive results were excluded from data set before statistical analyses. Performance characteristics presented demonstrate the superior performance of IgG class antibodies for investigating previous infections. In addition, utilizing a second antibody test for supplementary testing may significantly enhance performance, particularly in lower prevalence settings.
Introduction
Since the emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus responsible for coronavirus disease-19 (COVID-19), at the end of 2019, there are ∼39 million cases and nearly 1.1 million deaths worldwide, as of October 16, 2020 (23). To stop the spread of infection, manage patients, and provide timely information to public health policy makers, accurate, timely, and accessible diagnosis of SARS-CoV-2 infection is required (17,24).
At this time, the primary focus of SARS-CoV-2 testing in Canada, and in the province of Newfoundland and Labrador, has been on molecular methods using real-time reverse transcription–polymerase chain reaction (RT-qPCR) to detect SARS-CoV-2 RNA. The limitation of these molecular tests is that they can only indicate the presence of viral RNA in the particular sample; they cannot indicate the presence of viable viral particles. The absence of the viral RNA cannot determine if a person was infected and has since recovered or if the person is infected but the virus was undetectable from that source at that time (17,22). Often, RT-qPCR tests are performed on those patients who are symptomatic or those who are epidemiologically linked to COVID-19 cases, an approach that likely underestimates the true prevalence of infection in the population (9). In addition, RT-qPCR methods also face challenges with accessibility of reagents and equipment, availability of trained personnel, cost, and challenges with performance (13,25).
Because of these limitations, developments in serological testing are underway to better quantify the number of cases of COVID-19 (5,17). In addition, antibody detection may provide a complementary perspective, along with RT-qPCR testing, in the diagnosis of COVID-19 (24,25). At this time, it has yet to be established whether there is a long-term immune response against SARS-CoV-2 (12) or protection against reinfection (17).
ELISA and chemiluminescent microparticle immunoassay (CMIA) provide semiquantitative in vitro measurement of the levels of human antibodies of the immunoglobulin class A (IgA) and G (IgG) against SARS-CoV-2 in serum. To evaluate the serological tests' ability to detect previous infection with SARS-CoV-2, serum from laboratory-confirmed COVID-19 cases were used as the known positive specimen group and stored historic prepandemic serum specimens served as a negative comparator group.
In an effort to provide comprehensive public health and microbiological services during the SARS-CoV-2 global pandemic, assessment was performed for three tests: Abbott Architect SARS-CoV-2 IgG (A-IgG), EuroImmun Anti-SARS-CoV-2 ELISA IgG (EI-IgG), and EuroImmun Anti-SARS-CoV-2 ELISA IgA (EI-IgA). These assays were selected as our laboratory has Abbott Architect and EuroImmun platforms for the standard catalog of public health serological tests.
Materials and Methods
Ethics
This research was performed in consultation with the Health Research Ethics Board (HREB) St. John's, Newfoundland Island, and was deemed to be a quality assurance project, therefore ethics approval was not required. However, given that additional sampling of patients was needed, a written consent process was implemented to obtain serological specimens from confirmed, previously infected COVID-19 patients.
Sample size
To assess the new serological tests, 111 negative comparators, prepandemic specimens were withdrawn from local archives. These were selected in two ways: 50 specimens were selected in a random manner and 61 specimens were selected that were known to be positive for various non-SARS-CoV-2 reactive antibodies. The specimens that made up the randomly selected negative control group were matched to the same time period in the previous year, March–June 2019. Through partnership with the local Medical Officer of Health, confirmed RT-qPCR-positive patients were identified with strong epidemiological links, and 49 specimens were collected to serve as our known positive specimen group.
Specimen collection
For specimen collection from COVID-19 patients confirmed by RT-qPCR and quantified as previously published (11), frontline clinicians obtained written consent at local acute care facilities, collected two blood samples using serum separator tubes, and forwarded to the Newfoundland and Labrador Public Health Microbiology Laboratory (PHML). Patient name and health care number were provided to match clinical history based on institutional policies.
SARS-CoV-2 RT-qPCR viral load testing
Molecular testing was performed at the PHML using previously published primers and probes by Corman et al. for E gene (6,18). A quantitative standard of in vitro transcribed RNA (it-RNA) was developed by performing in vitro transcription using TrancriptAid T7 High Yield Transcription kit (Thermo Scientific), on an amplified gBlock (Integrated DNA Technologies). The it-RNA was extracted using MasterPure Complete DNA and RNA Purification kit (Lucigen) to remove all contaminates including template DNA. The it-RNA was then quantitated with QuantiFlour RNA System (Promega) to determine the copies per microliter. All RT-qPCR patient samples were extracted on either the QiaSymphony (Qiagen) or MagNA Pure Compact (Roche), extracting an initial volume of 200 μL and eluting to either 60 or 50 μL, respectively; all runs included a negative process control. RT-qPCR was performed with using Luna Universal Probe One-Step RT-qPCR Kit (New England Biolabs, Inc.) on the Lightcycler 480 II (Roche). A master mix was created with 400 nM of each primer and 200 nM of the probe, with 15 μL added to 5 μL of sample extract. One-Step RT-qPCR was performed with 15 min at 50°C, then 1 min at 95°C, 45 cycles of two-step qPCR with 95°C for 5 and 30 sec at 58°C. A quantitated positive control at 60 copies per reaction was included on all runs with a stored standard curve applied to each positive specimen.
EI Anti-SARS-CoV-2 (IgG and IgA)
The EI 2606-9601 G (IgG) is an ELISA that provides semiquantitative in vitro detection of IgG human antibodies against the S1 domain of the spike protein including the immunologically relevant receptor binding domain of SARS-CoV-2 in serum or plasma (8), whereas EI 2606-9601 A (IgA) is an ELISA that provides semiquantitative in vitro determination of IgA human antibodies against S1 domain of the spike protein of SARS-CoV-2 in serum or plasma (7). Health Canada has approved EI-IgG assay but has not yet approved the EI-IgA currently. For every group of tests performed, calibrator, positive, and negative control are run and must fall within the limits stated for the relevant test kit lot, as per manufacturer's directions.
Abbott (A) SARS-CoV-2 IgG assay
The SARS-CoV-2 IgG assay is a CMIA, which provides qualitative detection of IgG antibodies to SARS-CoV-2 in serum and plasma; IgG antibodies to the nucleocapsid proteins are detected in this methodology (1). This is a Health Canada approved test and, in addition, a comprehensive evaluation has been performed by Public Health England (19). For all tests performed, calibrations, positive, and negative controls were run per manufacturer's directions and fell within in the limits stated as per manufacturer directions.
Non-SARS-CoV-2 serology assays
For the 61 selected specimens that were known to be positive for various non-SARS-CoV-2-reactive antibodies, all serological testing was performed at the PHML using the Abbott Architect i2000 and i1000 systems and the EuroImmun Analyzer I to detect antibodies. For the purposes of this study, Architect i1000SR was used for the detection of human cytomegalovirus (HCMV) IgG. Architect i2000SR was used for the qualitative detection of hepatitis C virus (HCV) IgG/IgM, HCMV IgM, rubella virus IgG, Epstein–Barr virus (EBV), EBV nuclear antigen (EBNA) IgG, EBV viral capsid antigen (VCA) IgM, hepatitis A virus IgM, human immunodeficiency virus 1 (HIV-1) IgG, and Syphilis Treponema pallidum (TP) IgG/IgM. The EuroImmun Analyzer I is a platform for semiquantitative detection of varicella zoster virus (VZV) IgG and herpes simplex virus 1/2 IgG.
Statistical analysis
Statistical analysis was performed using Excel, Microsoft Office Professional Plus, 2013 and MedCalc Diagnostic Test Evaluation Calculator. Contingency tables were used to determine test positivity rates and the diagnostic sensitivity and specificity of each serological test. Confidence intervals for sensitivity and specificity are “exact” Clopper–Pearson confidence intervals. Differences in positive predictive values (PPVs) and negative predictive values (NPVs) were also calculated based on varying levels of prevalence for comparison of test performance. The t-test was used to determine the significance in our cross-reactivity analysis by comparing the A-IgG values for the HCV seropositive specimens and the HCV seronegative specimens. Precision and analytical sensitivity and specificity were also assessed to determine intraoperator reliability, relative lower limit of detection (LLOD), and possible cross-reactivity, respectively.
Results
For this study we had 160 patient specimens in total; 49 of which were SARS-CoV-2-positive RT-qPCR confirmed cases and 111 were historic serological specimens collected before the emergence of SARS-CoV-2. Of the 49 COVID-19 cases, 24 (49.0%) were women and 25 (51.0%) were men; the average age was 55 years with a minimum of 18 years and maximum of 81 years (median 57 years of age). Of the 111 historic serological specimens, 72 (64.9%) were women and 39 (35.1%) were men. The average age for these historic specimens was 44 years of age with a minimum of 11 and a maximum of 83 years (median 42 years of age). Viral load at time of diagnosis was found to be an average of 2.0 × 106 (1.3 × 103–6.5 × 108) copies/mL at 5 (−5 to 14) days postsymptom onset, with two patients being asymptomatic. Patients diagnosed before symptoms onset were known contacts of other symptomatic cases and are represented with negative days to onset.
Figures 1 and 2 illustrates days from symptom onset in comparison with viral load and A-IgG index values, EI-IgG and EI-IgA ratio values, respectively. Figure 1 results are in line with the literature and help to demonstrate the importance of early testing for SARS-CoV-2, as viral shedding decreases over time (20). For the positive SARS-CoV-2 RT-qPCR-confirmed cases, there was a median of 60 days from symptom onset to collection of serum specimen (min = 38, max = 67). For the 111 negative sample set, a panel of 61 specimens with previous non-SARS-CoV-2 antibody positivity was selected. These included 10 HCMV IgG, 9 HCV IgG/IgM, 5 HCMV IgM, 5 rubella virus IgG, 5 VZV IgG, 3 EBV EBNA IgG, 2 EBV VCA IgM, 3 hepatitis A virus IgM, 4 herpes simplex virus 1/2 IgG, 5 HIV-1 IgG, 4 Syphilis TP IgG/IgM, 6 samples positive for various hepatitis B viral markers. Precision assessments of the assays were performed with positive and negative controls performed 10 times within 1 day and on 10 different days; both intrarun and interrun coefficients of variation were <10% for all assays.
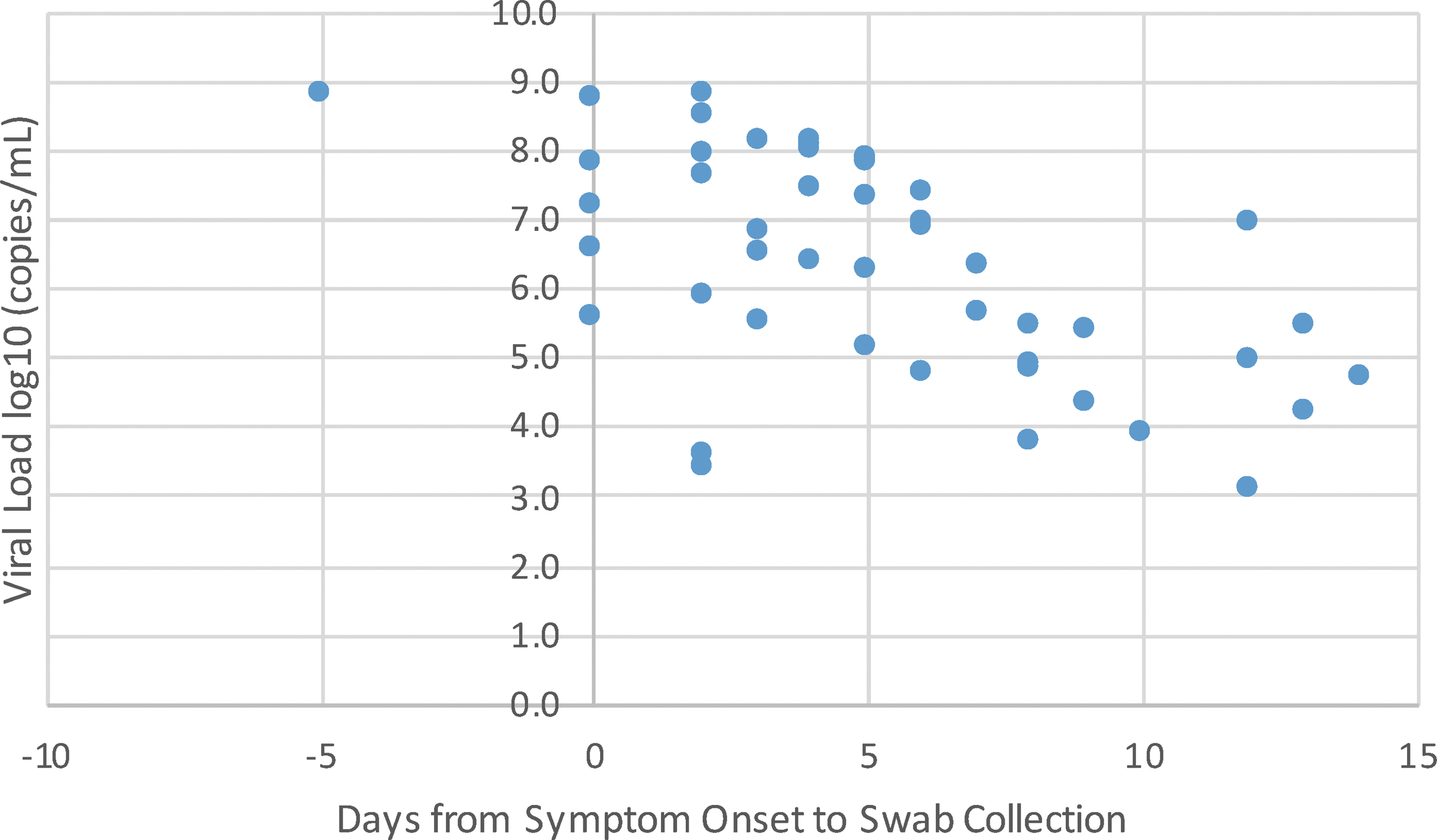
Days from onset versus viral load (n = 47*). *Two positive COVID-19 specimens did not have date of symptom onset.
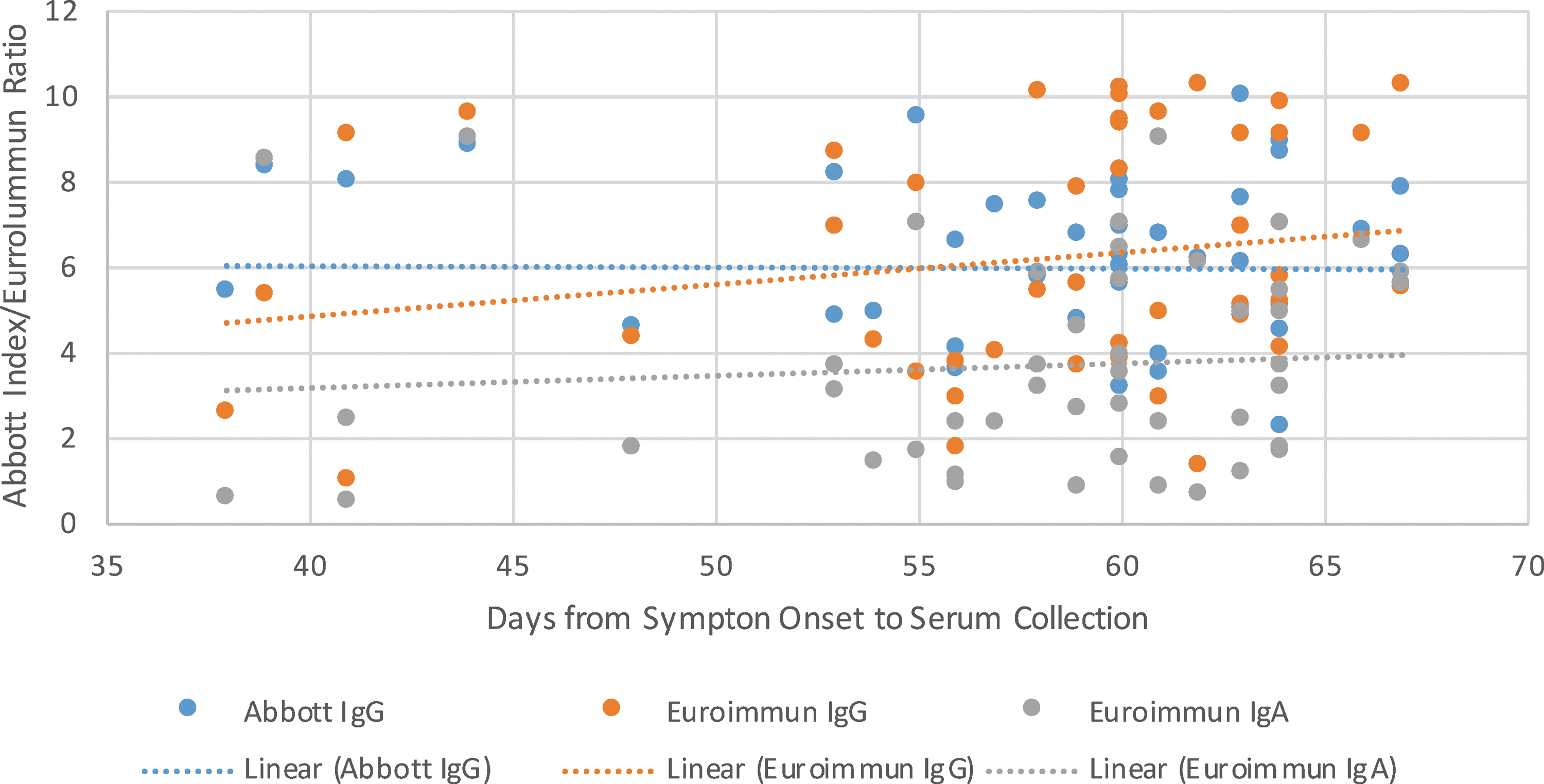
Days from onset versus Abbott IgG index values and EuroImmun IgG and IgA ratio values (n = 47*). *Two positive COVID-19 specimens did not have date of symptom onset. IgA, immunoglobulin class A; IgG, immunoglobulin class G.
The sensitivity of all three assays was assessed with specimens from positive SARS-CoV-2 RT-qPCR cases and analytically with a dilution panel of pooled positive samples. The positive clinical specimens demonstrated sensitivities of A-IgG, EI-IgG, and EI-IgA were 95.9%, 100.0%, and 91.3%, respectively, as presented in Table 1 when calculations were performed by not including the inconclusive results. Further calculations were performed with alternative interpretations of the inconclusive results (shown in Table 1). The two samples that were falsely negative for A-IgG produced index values of 0.99 and 1.28, demonstrating a lower titer of antibody that did not meet the manufacturer established cutoff of 1.4. The EI-IgG assay produced one sample that was inconclusive, which was the same sample that produced the lower false negative using the A-IgG assay. The EI-IgA assay produced four false-negative results that did not always correlate with the IgG titer of either assay or days from symptom onset to serum collection. Analytical sensitivity, also referred to as LLOD, was performed by pooling known positives and then diluting them as per Table 2, and this is an average relative determination. The limit of detection was found at the 1:16 dilution for A-IgG assay and 1:4 for both the EuroImmun assays. Overall, clinical sensitivity was found to be slightly higher for the EI-IgG assay, with the A-IgG assay being more analytically sensitive.
Diagnostic Performance of EuroImmun IgG/IgA and Abbott IgG
Inconclusive, not included in calculations.
Confirmed positive = positive by both tests.
Confirmed negative = negative by both tests.
Calculated with inconclusives not counted.
Calculated with inconclusives counted as positive results.
Counted with inconclusives counted as negative results.
IgA, immunoglobulin class A; IgG, immunoglobulin class G; PCR, polymerase chain reaction.
Analytical Sensitivity with Limits of Detection
The specificity of all three assays was measured by testing 111 prepandemic clinical specimens composed of two groups, 50 random samples and 61 samples known to be positive for non-SARS-CoV-2-reactive antibodies. For the A-IgG assay, there were two false-positive results on two HCV IgG/IgM-positive samples. In addition, the next highest index value, 0.49, of the negative sample set, was also from an HCV-positive patient. The EI-IgG assay produced one false-positive result against HCMV IgM and one false-positive result against a sample with anti-EBV/VZV IgG antibodies. The EI-IgA assay was positive for 10 different patients including samples from both randomly pulled samples and specimens positive for various non-SARS-CoV-2-reactive viral antibodies. The A-IgG and the EI-IgG assay were not falsely positive on the same samples. Overall, the A-IgG, EI-IgG and EI-IgA assays produce clinical specificity of 98.2%, 98.2%, and 90.8%, respectively.
Discussion
Detection of anti-SARS-CoV-2 antibodies will influence medical, public health, and societal decisions in the coming months and years as a result of the COVID-19 pandemic. Presented here is an initial evaluation of two classes of antibodies, from two different commercial providers, EuroImmun and Abbott. The assays detect separate antigenic targets with potential different implications on clinical performance (13), and potential protective implications. Our results present slightly lower performance than the package insert for Abbott Architect assay and slightly better than the EuroImmun assays (1,7,8). IgG antibody test showed superior sensitivity and specificity over IgA antibody test in our study. IgM antibody test for SARS-CoV-2 was not evaluated in this study, IgM (14,15) tests by themselves are less sensitive and specific than IgG results, however, may improve diagnostic sensitivity slightly when performed in tandem with IgG testing. In addition, the performance of the Abbott IgG assay in our setting showed a higher sensitivity and a lower specificity than a comprehensive evaluation of over 1,000 specimens conducted by the Clinical Service Unit at Public Health England Colindale (19). From a US study (n = 1,020) we found similar specificity, although slightly inferior sensitivity, for the performance of the A-IgG assay (4,17), demonstrating consistency with the manufacturer reported performance. Ultimately, there were no significant differences between both the IgG assays, which was also found in work completed in the United States (21).
Our sample subset likely impacted performance factors for two main reasons. First, our known positive samples were collected from mildly symptomatic patients that were managed in the community by the Communicable Disease Control team. There were two discordant results from our positive sample set for IgG antibodies. One sample collected 41 days postsymptom onset was negative on A-IgG and inconclusive on EI-IgG; and the other sample, which was collected 62 days postsymptom onset, was negative on the A-IgG and positive on the EI-IgG. As demonstrated in Table 3, there was no significant correlation between days of symptom onset to collection of serum and antibody index/ratio to suggest waning of antibodies during the time period tested. This information is in contrast to a study in Wuhan, China that found 10% of patients lost SARS-CoV-2 antibodies within weeks of infection (12), although different serology tests were used in this case. However, it has been previously shown that more severe disease produces a stronger antibody response, and thus our mild disease cohort may result in a lower sensitivity (26). Second, our negative sample subset was made up of two categories of randomized retrospective samples and a cross-reactivity panel of specimens with known antibody status for various non-SARS-CoV-2 pathogens. All discordant IgG and 8 of 11 of the IgA samples from presumed negative samples were from patients with known non-SARS-CoV-2-reactive viral antibodies.
Pearson R Relationships Between Age, Study Time Frames, Polymerase Chain Reaction Viral Loads, A-IgG, EI-IgG, and EI-IgA (n = 49)
A-IgG, Abbott Architect SARS-CoV-2 IgG; EI-IgA, EuroImmun Anti-SARS-CoV-2 ELISA IgA; EI-IgG, EuroImmun Anti-SARS-CoV-2 ELISA IgG; ELISA, enzyme-linked immunosorbent assay; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Given the ubiquitous nature of coronaviruses in general, there is a rightful concern of cross-reactivity in the development of serological testing methodologies (9). In the package insert, EuroImmun reported cross-reactions to other human pathogenic coronaviruses; however, no other viruses were mentioned (7,8). However, in the Abbott IgG documentation, it states that there is no-cross reactivity observed in a non-COVID-19 population for coronaviruses and only 1 case of 181 (0.6%) showed cross-reactivity with HCMV IgG (1). As this was an anticipated challenge for investigating these new tests, we selected a cross-reactivity panel of specimens with known immune status for various pathogens.
One limitation in our setting is that we do not test for non-SARS-CoV-2 human pathogenic coronaviruses by serology and chose to focus on other pathogens. Overall, anti-SARS-CoV-2 antibodies may cross-react with certain pathogens or under some medical conditions. It was interesting to note that in other studies, and in the manufacturer information, this type of cross-reactivity was not identified (7,16). That being said, in Matushek et al. (16) work they focused on other respiratory coronavirus cross-activity. Seropositive HCV samples were found to cross-react with the A-IgG assay in this validation significantly (p < 0.05) in comparison with the non-HCV-infected persons. Additional studies are required to fully evaluate the potential issues with cross-reactivity and the impact it may have on the seroprevalence investigations for SARS-CoV-2.
Given these limitations, current recommendations for lower prevalence area like Newfoundland and Labrador are to proceed with two-tiered testing (5). In our Table 1, sensitivity and specificity is shown for a two-tiered testing algorithm, where EI-IgG was applied as a supplementary test to all A-IgG results of index value ≥0.7. Tests were still interpreted per manufacturer instructions however; if EI-IgG was indicated per testing algorithm and produced different qualitative results from A-IgG, this was deemed to be inconclusive. This cutoff was developed by observing the lowest index value from a known COVID-19 case, 0.99 and the highest index value from a true negative result in our negative sample set, 0.49, applying the average rounded to the nearest tenth. In Newfoundland and Labrador, the confirmed case prevalence by RT-qPCR is ∼0.05%, whereas some studies have suggested that actual prevalence rates may be underrepresented by RT-qPCR by as much as 55-fold (3).
In Table 4, PPVs and NPVs are calculated based on both the confirmed prevalence and the largest estimate from published literature. Given the low prevalence in our province, even small drops in specificity can make very significant changes in the PPV. In addition, in Figure 3, we compared variances in prevalence and the impact on the PPV values for A-IgG, EI-IgG, and a two-tiered model. In both A-IgG and EI-IgG, a PPV of 95.0% is not reached until the overall prevalence is ∼25.0%. Based on the low prevalence in our province, a two-tiered model would maximize PPV and performance.
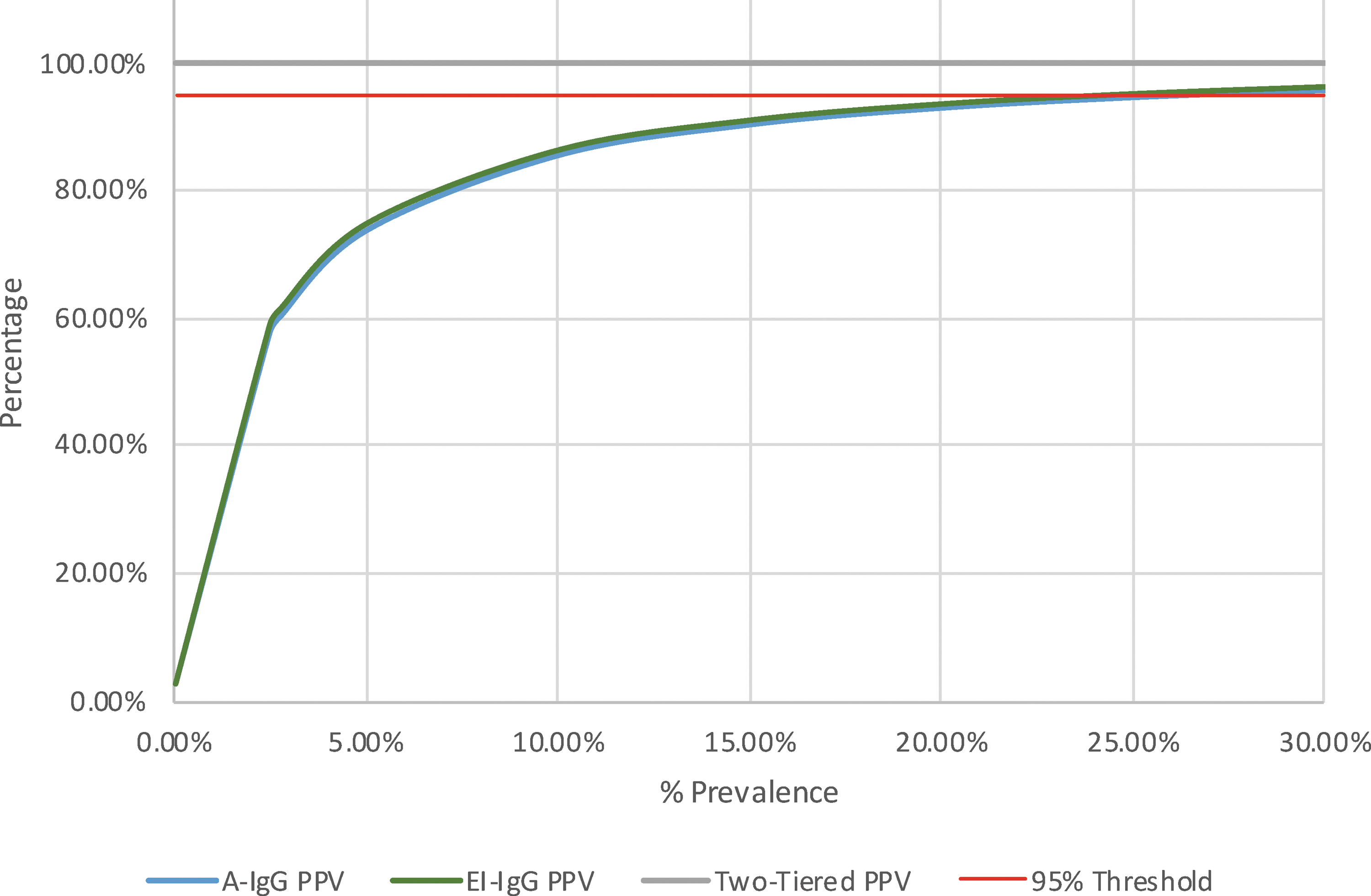
Impact of prevalence on PPV for IgG tests, independently and in a two-tiered model*. *A-IgG and EI-IgG PPV lines overlap in many places and may be difficult to discern. A-IgG, Abbott Architect SARS-CoV-2 IgG; EI-IgG, EuroImmun Anti-SARS-CoV-2 ELISA IgG; PPV, positive predictive value; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Impact of Prevalence on Positive Predictive Value and Negative Predictive Value for IgG Tests, Independently and in a Two-Tiered Model
NPV, negative predictive value; PPV, positive predictive value.
No additional clinical information, such as antibodies to seasonal coronavirus, respiratory distress, oxygen saturation, or radiological findings were investigated in our study. This is a potential limitation and additional clinical perspective may provide some insight into the clinical progression and manifestation of disease in patients as included in other works (10,24).
Serological specimens from COVID-19 cases were collected on average 52.7 days from the RT-qPCR results. Ideally, blood is collected at different phases of infection as clinically feasible to help understand the dynamic of the antibody production (24) and the differing performance of the assays based on time after diagnosis (10); at this time, we were unable to obtain specimens corresponding to disease severity. This is a limitation and certainly an opportunity for further future investigation.
When we analyzed viral load at the time of initial diagnosis, it did not correlate with antibody response. However, viral load negatively correlated with days from symptom onset; this added assurance to our symptom onset date, which in mild disease can be ambiguous. This reduction of viral load over the length of illness is in line with discussions regarding specimen suitability (2,14,22).
In our study population, age positively correlated with strength of antibody response. This may be owing to more severe disease in older population; however, additional investigation is necessary. Previous work in this area has shown a correlation with severity and antibody response (26).
Conclusion
Serological testing may serve a critical role in truly quantifying the number of COVID-19 cases. The EI-IgG and A-IgG assays may also serve as an effective tool in helping detect past SARS-CoV-2 infection, independently or in concert with other diagnostic modalities. However, given the high cross-reactivity found in EI-IgA there may be limited utility in the use of this immunoglobulin class for detection of previous infection. Cross-reactivity in HCV seropositive specimens was a unique observation that resulted in false positives. Additional studies would add to the strength of this evidence and help to better establish the relationship between severity of illness and antibody response.
Footnotes
Authors' Contributions
R.N. and L.G.: investigation, writing—original draft, review and editing, conceptualization, data curation, formal analysis, resources, investigation; L.J.: investigation, writing—original draft, review and editing, conceptualization, methodology, data curation, formal analysis, validation, supervision, resources, investigation, project administration; H.D.K and S.H.: writing—review and editing, validation, supervision; C.D., R.R. and P.W.: writing—review and editing, resources, investigation; G.Z. and Y.Y.: writing—review and editing, validation, investigation.
Acknowledgments
The authors thank the technologists at the Newfoundland and Labrador PHML for assisting with this quality improvement and development project, especially Cathy Lang, and Amy Buckle. Special thanks for those who helped coordinate patient specimens especially the Eastern Health Communicable Disease Control program, including Suzette Spurrell, Andrea Doyle, Anita Forward, Cindy Saunders, Colleen Kearley, Jennifer Slade, Josephine St. Croix, Joy Loveys, Lesley Ranson, Lynette Penney, Sherri Hopkins, Shianne Combden, Shelley Goulding, Andrea Morrissey, Cynthia LeRoux, Kimberley Finn, Ashley Hayward, and Jackie Jackman, as well as Peter Daley, Infectious Diseases.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. It was conducted as part of ongoing quality improvement and development. Abbott Diagnostics provided kits to assist in the validation and verification.