
Abstract
The CC5 and CXC3 chemokines (CK) pathways are involved in the pathogenesis and outcome of several disease states, including chronic hepatitis C (CHC). The kinetics of Regulated upon Activation Normal T cell Expressed and Secreted (RANTES) (CCL5) and IP-10 (CXCL10) during direct-acting antivirals (DAA) treatment was retrospectively analyzed in 18 liver transplant recipients (LT-R) compared with 20 patients with CHC and 49 healthy controls (HC). CK levels were determined at baseline, week 4, end of treatment, 24 weeks post-treatment (sustained virological response [SVR]), and later-on during follow-up (FU), 12 and 24 months post-DAA. At baseline, median RANTES levels were higher in HC than in both LT-R (p > 0.01) and CHC (p > 0.01), whereas IP-10 levels were higher in LT-R and CHC than in HC (p > 0.05 and p = 0.01), respectively. Mean RANTES values increased during DAA therapy to peak at SVR and FU with significantly higher levels than at baseline in LT-R (p < 0.01) and in CHC, but only at FU (p < 0.003). A subsequent return to baseline or lower levels was observed at extended FU. On the contrary, IP-10 values showed a significant decrease from baseline to SVR and FU in both LT-R (p < 0.03) and CHC (p < 0.01). RANTES profiles during the first 4 weeks of DAA treatment showed an increase or decrease from baseline according to baseline RANTES levels. CCR5 genotyping in LT-R showed the presence of 1 homozygous Δ32/Δ32 and 2 heterozygous WT/Δ32 haplotypes with a prevalence of 5.5% and 11.1%, respectively.
In conclusion, although IP-10 showed the expected kinetics, the CC5 pathway appears extensively altered during CHC infection: monitoring these patients may be indicated as they may be at risk of other infections or immune-mediated disorders.
Introduction
Chemokines (CK) are key mediators of cellular immune response and their interactions with specific cognate receptors induce recruitment and activation of different lymphocytes subpopulation at the site of the lesion (3,10,20,32). The main inflammatory CK, including Macrophage Inflammatory Protein (MIP)-1a, MIP-1b and Regulated upon Activation Normal T cell Expressed and Secreted (RANTES) or C-C chemokine ligand 5 (CCL5), bind the C-C chemokine receptor type 5 (CCR5) and have been found to regulate the trafficking of immune cells into the liver. CCR5-activated hepatic stellate cells may acquire a myofibroblastic phenotype with an increase in matrix deposition and progressive fibrosis (2,29,30,36). During hepatitis C virus (HCV) chronic infection, virus persistence may be favored by a reduced migration of antigen-specific cytotoxic T lymphocytes into the liver through impairment of CCR5 receptor expression (18,29). Indeed, it has been shown that various HCV proteins, mainly core, act on CCL5 expression by inhibiting its promoter (1). This could affect the induction of an effective Th1 response mediated by CCR5/CCL5 interactions and considered key for the control of viral replication through HCV-specific cytotoxicity. In this respect, as in the case of HIV infection, where CCR5 acts as the virus cellular co-receptor and CCR5 antagonists have already been used in clinical practice, the modulation of the CCR5/CCL5 pathway might be a potential therapeutic strategy (4,6,27).
In addition, also IP-10 (Interferon-induced Protein 10, CXCL10) and its CXCR3 receptor are active in recruitment of monocytes, macrophages, T lymphocytes, natural killer cells, and dendritic cells to the site of the lesion (16,24). During chronic HCV infection, the CXC3 and CCR5 receptor/ligands systems play a major role in eliciting the adaptive immune response, through the activation of specific cytotoxic CD8 and regulatory helper CD4 cells. The CXC3 IP-10 is key in controlling HCV replication in acute infection and in influencing disease progression in chronic infection (8,22). Indeed, several studies showed elevated plasma IP-10 levels after HCV infection as expression of activation of innate immunity (7,31,33) and in association with spontaneous or interferon-induced HCV clearance (5,37). Increased plasma IP-10 levels (15,26,28) and upregulated intrahepatic IP-10 expression (12) appear to be associated with greater grade and/or stage in HCV-related chronic hepatitis. Moreover, plasma IP-10 levels at the time of liver biopsy may help predicting the development of fibrosis (38).
Since these molecules indicate the rapid fall of viral load during PEG-interferon therapy, it would be interesting to evaluate their dynamics during direct-acting antivirals (DAA) treatment that induce even more rapid viral suppression (17).
No data are currently available on CK pattern during DAA treatment in liver transplant recipients (LT-R) with recurrent HCV who are under immunosuppressive therapy.
In this study, we investigate the pattern of circulating CCL5 (RANTES) as well as CXCL10 (IP 10) ligand and the occurrence of the CCR5 Δ32 deletion in LT-R with recurrent HCV before, during and after DAA treatment. We compared them with immunocompetent patients with chronic hepatitis C (CHC) to gain insight into the resetting of the immune response after a DAA-induced rapid virus elimination. Healthy blood donors (healthy controls [HC]) served as controls.
In both patients' groups, we correlated the CK findings with post-treatment outcome, in terms of virological response, fibrosis, or inflammatory changes at histology and/or by noninvasive techniques.
Materials and Methods
This is a retrospective single-center study (conducted at the Gastroenterology and Hepatology Division, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico in Milan, Italy) including 18 HCV LT-R who received DAA therapy between 2015 and 2016 for histologically proven post-transplant recurrent HCV (34). Stored serial serum samples and whole blood samples were available at the following time point: before treatment, on-treatment at week 4, at the end of treatment (EOT), 24 weeks post-treatment (sustained virological response [SVR]), and later on during follow-up (FU) between 12 and 24 months from starting DAA.
A group of 20 immunocompetent patients with CHC, successfully treated with DAA and a group of 49 matched healthy blood donors (HC) served as controls. In HCV LT-R a liver biopsy was scheduled at baseline before starting antiviral treatment in association with liver stiffness measurement by Fibroscan® (Echosense, Paris, Fr). A liver biopsy was repeated also during or after treatment only in case of persistent or new appearance of abnormal liver functions tests and/or increased liver stiffness. This to exclude cellular rejection, de novo autoimmune hepatitis or other causes of concomitant liver graft dysfunction (35).
Liver histology and immunohistochemistry
Liver tissue sections were routinely processed and stained with hematoxylin-eosin and Masson's Trichrome staining. Fibrosis stage and activity were histologically scored according to Ishak (21).
Patients gave their informed consent to data handling and samples use. The Institutional Review Board approved the study, which conforms to the Good Clinical Practice Guidelines and principles of the Declaration of Helsinki.
CCL5-RANTES and CXCL10-IP 10 determination
The amount of circulating RANTES and IP 10 was assessed on serum at each time point using specific enzyme-linked immunosorbent assay (ELISA) (Human CCL5/RANTES Quantikine ELISA Kit, Human CXCL10/IP-10 Quantikine ELISA Kit, R&D System).
CCR5 genotyping
Genomic DNA was extracted from whole blood using the extraction kit from QIAGEN (Hilden, Germany). Evaluation of the CCR5Δ32 haplotype was performed by PCR with specific primers (Fw 5′-CTTCATTACACCTGCAGCTCTCA-3′ and Rv 5′-CGAGTAGCAGATGACCATGACA-3′) and PCR products were separated by standard electrophoresis on 2% agarose gels containing ethidium bromide (11).
Statistical analysis
Statistical analyses were conducted using the Mann–Whitney U test or the Student's t-test for continuous variables and the χ 2 or Fisher's exact probability test for categorical data. A probability value of p < 0.05 was considered statistically significant.
Results
Overall, 18 HCV LT-R, 20 CHC, and 49 HC were included in the study, as previously described.
Epidemiological, histological, virological, and clinical features are reported in Table 1. Most of the patients were males (63%) with a median age of 61 years, infected with genotype 1 or 2. Fourteen patients were failures to previous IFN-therapy. Epidemiological and clinical features of the LT-R and CHC cohort were similar. An SVR was achieved by 33 (87%) patients, overall.
Patients Baseline Characteristics
Results are reported as number (percentage) or median (range).
ALT, alanine amino transferase; AST, alanine aspartate transferase; CHC, chronic hepatitis C; CyA, cyclosporine; DAA, direct-acting antivirals; de novo AIH, de novo autoimmune hepatitis; FCH, fibrosing cholestatic hepatitis; G/P, Glecaprevir/Pibrentasvir; HCV, hepatitis C virus; HCV rec-Hep, HCV recurrent hepatitis; LDV, ledipasvir; LT-R, liver transplant recipients; MMF, mycophenolate mofetil; RBV, ribavirin; SOF, sofosbuvir; TACRO, tacrolimus; VEL, velpatasvir.
Median time from LT to effective DAA treatment was 10 years (1–18 years). Immunosuppression was calcineurin inhibitors (CNI) based in all cases. A severe HCV recurrence in three recipients with histologically proven cirrhosis and one with fibrosing cholestatic hepatitis (FCH) were observed. Three patients had features of plasmacellular recurrent HCV, a combination of viral and autoimmune factors. None of the patients presented with relevant comorbidities. One LT-R patient experienced a relapse to a treatment administered before liver transplantation.
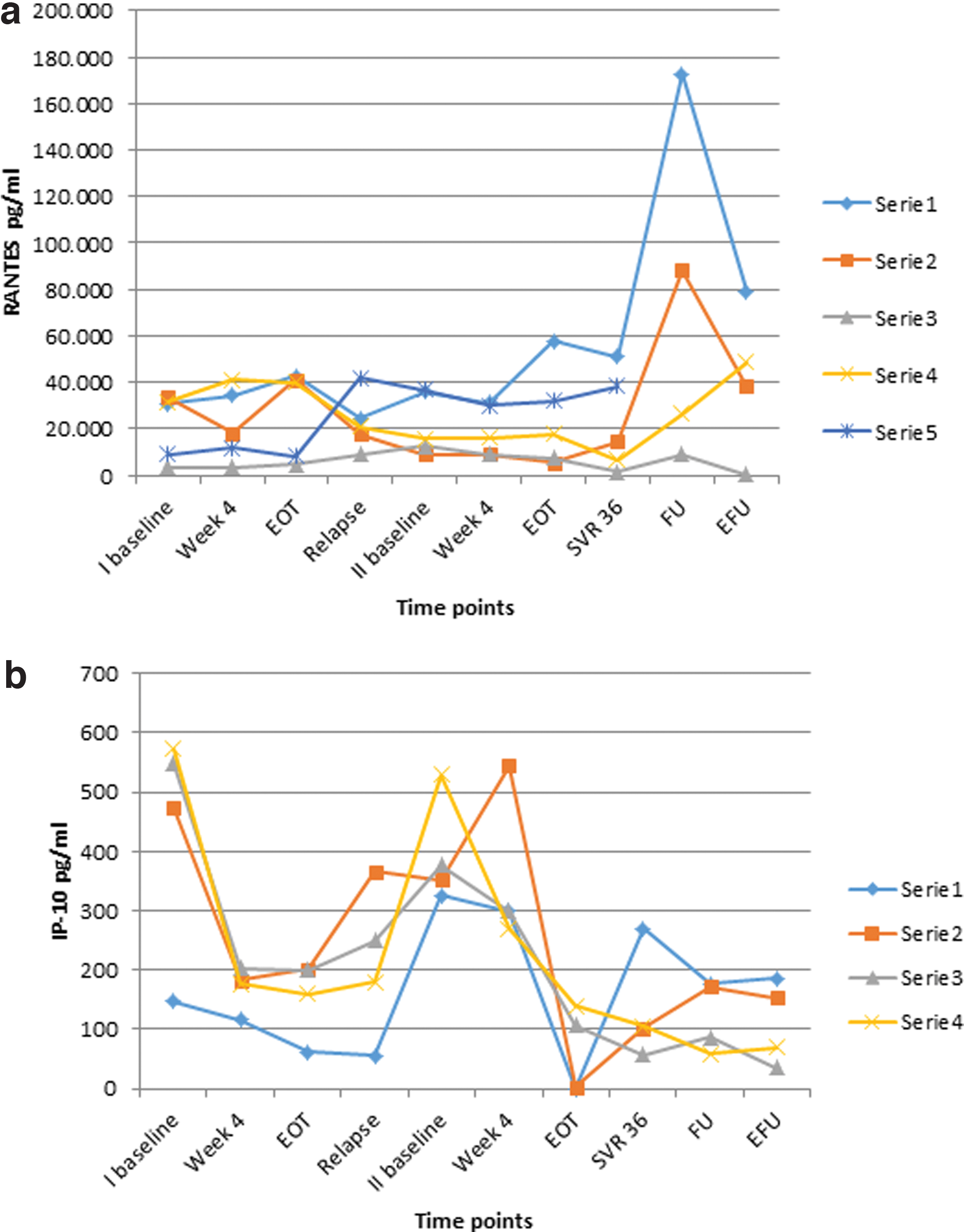
At baseline, median RANTES level was higher in HC than in both LT-R (68,698 pg/mL vs. 22,634 pg/mL, p > 0.001) and CHC (68,698 pg/mL vs. 38,432 pg/mL, p > 0.01) (Fig. 1). As described in Figures 2a and b, RANTES showed in most patients slightly fluctuating levels with isolated spikes observed at the EOT with levels two- to threefold higher than at baseline and week 4. Twenty-four weeks post-treatment, after achievement of SVR, median RANTES levels were similar in LT-R and CHC, 36,569 pg/mL (11,460–60,800 pg/mL) and 49,463 pg/mL (19,670–80,410 pg/mL), respectively. However, mean RANTES values were significantly higher at the SVR time point than at baseline in LT-R patients (36,569 pg/mL vs. 22,634 pg/mL, p < 0.01) but not in CHC (48,701 pg/mL vs. 38,432 pg/mL, p < 0.93) (Fig. 3). Thereafter, RANTES levels increased again with spikes at the first FU (6–12 months after SVR) reaching concentrations two- to fivefold higher than at previous time points. This pattern was observed both in LT-R and CHC patients with values during FU significantly higher than at baseline, 117,420 pg/mL vs. 22,634 pg/mL, p < 0.003 and 190,040 pg/mL vs. 48,701 pg/mL, p < 0.01, respectively (Fig. 3). A subsequent return to early on-treatment time point levels was observed in 8 LT-R patients (61%) further analyzed at extended FU, at least 24 months post-SVR (Figs. 2a, b, and 3). As opposed to RANTES, baseline IP-10 levels were higher in both LT-R (211 pg/mL vs. 112 pg/mL, p < 0.05) and CHC (305 pg/mL vs. 112 pg/mL, p < 0.01) than in HC (112 pg/mL) (Fig. 4). The dynamic profile of IP-10 values showed a significant decrease from baseline to SVR in both LT-R (211 pg/mL vs. 124 pg/mL, p < 0.03) and CHC patients (305 pg/mL vs. 161 pg/mL, p < 0.01) a trend confirmed also at FU time points in the majority of patients (Figs. 5a, b, and 6). Although this pattern was consistent among all CHC patients, it showed more heterogeneous profiles in patients with LT-R with fluctuating IP-10 levels during treatment. Interestingly, two different CK profiles were observed in LT-R patients during the first weeks of treatment, with an increase or decrease from baseline to week 4. The pattern characterized by an increase in RANTES level was significantly associated with lower baseline RANTES concentration (17,000 pg/mL vs. 32,000 pg/mL, p < 0.01) (Fig. 7). No differences were observed for IP-10. None of these profiles was associated with other parameters, including ALT, HCV viral load, histological grading and staging scores, and DAA therapy regimens. One patient had evidence of FCH and three of plasmacellular HCV recurrence with signs of autoimmune tissue damage: they had higher levels of baseline RANTES and IP-10 compared with the other LT-R and CHC patients (data not shown). All patients eventually cleared HCV infection. The five LT-R who experienced a virological relapse after the first DAA treatment showed similar patterns to those observed for LT-R responders and CHC, in terms of CK spikes after the successful DAA retreatment (Fig. 8a, b). CCR5 genotyping of the 18 LT-R patients showed the presence of 1 Δ32/Δ32 homozygous and 2 WT/Δ32 heterozygous haplotypes with a prevalence of 5.5% and 11.1%, respectively. In the CHC group 2 WT/Δ32 heterozygous (10%) were also found.
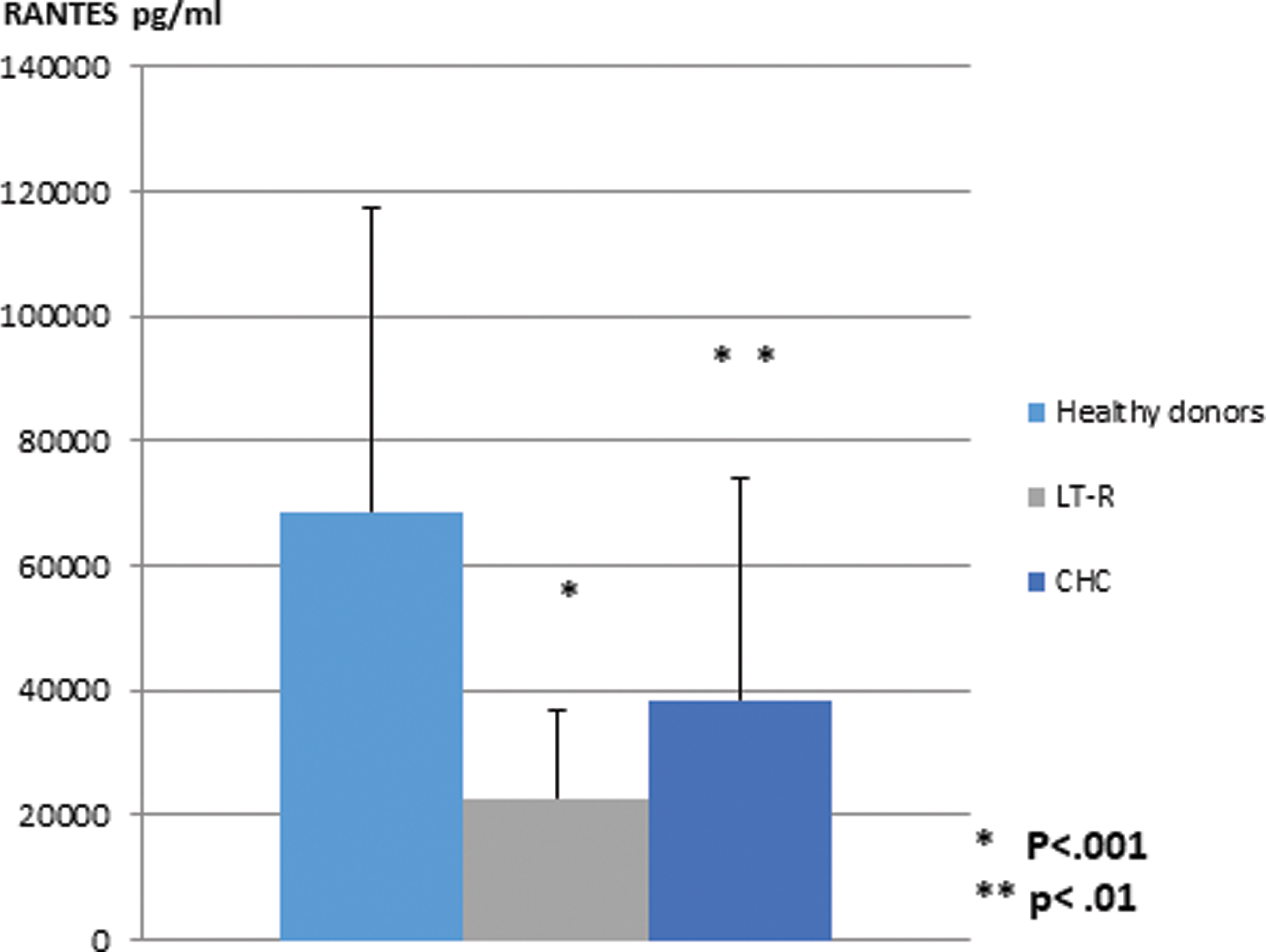
Mean RANTES values at baseline in LT-R and CHC patients as compared with HC. Results are expressed as pg/mL. Significant differences are observed between the two patients' populations and HC (*LT-R vs. HC, p < 0.001; **CHC vs. HC, p < 0.01). CHC, chronic hepatitis C; HC, healthy donors controls; LT-R, liver transplant recipients; RANTES, Regulated upon Activation Normal T cell Expressed and Secreted. Color images are available online.

Individual patients' RANTES values at different time points during the course of DAA treatment in LT-R
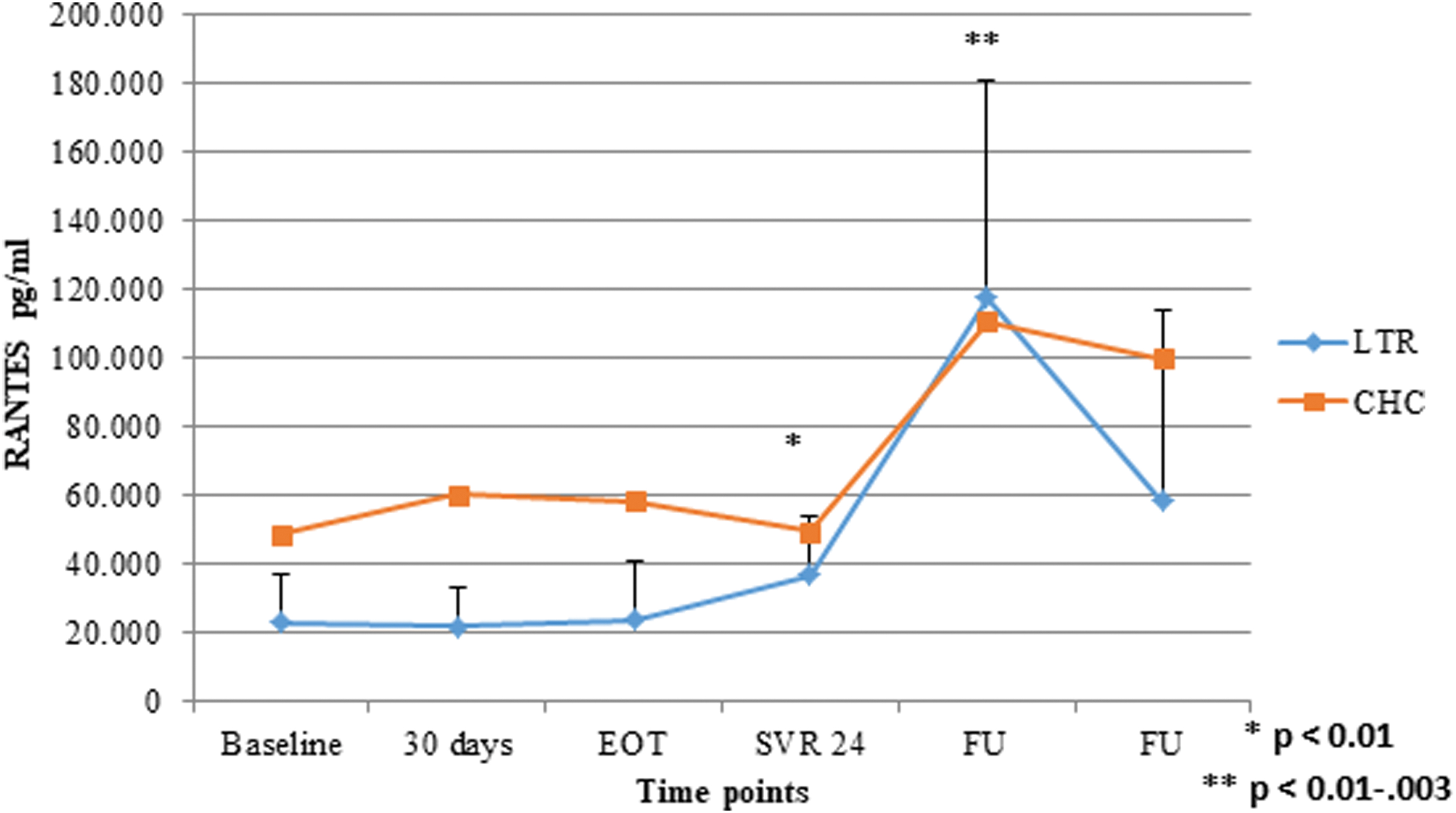
RANTES values (mean ± SD) at different time points during the course of DAA treatment in LT-R and CHC patients. Results are expressed as pg/mL. Significant differences are observed between baseline and SVR in LT-R (*p < 0.01) and between baseline and FU levels both in LT-R and CHC (**p < 0.03 and p < 0.01). SD, standard deviation; SVR, sustained virological response; FU, follow-up. Color images are available online.
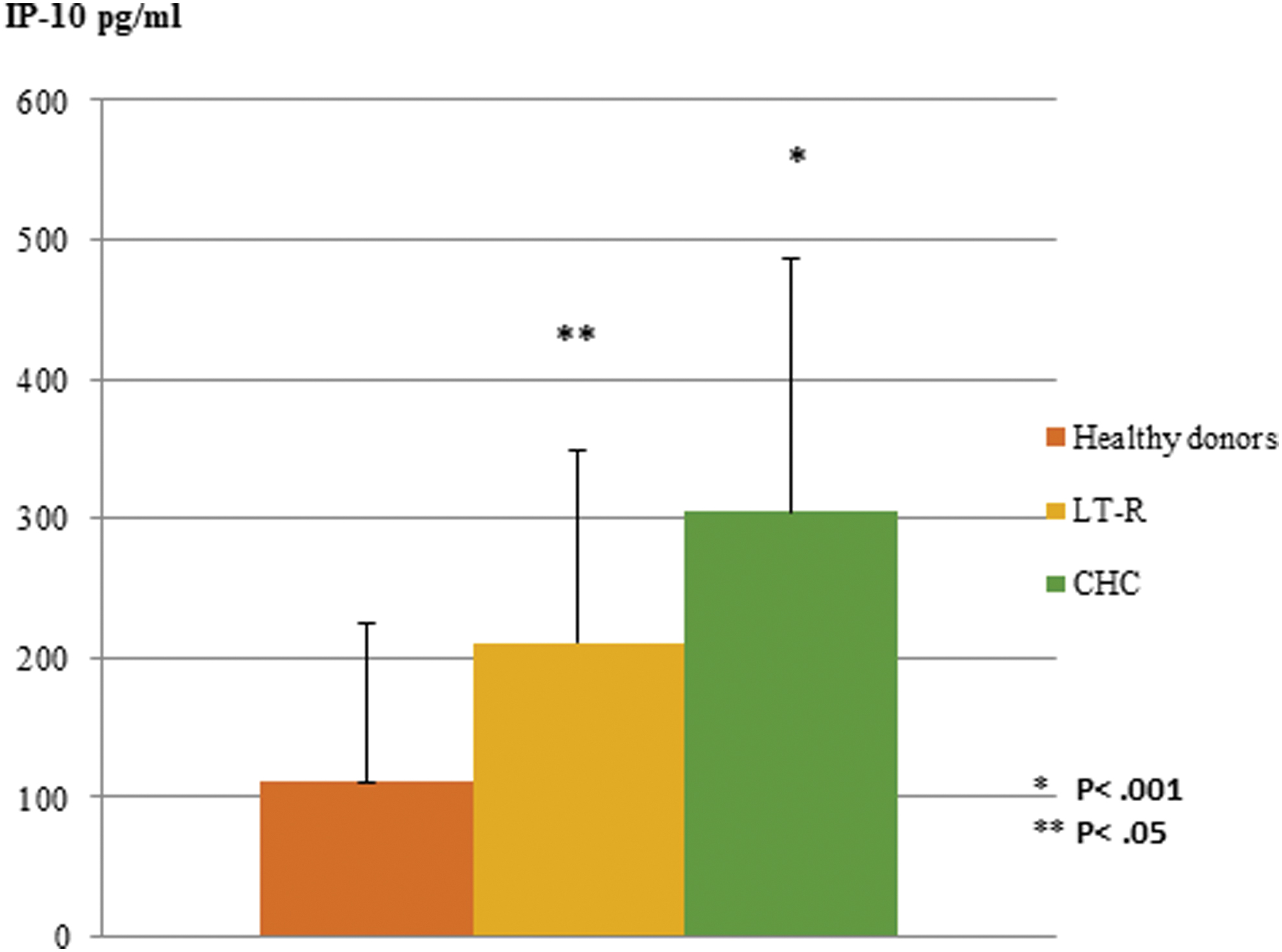
Mean IP-10 values at baseline in LT-R and CHC patients as compared with HC. Results are expressed as pg/mL. Significant differences are observed between the two patients' populations and HC (LT-R vs. HC, p < 0.05; CHC vs. HC, p < 0.01). Color images are available online.
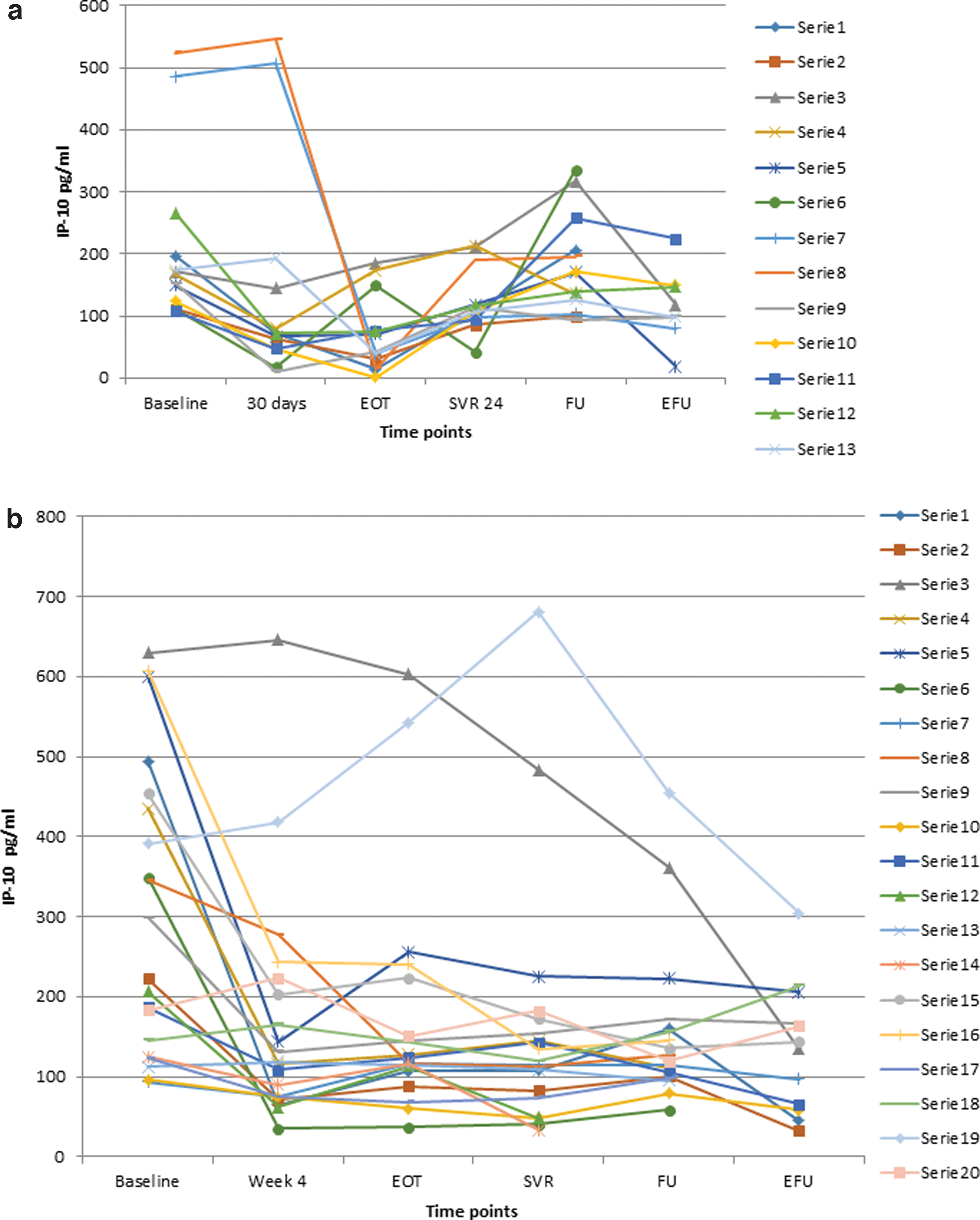
Individual patients' IP-10 values at different time points during the course of DAA treatment in LT-R
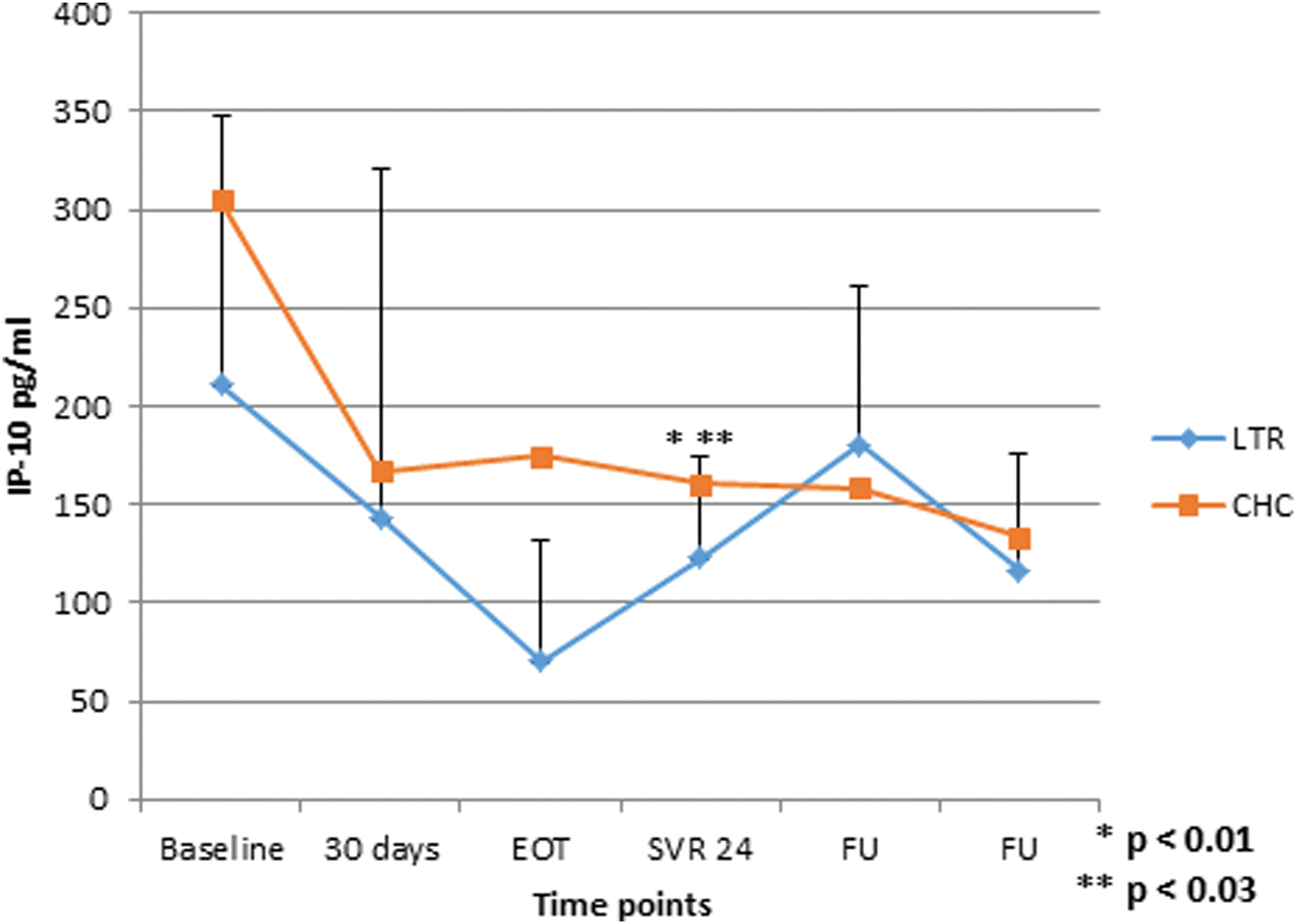
IP-10 values (mean ± SD) at different time points during the course of DAA treatment in LT-R and CHC patients. Results are expressed as pg/mL. Significant differences are observed between baseline and SVR levels for both LT-R and CHC (*LT-R SVR vs. baseline, p < 0.03; **CHC SVR vs. baseline, p < 0.01). Color images are available online.
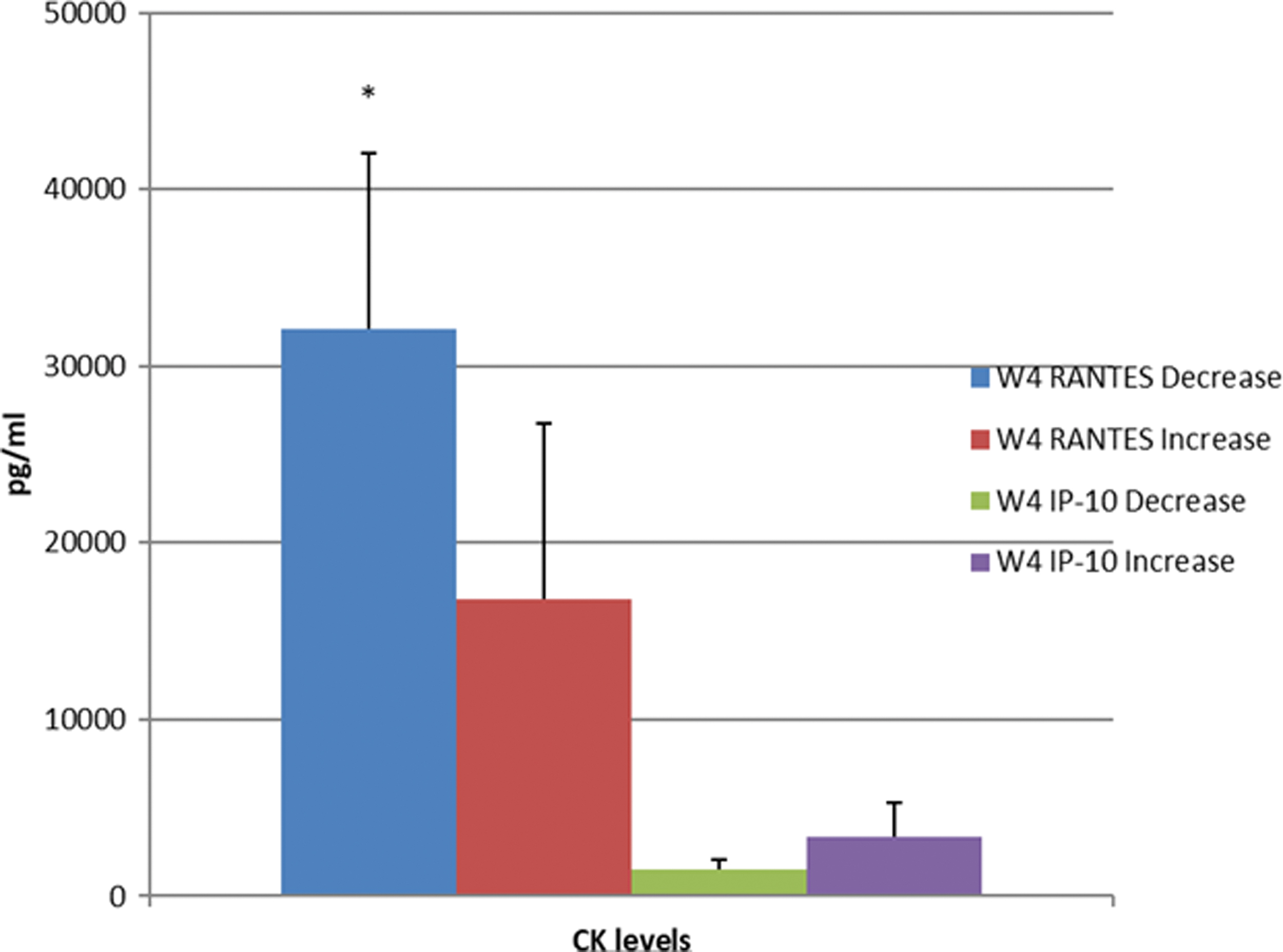
Baseline RANTES and IP-10 levels in LT-R patients who showed decreasing or increasing RANTES and IP-10 levels at week 4 of DAA treatment. RANTES values were significantly lower in patients who showed increased RANTES values (*p < 0.01). Color images are available online.
RANTES
Discussion
CK and their cognate receptors are known to be deeply involved in the immune response to pathogens and in the outcome of any infection (10). RANTES and IP-10 are the main CK of the CC5 and CXC3 pathways, active in the recruitment of effectors cells, mainly NK and lymphocytes, at the site of the lesion (32).
In our patients' population, including LT-R with recurrent HCV and immunocompetent CHC patients with DAA-induced HCV eradication, baseline RANTES levels were significantly lower than in noninfected HC, indicating a possible reduced activation of this pathway in HCV chronically infected patients. This could lead to a consequent lack of control on viral replication and is consistent with the high prevalence of CCR5 Δ32 alleles detected in our patients. One homozygous and two heterozygous deleted patients were observed in the LT-R with a remarkably higher rate than in the general population where it is extremely low (18,23). Owing to the limited sample size, these data may only suggest a specific enrichment of the deleted genotype in patients transplanted for advanced CHC with a consequent defective immune response to the virus. Additional larger studies might confirm whether carriers of the Δ32 allele are unable to induce an adequate recruitment of effector cells, resulting more susceptible to chronic HCV infection.
In our patients RANTES reduced expression before DAA treatment may be due to the suppression of CC5L gene promoter exerted on infected liver cells by HCV gene products, namely core and NS5A (9). This may be further supported by an increase of RANTES levels during the first 4 weeks of DAA therapy. A sharp HCV viral load decline with a very fast HCV-RNA suppression at week 4, as observed in these patients, is probably associated to the disappearance of the viral inhibitory effect on both RANTES production and release. Two hypotheses might explain the low baseline RANTES levels: the exhaustion of the immune system or the progressive damage of CC5L producing liver resident cells. The pattern of increasing RANTES during the following virological clearance and particularly after the end of therapy seems to support this interpretation. Reduced RANTES concentrations, with a subsequent decrease of chemotactic activity, are consistent with low levels of HCV-specific CD4 lymphocytes previously reported during chronic HCV infection (14).
Compared with RANTES, IP-10 showed a more predictable profile with higher baseline levels compared with HC, an expected pattern after the virus-induced release of IFN gamma (13).
The subsequent CK kinetics during and after DAA treatment showed in both LT-R and CHC an increase of RANTES several months after HCV eradication, as if an HCV-related inhibitory effect was finally removed. A progressive recovery, with severalfold spikes and with a return to baseline levels, was the predominant pattern mainly in the LT-R population. In both LT-R and CHC, IP-10 concentrations tend to reach healthy donors after HCV eradication. On the contrary, in patients with LT-R whose samples were available up to 2 years after SVR, RANTES appears to return to the initial low levels, suggesting a relapsing persistent partial suppression of the CC5 pathways in these individuals. This seems to be independent on the previous suppressive effect of HCV and may reflect a constitutive deficiency of the CC5 pathway instrumental for the initial chronicization of the virus infection in these patients.
In the small group of LT-R relapsers similar profiles were observed in the long-term FU after the second successful treatment regimen.
These data seem to confirm the hypothesis of an HCV-mediated suppression in the production and release of CCL5. As a potential confounding factor, the immunosuppressive treatment in our LT population does not seem to play a major role: the CK patterns are similar to those observed in the CHC group and none of CNI used are known to act directly on these pathways (19). Taken together these data suggest that the CC5 pathway is extensively altered during chronic HCV infection with a defective production of RANTES. This may result in a reduced recruitment and activation of CCR5 positive effector lymphocytes and a consequent increased severity of liver damage. In patients with advanced liver disease undergoing LT, the defective CC5-related immune response may be caused also by a high prevalence of the deleted genotype.
In conclusion, it might be of interest to continue monitoring RANTES levels in these patients as they may be at risk of other infections or immune-mediated diseases. Modulation of the CC5 pathway with agonist/antagonists may also be worth considering to control cell-mediated immunity reactions (25).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.