
Abstract
Coronavirus disease 2019 (COVID-19) a global infectious disease caused by severe acute respiratory coronavirus 2 (SARS-CoV-2) affects various organs, primarily the respiratory system, and presented with pulmonary manifestations such as acute lung injury (ALI) and acute respiratory distress syndrome. Levamisole (LVM) is an anthelminthic drug; it has immune-modulating effects through induction of type 1 immune response. Based on these findings several recent studies highlighted that LVM might be effective in preventing and treating SARS-CoV-2 infections. The aim of this report is to illustrate the potential role of LVM in SARS-CoV-2 infection and in the management of COVID-19. Different studies proposed that LVM may inhibit proliferation of SARS-CoV-2 through inhibition of papain-like protease. LVM may prevent ALI and acute kidney injury through activation of glucocorticoid receptors. In general, LVM has strong immune stimulant effects by modulating cellular and humoral immune responses. This effect is beneficial in the early phase of COVID-19 and harmful in the late phase. In the early phase, immune stimulation facilitates SARS-CoV-2 clearance and tissue repair, however, in the late phase, immune stimulation in COVID-19 may increase propagation risk of cytokine storm. In conclusion, LVM therapy in COVID-19 has bidirectional effects, beneficial in the early phase and harmful effects in the late phase of COVID-19. Clinical trial and prospective studies are warranted in this regard to confirm the efficacy and timing administration of LVM in the management of COVID-19.
Introduction
Coronavirus disease 2019 (COVID-19) a global infectious disease caused by severe acute respiratory coronavirus 2 (SARS-CoV-2). It affects various organs, primarily the respiratory system, and presented with pulmonary manifestations such as acute lung injury (ALI), acute respiratory distress syndrome. COVID-19 is also presented with extrapulmonary manifestation such as acute cardiac injury, neurological disorders, pancreatic injury, and acute kidney injury (AKI) (23,21). This systemic effect of COVID-19 is due to the wide distribution of angiotensin converting enzyme 2 (ACE2), a receptor and entry point for SARS-CoV-2 (5). ACE2 receptor is chiefly expressed in lung alveolar cells type II, proximal renal tubules, immune cells, and intestines (3). The binding of SARS-CoV-2 to ACE2 is associated with downregulation of ACE2 receptor with consequent intensification in the level of vasoconstrictors angiotensin II (Ang II) and reduction of vasodilator angiotensin (Ang 1–7), (Ang 1–9) with induction release of proinflammatory cytokines (4). Since the World Health Organization (WHO) declaration of this disease as a pandemic, and till late February 2021, the total confirmed cases are 109,326,628, with 2,248,181 deaths. In this global dilemma, several efforts and advancing researches are developed to finding effective agents against SARS-CoV-2 from recent or old approved drugs as repurposing drug strategies (22).
Immunological Effect of Levamisole
Levamisole (LVM) is an anthelminthic drug first used in 1969 and in the management of colonic carcinoma, leprosy, and nephritic syndrome (16). LVM has immune-modulating effects, including improvement of T cell functions through activation of cholinergic-dependent cyclic guanosine monophosphate, modulation of B cell functions and antibody productions, reduction of circulating immune complexes, and modulation of the immune response through activation of interleukin (IL)-18 (15). It has been reported that LVM therapy in rats is associated with elevation of interferon-gamma (INF-γ), CD4/CD8 ratio, and IL-18 with reduction of IL-4 through induction of type 1 immune response (9). Different experimental studies confirmed that LVM therapy in allergic rhinitis models increases IL-12, IL-18, and INF-γ with the reduction of IL-4, IL-5, and IL-13 (29).
LVM activates monocyte–macrophage axis functions through stimulation of chemotaxis and phagocytosis (13). Likewise, LVM increases proinflammatory cytokines and inhibits anti-inflammatory cytokines. Therefore, LVM is an effective agent against various viral infections such as rotavirus by activating release of INF-γ and IgG production (11). Of note, LVM augments the humoral immune response to the hepatitis B (HB) vaccine and immunodeficiency virus (HIV) (2). Thus, coadministration of LVM with HB vaccine enhances immune response in anti-HBs antibody generation (7). A meta-analysis study showed that LVM efficiently stimulates an immune response in patients with end-stage kidney disease. Coadministration of LVM with HB vaccine may enhance humoral immune response in patients with chronic hemodialysis through modulation of B cell immune response (18,25). Although LVM reduces TNF-α in patients with recurrent aphthous ulcerations (12) and helps in the management of steroid-sensitive nephrotic syndrome to avoid steroid toxicity, LVM also reduces circulating immune complexes in patients with relapsing nephrotic syndrome (20). Recently, Rastgou et al. illustrated that LVM improves humoral immune response in patients with HIV through increase in expression of IL-4 (30).
In summary, the immunological effects of LVM are through modulation of the following: Improves T cell functions Modulates B and T cell functions and antibody productions Improves immune response through activation of IL-18 Activates monocyte–macrophage axis functions.
LVM and COVID-19
Based on these findings, several recent studies highlighted that LVM might be effective in preventing and treating SARS-CoV-2 infections (10). It has been reported that LVM may inhibit proliferation of SARS-CoV-2 and associated inflammatory reactions through inhibition of papain-like protease (PL-pro) and release of IL-6 and TNF-α (6). SARS-CoV-2 PL-pro is important for cleaving viral polyprotein to release nonstructural proteins, glycation of the viral polyprotein, and viral replication. As well, SARS-CoV-2 PL-pro modulates host immune response; therefore, PL-pro inhibitors may be a promising target against SARS-CoV-2 infection (24). Previous studies illustrated that inhibition of SARS-CoV PL-pro led to promising results in the mitigation of SARS, 2003 (20). Arya et al. (7), in silico study, confirmed that LVM has a potential inhibitory effect on the SARS-CoV-2 PL-pro and might be effective in the management COVID-19.
Abeyagunawardena et al. in a randomized double-blind clinical trial tests the efficacy of LVM in the management of COVID-19, involved 50 COVID-19 patients, 25 on the standard care therapy plus placebo and 25 on the standard care therapy plus LVM, illustrated that LVM reduced dyspnea and improved clinical outcomes within 14 days (1). Furthermore, a clinical trial of the combination of LVM, budesonide, and formaterol inhaler was done and showed early clinical improvements in COVID-19 patients (27). LVM has an immune-enhancing effect, thereby increasing host immune response and viral clearance. Theoretically, coadministration of LVM with the COVID-19 vaccine may enhance the humoral immune response and immunization against SARS-CoV-2.
It has been reported that LVM action is mediated through the expression and activation of wide spread glucocorticoid receptors, and so glucocorticoid receptor antagonist such as mifepristone may abolish this action. Therefore, LVM may prevent ALI and AKI through activation of glucocorticoid receptors (17,19). ALI and AKI are the most typical pathological presentation of COVID-19; thereby, LVM has potential therapeutic application in the management of COVID-19 (27). During SARS-CoV-2, the mammalian target of rapamycin (mTOR) is activated with inhibition of p53. Activation of mTOR inhibits host cells for INF production, whereas inhibition of p53 is associated with high viral survival. Thus, mTOR inhibitors and p53 activators might attenuate SARS-CoV-2 (8). LVM inhibits p53 by activating glucocorticoid receptors, which may propagate SARS-CoV-2 proliferation and infection (28).
LVM has strong immune stimulant effects by modulating cellular and humoral immune responses. This effect is beneficial in the early phase of COVID-19 and harmful in the late phase. In the early phase, immune stimulation facilitates SARS-CoV-2 clearance and tissue repair (Fig. 1). However, late-phase immune stimulation in COVID-19 may increase the risk of cytokine storm propagation (9). Thus, the potential role of LVM in the management of COVID-19 should be re-evaluated and not merely depended on the in vitro findings only since in vivo immune stimulant effect may worsen the exaggerated immune response during SARS-CoV-2–induced cytokine storm (Fig. 2).
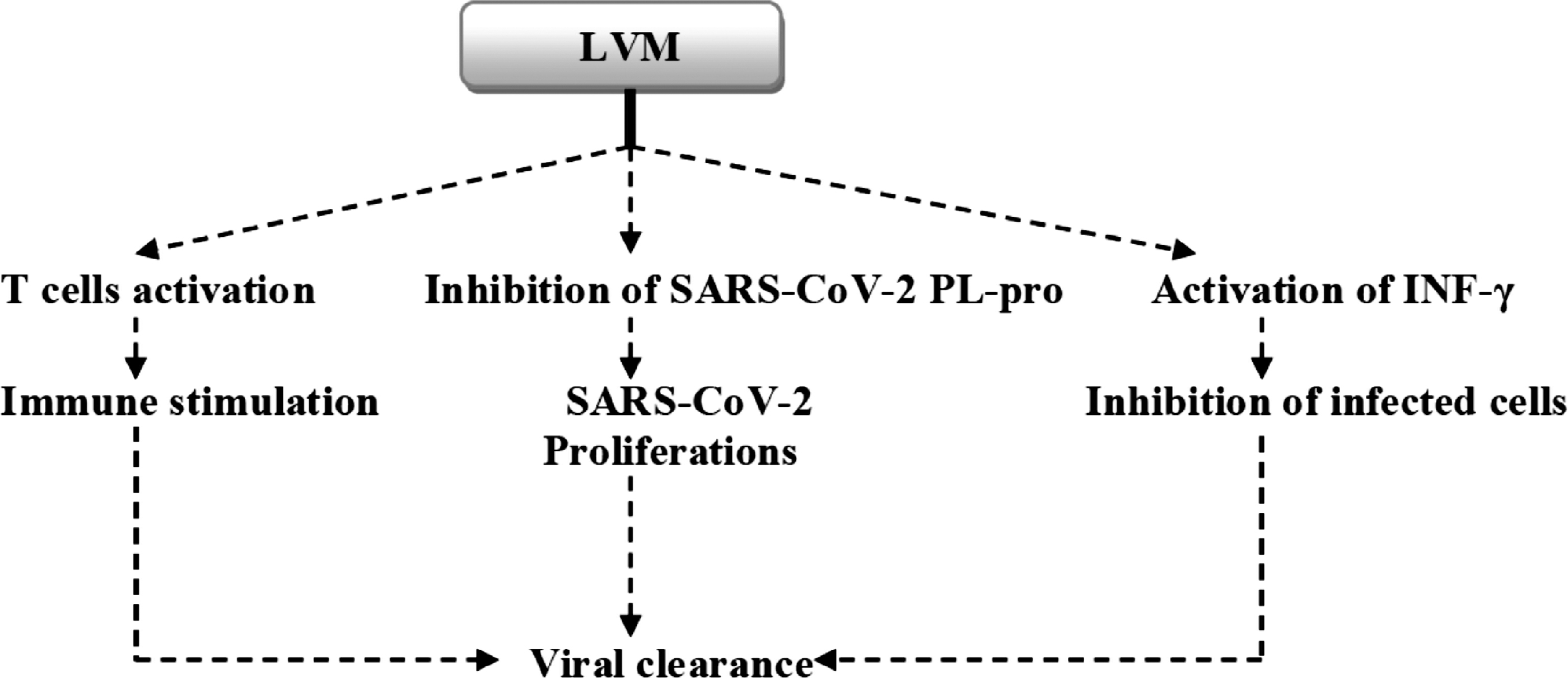
LVM in early SARS-CoV-2 infection. LVM, levamisole; PL-pro, papain-like protease; SARS-CoV-2, severe acute respiratory coronavirus 2.
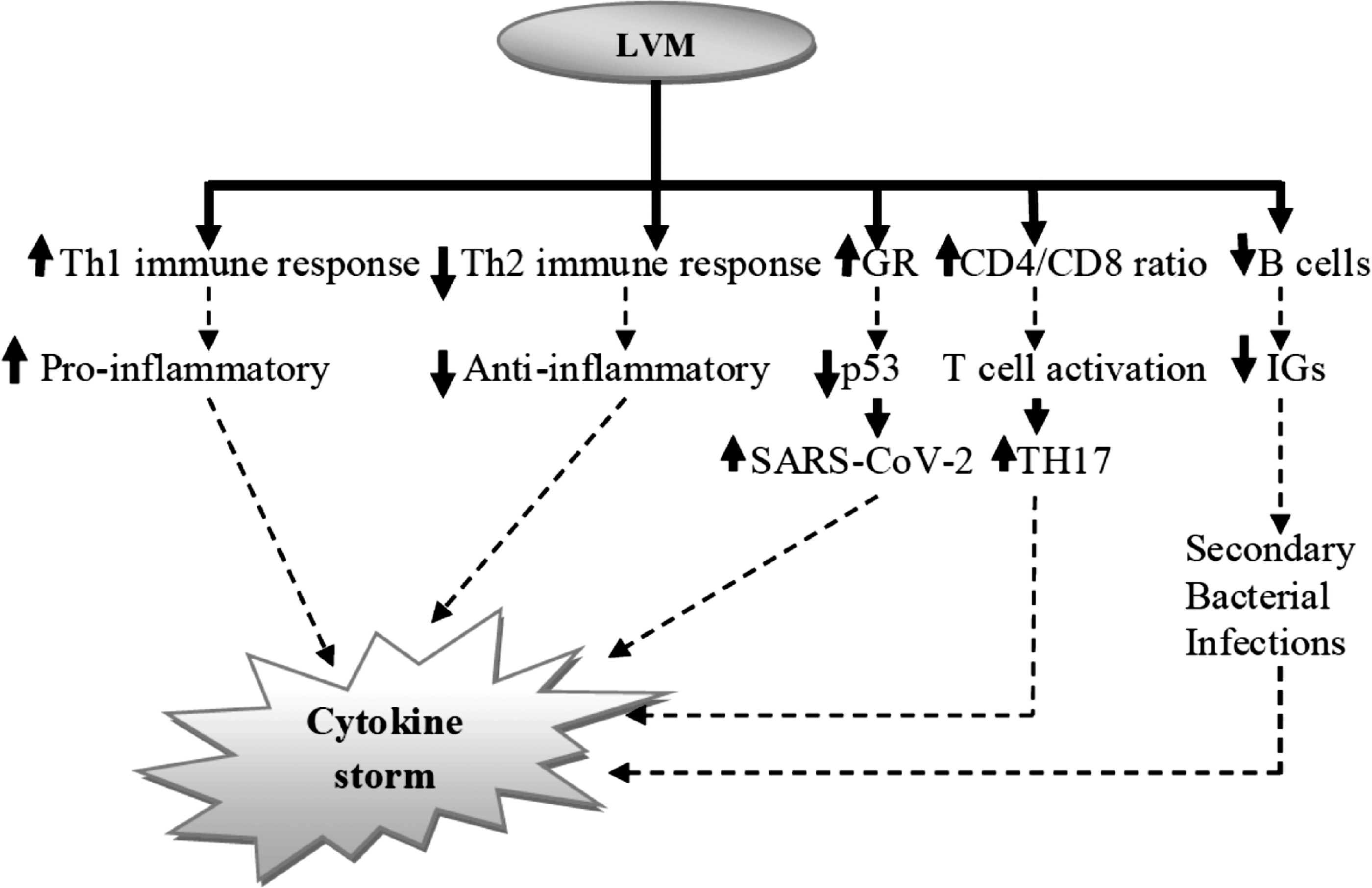
LVM in late SARS-CoV-2 infection and risk of the cytokine storm. GR, glucocorticoid receptors; IG, immunoglobulin.
However, LVM therapy is associated with different adverse effects, including leukopenia, pyrexia, fixed drug eruptions, leg ulcer, skin necrosis, agranulocytosis, pulmonary hypertension, acute coronary syndrome, vasculitis, and thrombocytopenia (26). These adverse effects may affect the clinical presentations and outcomes of COVID-19 patients and burden the general health condition (14).
Conclusion
LVM therapy in COVID-19 has bidirectional effects, beneficial in the early phase of COVID-19 through anti-SARS-CoV-2 effect, augmentation of Th1 immune response that enhance SARS CoV-2 clearance and harmful effects in the late phase of COVID-19 through suppression of Th2 immune response and propagation of proinflammatory cytokines to cytokine storm. Clinical trial and prospective studies are warranted in this regard to confirm efficacy and timing of administration of LVM in the management of COVID-19.
Footnotes
Authors' Contributions
The authors contributed equally to the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.