
Abstract
Human health has always been challenged by variety of viral infections, but severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has surpassed all previous viral diseases and emerged as a major health challenge around the globe. Real-time polymerase chain reaction (PCR) is the gold standard for the diagnosis of SARS-CoV-2 and serological assay provides a compliment to diagnosis after second week of infection. The aim of the study is the characterization of antibody response to SARS-CoV-2 in the blood sample of diagnosed coronavirus disease 2019 (COVID-19) patients, and its potential association with factors such as age, gender, time, and symptoms. Serum from 248 confirmed SARS-CoV-2 patients was investigated for antibodies. Elecsys anti-SARS chemiluminescent immune assay was performed for the detection of nucleocapsid-specific antibodies. Association of antibody response with gender, age, and time after onset of symptoms was analyzed. Among 248 PCR positive SARS-CoV-2 patients, 214 (86.3%) have virus-specific antibody signals. Antibodies positivity rate was higher in male patient patients as compared with female patients (90.8% vs. 79.2%, p = 0.009). Patients aged 30–40 years had the highest antibody positivity rate as compared with other groups (89.10%, p = 0.04). Patients age group >60 years had a lower positivity rate (75%, p = 0.04). The increasing trend in the antibodies detection with time was observed, maximum positive antibodies response rate observed at 8 weeks. Patients were categorized on the basis of clinical symptoms into asymptomatic, mild, and moderate; 17.7% were asymptomatic, 60.5% showed mild symptoms, and 21.8% showed moderate symptoms of the disease. Males were seen to be more asymptomatic as compared with females (i.e., 59.1% to 40.9%). The serological test for SARS-CoV-2 has a high sensitivity at >2 weeks after the positive PCR result or onset of illness. In addition, the serological response differs among patients based on gender, age, as well as time between the onset of symptoms or PCR confirmation and sample collection for the study of antibody response.
Introduction
Human health has always been challenged by plethora of viral infections; among these, coronavirus became a major challenge throughout the world. Coronavirus was discovered in 1960 by group of virologist led by Tyrrell (40). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in 2019 causing respiratory syndrome associated with the infection and was assigned name coronavirus disease 2019 (COVID-19) (20) by the World Health Organization (WHO). WHO declared the outbreak a public health emergency of international concern on 30th January 2020 (36,46,47).
Later in March 2020, WHO declared a global pandemic in response to the emerging SARS-CoV-2. Since then, efforts have been under way to control its spread. Diagnosis of COVID-19 on the basis of clinical symptoms alone is not reliable because symptoms are similar with many respiratory viruses and bacterial pneumonia. Therefore, diagnostic tests for SARS-CoV infection were needed. In response to this, real-time reverse transcriptase assay and antibody assay for the detection were developed and being used.
Serological testing measures the antibody response to the SARS-CoV-2 and may be a promising way to compliment the diagnosis. It may also be useful to improve our understanding of pathogenesis. It is also helpful to identify people who are negative according to nucleic acid testing (28). It helps to understand transmission intensity and population susceptibility. In addition, assays measure antibody response and determine seroconversion and herd immunity (38). Moreover, serological assays allow the identification of persons who have strong antibody response and could be donors of plasma and serum therapeutics (4).
However, in mild infections or asymptomatic cases, the invisible part of iceberg can be estimated by using population based sero susceptibility (29). Antibodies to the nucleocapsid are considered as a sensitive target. Serological tests that detect antibodies to nucleocapsid protein are sensitive for the diagnosis of COVID infection (25,50). Nucleocapsid serological testing by chemiluminiscent immunoassay has been reported (27) to be helpful to elucidate the correlates that have a potential role in immunity after infection (3,37).
The primary objective of this study is characterization of antibody response to SARS-CoV-2 in blood sample of patients with confirmed COVID-19 infection and its potential association with factors such as age, gender, time, and symptoms.
Methods
This study was conducted at Nuclear Medicine, Oncology and Radiotherapy Institute (NORI), Islamabad, Pakistan from June 2020 to April 2021. This is cross sectional study approved research training and monitoring cell/institutional review board and ethics committee of the institute. Informed written consent was obtained from all the patients who participated. Sample collected from polymerase chain reaction (PCR) confirmed SARS-CoV-2 patients during June 2020 to April 2021.
The time of sample collection for antibody detection varied between 2 weeks and >8 weeks after onset of clinical symptoms compatible with COVID-19 infection. Date of PCR positive result was considered if the patients were asymptomatic or date of symptoms was not available. The blood samples were collected and upon centrifugation, the serum specimen was separated. Serum samples were used for serological testing to monitor the presences of antibodies against SARS-CoV-2 and later was stored at −20°C. Symptoms were also recorded for all patients.
SARS-COV-2 antibody assay
SARS-CoV-2 antibody test was performed on Cobas 6000 analyzer (Roche Diagnostics, Rotkreuz, Switzerland). Elecsys anti-SARS-CoV-2 assay is an electrochemiluminescence immunoassay that detects total antibodies that have high affinity for recombinant protein representing nucleocapsid antigen in human serum. Results are reported as a cutoff index (COI) and interpreted as nonreactive (COI <1.0) or reactive (COI ≥1.0). This is a U.S. Food and Drug Administration Emergency Use Authorization–approved chemiluminescent immunoassay.
Statistical analysis
SPSS v. 15.0 (SPSS, Inc., Chicago, IL) was used for analysis. Categorical variables are expressed as the number and percentage. Pearson's chi-square test was used to evaluate the associations of variables with the likelihood of achieving nucleocapsid antibodies. A p-value <0.05 was considered significant.
Results
Two hundred forty-eight coronavirus confirmed cases were included in this study, of which 152 were males and 96 were females. The characteristics of patients are summarized in Table 1.
Characteristics of Patients Included in the Study
Mild symptomatic (fever, body ache, loss of smell, and loss of taste). Moderate symptomatic (fever, body ache, loss of smell, loss of taste, and cough).
Performance of nucleocapsid antibody assay
Elecsys Anti-SARS-CoV-2 assay detects the antibodies that were developed using SARS-CoV-2 nucleocapsid. The sensitivity of the assay was tested with serum samples from patients collected between 2 and 4 weeks postsymptoms onset in symptomatic patients and in asymptomatic patients after (2–4 weeks) tested positive by PCR. The specificity of the assay was tested with serum samples stored before the COVID-19 pandemic from hepatitis patients, no cross-reactivity or false positive results were observed. Sensitivity of the assay was 92.0% and specificity 98.5% in sample from PCR confirmed SARS-CoV-2 infection. Receiver operating characteristic (ROC) curve analysis was used to study the performance of the assay. The area under the curve is 0.946. ROC curve evaluates the trade-off between true positive (sensitivity) versus false positive (1-specificity) (Fig. 1).

ROC-AUC analysis of anti-SARS-CoV-2 serological test. ROC curves for Roche Elecsys anti-SARS-CoV-2 assay. The AUC is 0.946 indicates the test accuracy. ROC curve shows the relationship between true positive (sensitivity) versus false positive (1-specificity). ROC-AUC, receiver operating characteristic-area under the curve; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Antibody response
Out of 248 PCR positive coronavirus patients, 214 patients (86.3%) had virus-specific antibodies >1 COI. A COI >1 is considered reactive. Thirty-four (13.7%) patients had antibody titer <1 and considered as nonreactive. The preliminary analysis showed that % positive rates of antibodies were higher in male patients as compared with female patients (90.8% vs. 79.2%, p = 0.009) (Fig. 2). Patients were divided into five groups on the basis of their age. The number of tests as well as number of positive results in each group is shown in Figure 3a.
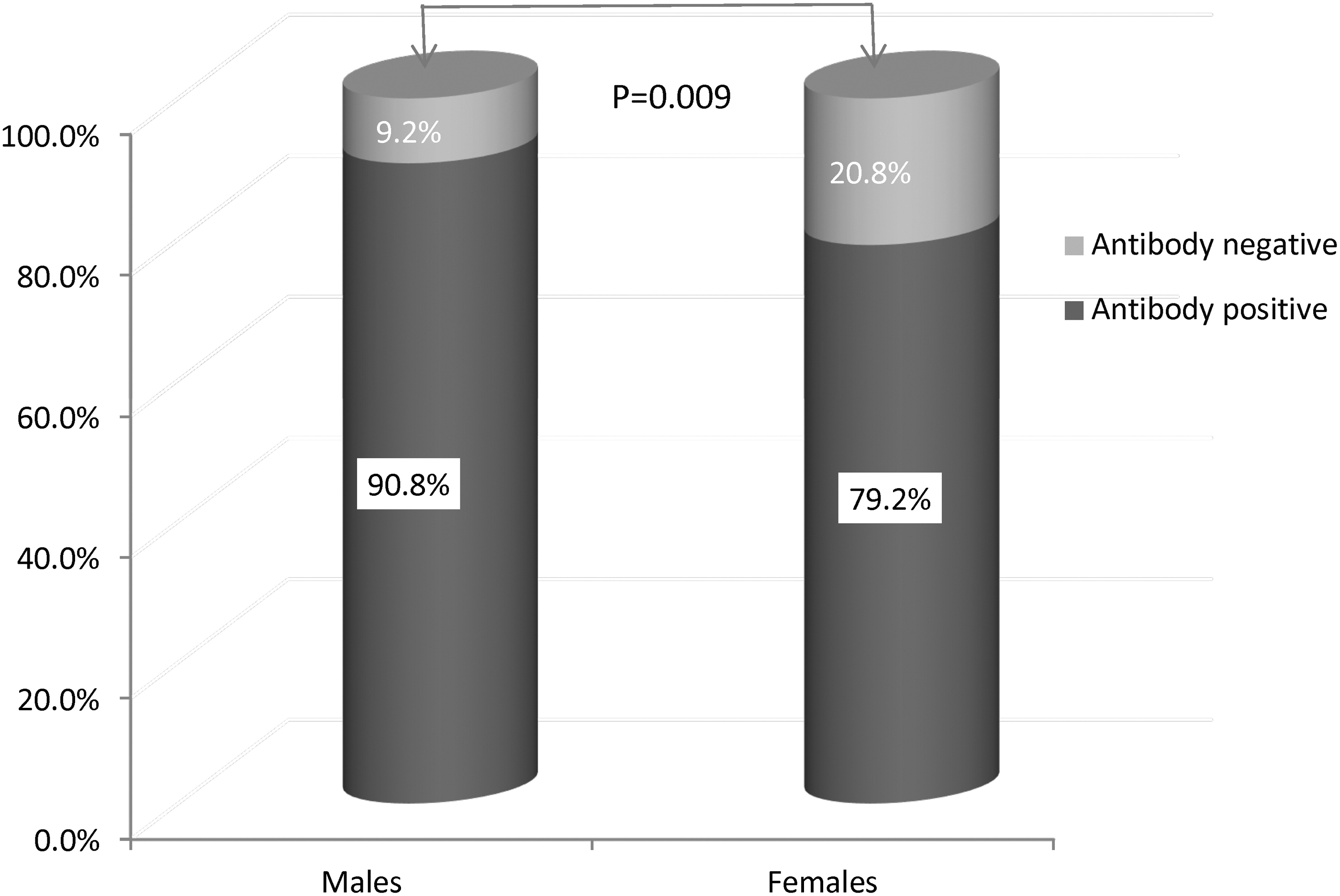
Antibody positive and negative rate in COVID-19 male and female patients. Vertical bars show percent antibody positive and negative cases among COVID-19 patients. The p-value was calculated using the chi-square test. COVID-19, coronavirus disease 2019.
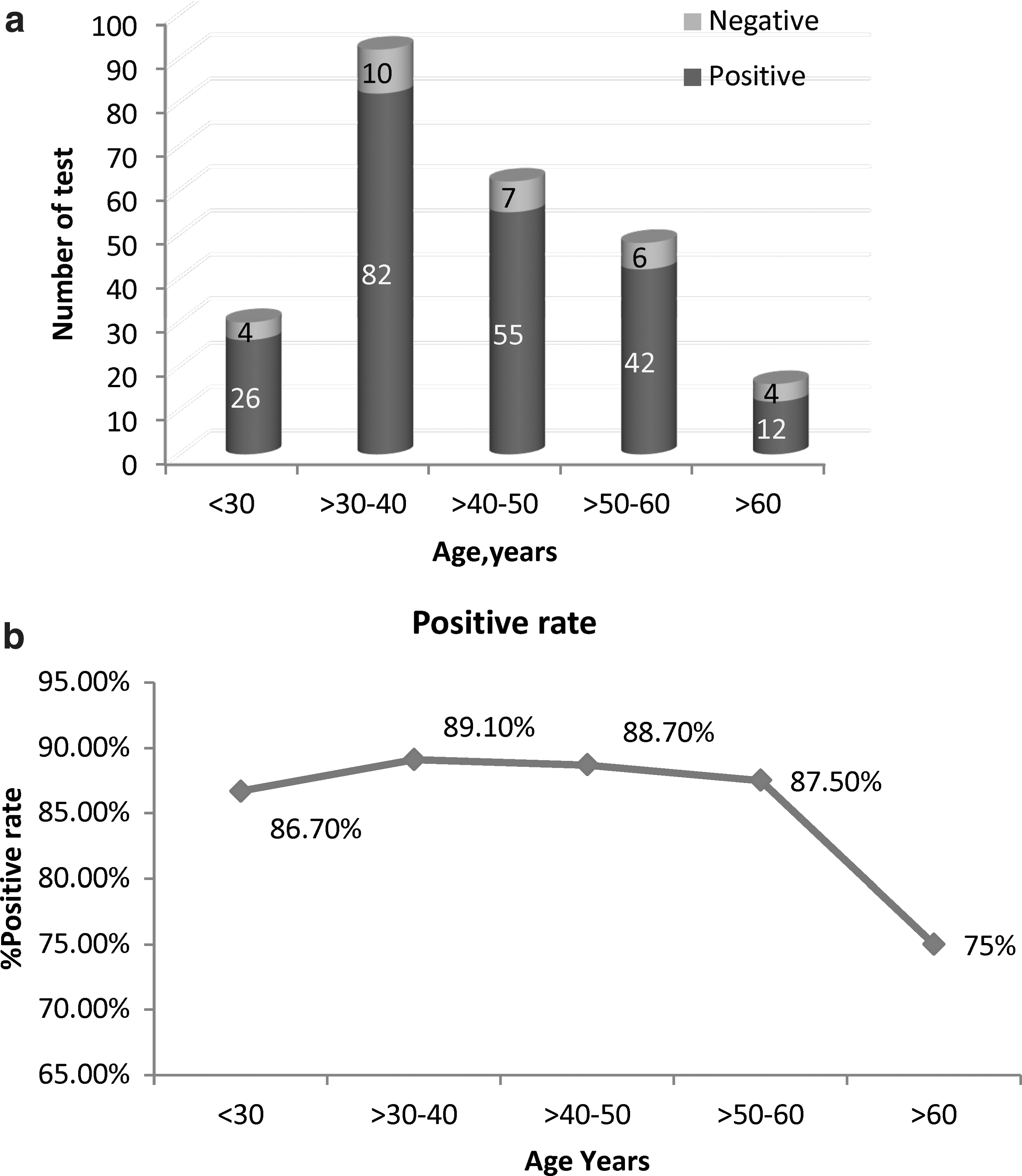
Antibody positive rate was observed as shown in Figure 3b. Patients aged 30–40 years had the highest positivity rate as compared with other groups (89.10%, p = 0.04). Patients aged >60 years had a lower positivity rate (75%, p = 0.04) (Fig. 3b). Antibodies response in patients was observed at 2 weeks interval each. Among the patients who were tested PCR positive for SARS-CoV-2, samples were collected at 2 weeks after the onset of the symptoms. Percentage positive rate was calculated based on the total number of patients who showed antibodies response with score greater than COI >1.
The % positive response rate increased from 54.5% (≤week 2) to 88.9% at 8 weeks in about 45–55 days after being PCR positive result and onset of the symptoms. The % positive rate at 2 weeks after PCR positive result was lower as compared with that at eighth week after the PCR positive and symptoms onset. The graph shows the increasing trend in the antibodies detection overtime, with maximum positive antibodies response rate at 8 weeks (Fig. 4).
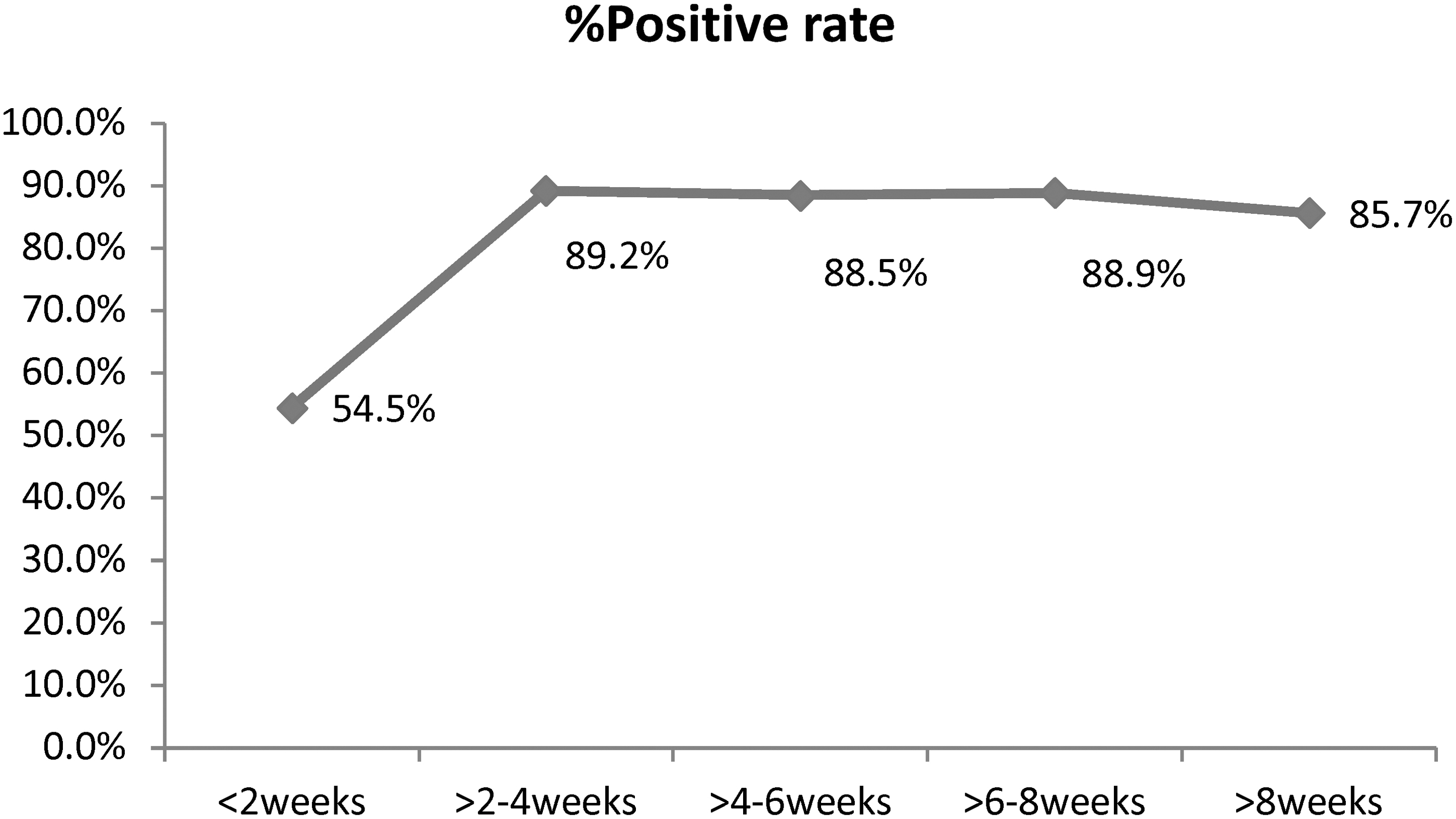
Correlation between antibody-positive rate and time. SARS-CoV-specific antibody positive rate plotted against the number of weeks post-PCR confirmation. (less than <, > greater than). PCR, polymerase chain reaction.
Furthermore, serological testing for surveillance was carried in 50 close contacts of patients with known COVID-19. Five individuals were confirmed to be infected by antigen test and PCR test. The other 45 individuals had negative antigen result and no symptoms. After 18 days (>2 weeks) sample were collected for a nucleocapsid antibody test. Five of the patients who had negative antigen test result (5/45) were positive for virus-specific antibody indicated that close contact were missed by antigen test. Moreover, the five cases that had positive virus-specific antibody were asymptomatic (Fig. 5).

Serological testing in close contacts with COVID-19 patients.
All the patients had a wide range of symptoms with commonly occurring symptoms such as fever, myalgia, anosmia, ageusia, and cough. These clinical symptoms were divided into three categories, with patients showing no symptoms at all labeled as asymptomatic, and the mild category comprised patients with fever, myalgia, anosmia, and ageusia. Patients with cough along with other symptoms (fever, myalgia, anosmia, and ageusia) were labeled as moderate cases. The results show that 17.7% of the patients were asymptomatic, 60.5% had mild symptoms, and only 21.8% showed moderate symptoms of the disease. To investigate the association of antibody response to the symptoms of disease, antibody response is expressed using COI and symptoms are stratified as asymptomatic, mild, and moderate symptoms.
Antibody response was higher (92.6%) in patients with moderate symptoms as compared with those having mild symptoms 86.7% and asymptomatic 77.3%. We did not find significant relatedness between age and symptoms. Results show that in the age group between 30 and 40 years, moderate symptoms were more frequent (40.7%, p = 0.5). On analyzing gender association with symptoms, males were seen to be more asymptomatic as compared with females (59.1% to 40.9%).
Discussion
Our study evaluates the behavior of SARS-CoV-2 nucleocapsid-specific antibodies. For this we used Elecsys Anti-SARS-CoV-2 assay. The assay has high sensitivity and specificity for antibody detection (27). The analysis of serum sample showed that antibodies appeared ≤2 weeks (8–15 days) after onset of symptoms. In this study, more males were infected with SARS-CoV-2 (61.3%) than females (38.7%). This finding is in contrast with Kowitdamrong et al. (21) who reported 60% females and 40% males infected with coronavirus.
Our outcome agreed with the finding that men are more likely to contract SARS-CoV-2 as they may be exposed to the virus in non-health care settings (2). In addition, higher susceptibility of men as compared with women has been reported. From China, a higher COVID-19 death rate has been reported in men (4.7%) as compared with women (2.8%). Similarly, in Italy the COVID-19 death rate is 16.6% in men compared with 9.1% in women (1,12). A higher antibody level was observed in males than in females (20). However, it is said that there are many mechanisms through which gender has its effect on the immunity (33).
As compared with males, females exhibit stronger innate and humoral immune responses, and are consequently less vulnerable to many bacterial, fungal, parasitic, and viral infections (32). However, according to our results, antibody positive rates of 90.8% in males is significantly >79.2% in females (p < 0.005). The most likely explanation of this finding is male predominance in our study population. This may be attributed to factors such as the employment structure in Pakistan; male to female differences in antibodies is likely due to more exposure of the male to the outside environment regarding their job requirements and other outdoor activities for their families.
Consistent with the literature is that seroprevalence to COVID-19 is higher among people who have higher SARS-CoV-2 exposure due to the nature of their job (24,30). Other reported facts in the literature is that the severity of disease leads to enhanced inflammatory response, which leads to higher antibody production. When we analyzed antibody response with clinical symptoms, it was observed that the patients with moderate symptoms had higher antibody response (96.3%) than patients who had mild symptoms (86.7%).
Our male patients showed higher levels of developed antibodies as males infected with SARS-CoV-2 showed more moderate symptoms (74.1%) than females (25.9%). Our results can be explained by the fact that in severe disease, elevated inflammatory response has been hypothesized to lead to robust antibody production from B lymphocytes. However, this postulated link has yet to be tested in larger data. Many studies claim higher antibody response in females but males have been hypothesized to have severe clinical disease and higher antibody loads because of regulatory T cells, expression of angiotensin-converting enzyme 2 (ACE2), or other mechanisms related to sex hormones (21).
Some reports suggest that androgen may play a role in the severity of disease between males and females, as androgen plays a regulatory role in transmembrane protease, which is required for SARS-Cov-2 infectivity (43). The same phenomenon of correlation of higher antibody production with disease severity is observed in other infectious diseases such as tuberculosis (48). The other likely reason would be that our entire female population was premenopausal and had fewer comorbidities such as hypertension and Ischemic heart disease, as compared with the male population. Coexistent comorbidities risk factors are reported to have worse SARS-CoV-2 symptoms and disease outcome. Our study findings also echo outcomes of many population-based surveys conducted in Europe, USA, Brazil, Asia, and so on, which showed higher prevalence of seroprevalence in male population (16,23,51).
The Elecsys anti-SARS-CoV-2 immunoassay was used to investigate nucleocapsid antibodies in patients with COVID-19 infection. The method works on a double-antigen sandwich principal for the detection of mature antibodies to SARS-CoV-2. In this study, the assay demonstrates overall sensitivity 92.0% and specificity 98.5% in samples from PCR confirmed SARS-CoV-2 infection. This is consistent with the finding observed by Muench et al. who reported 99.80% specificity for SARS-CoV-2 antibody detection by the Elecsys SARS-CoV assay (27). Other studies also confirmed the performance of the Elecsys assay, which are comparable with and better in terms of specificity and sensitivity for other serological assays that showed sensitivity 75–100% at 14 days after confirmation by PCR (5,37).
Plasma samples showed that antibodies appeared between 8 and 15 days (≤2 weeks) after the onset of symptoms. Antibody signal to cutoff shown to rise with time and a peak observed between 6- and 8-weeks postsymptoms onset and with subsequent decline. Other studies also demonstrated that antibodies appeared and were detected in majority of the patients after a week of diagnosis (34,49). Specific immune response is important for determining protection as demonstrated for other viruses (42). The antibody positive rate in ≤2 weeks of symptom onset is only 54.5%. The rate increases to 89.2% in >2–4 weeks and 88.9% during week 8 and then decline in the antibody level appears after week 8.
This is consistent with finding observed by Vabret et al. and Huang et al. that antibody level decreases in the eighth week postsymptom onset (17,41). Studies conducted previously on humoral response in SARS and MERS exhibited that humoral response showed downward trend over the period (6,7). Moreover, in our analysis in close contacts of COVID patients who had negative antigen test results, 5/45 were positive for virus-specific antibody indicated that close contact were missed by antigen test. This highlights the importance of antibody testing as the sensitivity of antigen test ranges between 70% and 90% in symptomatic individuals and <50% in asymptomatic close contacts of COVID patients (11,39).
Our study showed that 13.3% of the individuals with mild symptoms and 20.5% with moderate symptoms did not develop antibody response specific to COVID-19. Others studies have also reported variation in response, reported 20–30% of cases had negative response for antibodies with mild symptoms (21,44). Our results indicate that patients with moderate symptoms developed antibodies greater in number as compared with patients who were asymptomatic or with mild symptoms. Some of the patients did not develop antibodies after sufficient time (6–8 weeks) with mild to moderate symptoms. This is in agreement with other reported studies showing that 3.9% of PCR confirmed patients remains seronegative for antibodies (3,14,26).
Rapid decay of neutralizing antibodies with half-lives in weeks is reported in various studies (18). The mechanism behind this rapid decay is well explained. How the waning titer of neutralizing antibodies will provide protection against the future SARS-CoV infection is an area of great interest. The exploration at this front has highlighted the role of cellular immunity in the of form memory B cells and CD4+ and CD8+ T cells, which may subsequently take over and provide protection against the reinfection (9,35). Although mechanisms underlying this recall immunity is not yet fully understood, there are few studies that have highlighted the role of recall immunity for long-term protection.
There have been many studies that confirmed the rising titers of circulating memory B cells for several months post-COVID-19 infection (15,45). This indirectly suggests that recall of B cell memory may provide more lasting recall immunity rather than residual immunity. Many short- and long-term immunity models have been proposed undertaking multiple scenarios and variable immune responses (13,31). What has been understood so far from direct analysis of infected patient data and vaccinated population is that there declining immunity and viral antigenic variation can lead to reinfection.
The severity of the reinfection in exposed population, either from infection or vaccinated, is another debatable issue. There have been direct and indirect evidences that severity of disease in reinfected patient is much less than the initial infection (19). It has been postulated that neutralizing antibody level as low as 3% of convalescent antibody titers level can provide 50% protection from severe infection. However, these findings need a large population-based study validation. This is a potential area of future exploration. The other important debate is about the effects of various types of vaccination in acquiring and sustaining long-term immunity.
Many studies and data results (including ours) have affirmed the notion that antibody titer postvaccination have almost similar declining pattern as we have seen in post-SARS-CoV infection. Based on these similarities, we can predict that vaccination will also provide limited term immunity not in years but in months. To add complexity to an already intricate situation is the fact that most of the vaccines are targeting spike proteins (8) and recent emergence of multiple mutations in spike protein (10) raise the question about the future efficacy of vaccinations. In the emerging scenario we need to explore the efficacy of vaccines against whole attenuated virus or spike protein.
It seems that the vaccines against live attenuated virus may provide better and lasting immunity against SARS-CoV-2 variants (22). However, long-term prospective studies need to be ensued to confirm this notion. This also need to be explored whether combination of vaccines provide more lasting immunity as compared with single one. Despite these entire questions one thing is becoming clearer with time that vaccines are producing neutralizing antibodies that last only a few months, and we may need boosters of vaccines to keep our population in protective range. The future course of pandemic will depend on better understanding of mechanisms to boost recall and residual immunity, and vaccine response and its administration regimens in view of rapid antigenic variation in virus.
Conclusion
In conclusion, our study reaffirmed that seropositivity to SARS-CoV-2 differs among gender, age, time from onset of symptoms, and positive PCR confirmation sample collection. Our data also confirm that some of the patients did not develop antibodies and remained seronegative to SARS-CoV-2 after sufficient time. The seronegative and seropositive SARS-CoV-2 patients had similar demographics and disease presentation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study received no specific funding from any funding agency in the public, commercial, or not-for-profit sectors.