
Abstract
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection causes coronavirus disease 2019 (COVID-19), which has affected hundreds of millions of people globally. The development of safe and effective vaccines represents an urgent demand. A total of 136 participants were recruited in this study, including 75 men and 61 women. The participants were divided into two groups: those who were virus naïve (never infected) and those who had recovered from COVID-19. Each group included individuals who received either the Pfizer–BioNTech BNT162b2 mRNA or the Oxford–AstraZeneca ChAdOx1 COVID-19 vaccine. Enzyme-linked immunosorbent assay (ELISA) was used to measure anti-S IgG antibody concentrations in sequential serum samples obtained before vaccine administration, after the first vaccine dose, and after the second vaccine dose. We compared the antibody responses of individuals with confirmed prior COVID-19 infection with those of individuals without prior evidence of infection. All participants who were previously infected with SARS-CoV-2 who received one dose of either the Pfizer–BioNTech BNT162b2 mRNA or the Oxford–AstraZeneca ChAdOx1 COVID-19 vaccine showed significant anti-S IgG antibody levels. No sex-related differences were observed when we compared antibody levels between men and women. In infection-naïve participants ≥60 years, a second vaccine dose was necessary to achieve higher levels of antibody when comparing the IgG antibody levels after receiving the first and second dose.
Introduction
The novel and the highly contagious severe acute respiratory syndrome coronavirus s (SARS-CoV-2) has spread worldwide, causing extraordinary global mortality rates (26).
The use of masks, physical distancing, serological testing, and other control measures has contributed to reducing viral transmission. However, these methods have been applied inconsistently and have been inadequate to prevent the spread of coronavirus disease 2019 (COVID-19), the disease caused by SARS-CoV-2 infection (37).
Several vaccine candidates at different phases of development are currently assessed (17). Vaccines are desirable to decrease the morbidity and mortality associated with COVID-19 (14). Several vaccines have been developed against SARS-CoV-2 and have demonstrated the pronounced ability to limit the effects of the infection (3). To date, six vaccines have been approved for emergency use. In our study, we investigated two: the Pfizer–BioNTech BNT162b2 mRNA vaccine and the Oxford–AstraZeneca ChAdOx1 vaccine. The Pfizer–BioNTech BNT162b2 mRNA vaccine induced a broad immune response, including SARS-CoV-2 spike protein (S)–specific neutralizing antibodies and poly-specific CD4+ and CD8+ T cells (30). The Oxford–AstraZeneca ChAdOx1 vaccine displayed an efficacy of 76% (59.3–85.9%) after a single standard dose (35). In addition, the Oxford–AstraZeneca ChAdOx1 vaccine showed an adequate safety profile and was efficient against symptomatic COVID-19 (34).
In this study, we aimed to investigate differences in the antibody levels induced after receiving one of these two vaccines, and compare the humoral immune response between COVID-19–naïve individuals and those who have recovered from COVID-19. We also investigated the immune responses in individuals ≥60 years to clarify the importance that this group receives two doses of the vaccine. We used enzyme-linked immunosorbent assay (ELISA) to measure the specific anti-S IgG serum levels in a sequential manner: prevaccine (as baseline antibody levels), after one dose of the vaccine, and after two doses of the vaccine.
Materials and Methods
Participants
A cohort of 136 participants was recruited for this study, including 75 men and 61 women. The participants were divided into two groups: the first group included virus-naïve individuals (noninfected, n = 62). This group was subdivided into two additional groups: those who received the Pfizer–BioNTech BNT162b2 mRNA vaccine (n = 35) and those who received the Oxford–AstraZeneca ChAdOx1 vaccine (n = 27). The second group included those who were recovered from a previous COVID-19 infection (n = 74). This group was also subdivided into two groups: those who received the Pfizer–BioNTech BNT162b2 mRNA vaccine (n = 51) and those who received the Oxford–AstraZeneca ChAdOx1 vaccine (n = 23). According to the Ministry of Health (MOH), the recommended time between the administration of the first and second dose of the Pfizer–BioNTech vaccine is 14 days, whereas the recommended time between the two doses of the Oxford–AstraZeneca vaccine is 3 months. Therefore, we encountered a small sample size for participants who received the Oxford–AstraZeneca vaccine.
We recorded the prior SARS-CoV-2 infection status for each patient and the timing relative to the first vaccine date using data extracted from MOH records and self-reported information.
Participants differed widely in age (18–87 years), comorbidities, and time since infection, which ranged from 6 to 15 months. Serum antibody titers were determined at the time of vaccination, 2–3 weeks after receiving the first and second dose of the Pfizer–BioNTech BNT162b2 mRNA vaccine, and 3 months after receiving the first dose and 2–3 weeks after receiving the second of Oxford–AstraZeneca ChAdOx1 vaccine.
Blood samples
At each time point, 5 mL venous blood was drawn from each participant. After serum separation, samples were maintained at −20°C until antibody analysis. Approval for the study was obtained from the research ethics committee of the College of Applied Medical Sciences, Taibah University (2021/96/117/MLT).
Enzyme-linked immunosorbent assay
An ELISA was applied to measure antibodies against the SARS-CoV-2 S protein, following a formerly designated procedure (21). In brief, the ELISA plate was coated with 100 μL spike protein antigen at 2 μg/mL (Sino Biological, China), and the plate was stored overnight at 4°C. The plate was then washed five times with washing buffer (phosphate-buffered saline containing 0.05% Tween-20), and 150 μL/well blocking buffer added and left for 1 h at room temperature. Before adding serum samples, they were diluted (1:100), and 100 μL diluted sample was added to each well. The plate was kept for 30 min at room temperature, washed five times, followed by the addition of 100 μL alkaline phosphatase-conjugated goat antihuman IgG (1:1,000) to each well and kept for 30 min at room temperature. Finally, after washing the plate five times, 100 μL/well of p-nitrophenyl phosphate substrate was added in the dark. After 30 min incubation, the stop solution was added at 100 μL. The optical density (OD) at 405 nm was measured through a microplate reader (ELX800; BioTek).
Statistical analysis
All statistical analyses were performed using GraphPad Prism software version 9 (GraphPad, San Diego). The antibody levels are presented as the mean ± standard error of the mean. To compare the mean age across the naïve and recovered groups, the Mann–Whitney U test was used. Fisher's exact test was used to assess the association between two categorical variables (e.g., sex differences across the naïve and recovered groups). Correlation between variables was calculated using the Pearson correlation. A p-value of <0.05 was considered significant.
Inclusion and exclusion criteria
Participants who were pregnant or diagnosed with laboratory-confirmed infections within the last 6 months were excluded, according to MOH guidelines. All healthy adult participants were included in the study.
Results
A total of 136 participants were included in the final analysis of this study. Mean age of participants was 44.9 ± 19.0 years. Over half of the sample were males (55.1%, n = 75). Sixty-three percent (n = 86) of the study sample was vaccinated with Pfizer. Participants in the naïve group were significantly older (49.8 ± 21.2 years vs. 40.8 ± 15.8 years, respectively, p = 0.012). Detailed description of the characteristics of the study participants is provided in Table 1.
Demographic Characteristics of Study Participants (n = 136)
Alpha = 0.05.
Measurement of anti-S IgG antibody in vaccinated, COVID-19–recovered patients
To investigate the humoral immune response induced after vaccine administration, we used ELISA to measure specific anti-S IgG antibody concentrations in the serum of vaccinated individuals. We compared the antibody levels of paired subjects prevaccine, after one vaccine dose, and after two vaccine doses. Interestingly, we found detectable anti-S IgG antibody levels in the majority of COVID-19–recovered patients prevaccine (85%, n = 63). No significant difference in vaccine-induced anti-S antibody levels was observed between the two vaccine types; therefore, we combined the results of the two vaccines. A significant increase in the specific anti-S IgG antibody concentration was detected after the first vaccine dose compared with the prevaccine (baseline) antibody concentration for both vaccines (Fig. 1, p < 0.001, n = 74). In addition, no significant difference was observed in the anti-S IgG antibody concentration measured after receiving the first dose compared with that after the second dose. We investigated the correlation between the baseline (prevaccination) antibody levels in COVID-19–recovered patients and antibody levels after first and second dose. We found a strong positive correlation between baseline levels and first dose and baseline levels and second dose, Pearson r = 0.71, p < 0.0001; Pearson r = 0.68, p < 0.0001, respectively (Fig. 2). This result supports the recommendation that COVID-19–recovered patients require only one vaccine dose.

Comparison of serum anti-S IgG antibody concentrations measured in COVID-19–recovered patients at different time points. A significant difference in the specific anti-S IgG antibody concentrations was found when we compared the levels prevaccine, after one vaccine dose, and after two vaccine doses (p < 0.001, n = 74). The antibody levels are shown as the mean ± SEM. SEM, standard error of the mean.
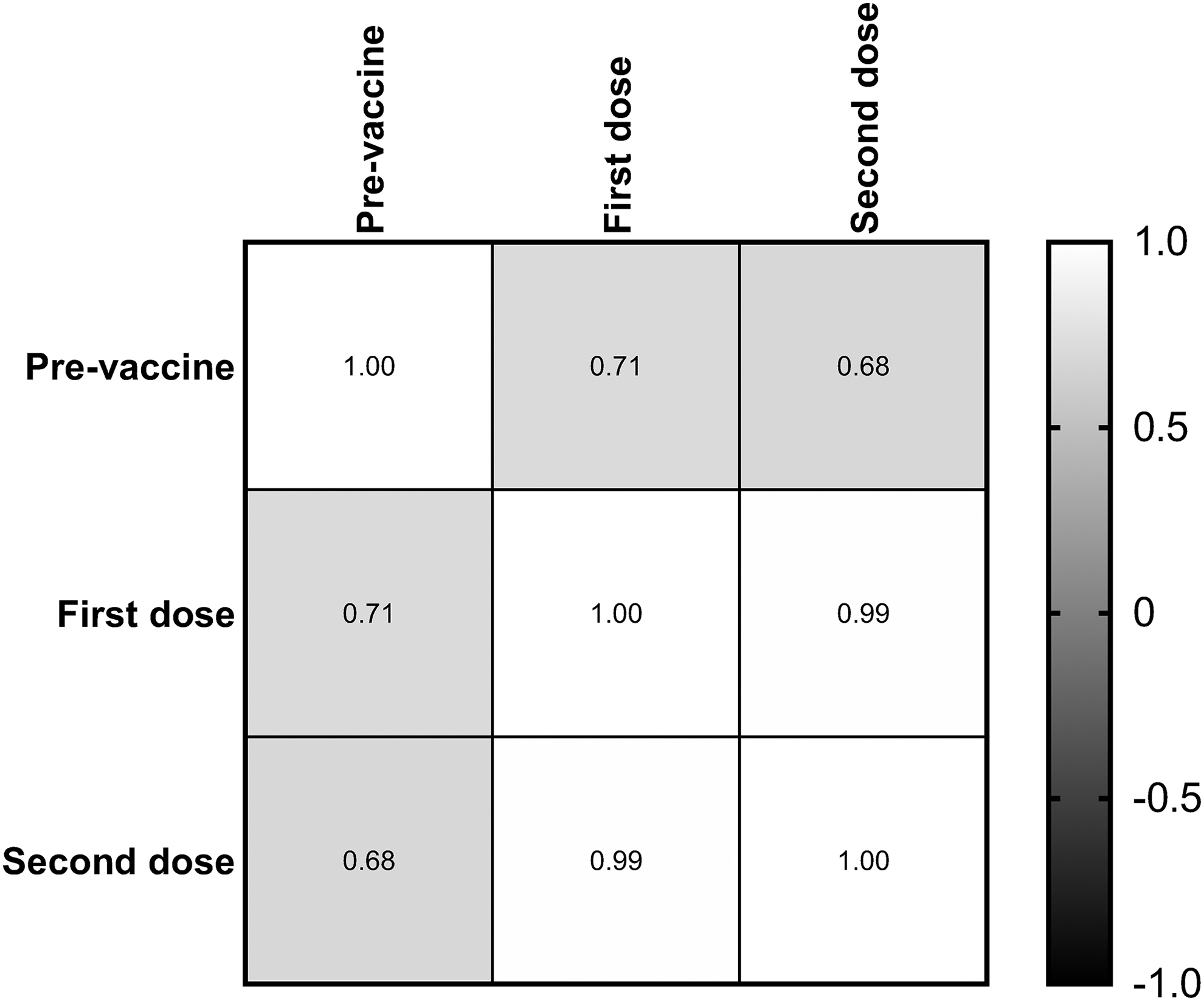
Correlation between the prevaccination antibody levels in COVID-19–recovered patients and that after first and second dose. A strong positive correlation observed between prevaccination antibody levels and first dose and second dose, Pearson r = 0.71, p < 0.0001; Pearson r = 0.68, p < 0.0001, respectively.
Comparison of anti-S IgG antibody concentrations between vaccinated COVID-19–recovered patients and vaccinated COVID-19–naïve individuals
To compare the humoral immune responses between the different participant groups, we measured the specific anti-S IgG antibody concentrations in the serum of vaccinated COVID-19–recovered patients and vaccinated COVID-19–naïve individuals. A significant (Fig. 3, p < 0.001, n = 136) increase in the anti-S IgG antibody concentration (mean OD = 1.47, n = 74) was found in vaccinated COVID-19–recovered patients compared with that in vaccinated COVID-19–naïve individuals (mean OD = 1.03, n = 62) after the first dose of both vaccines. Moreover, we found that anti-S IgG levels (mean OD = 1.03) in naïve individuals who received a single vaccine dose differ significantly from the anti-S IgG antibody (mean OD = 0.47, p < 0.0001) measured in the previously infected individuals at the baseline before receiving their first vaccine dose (Fig. 4).
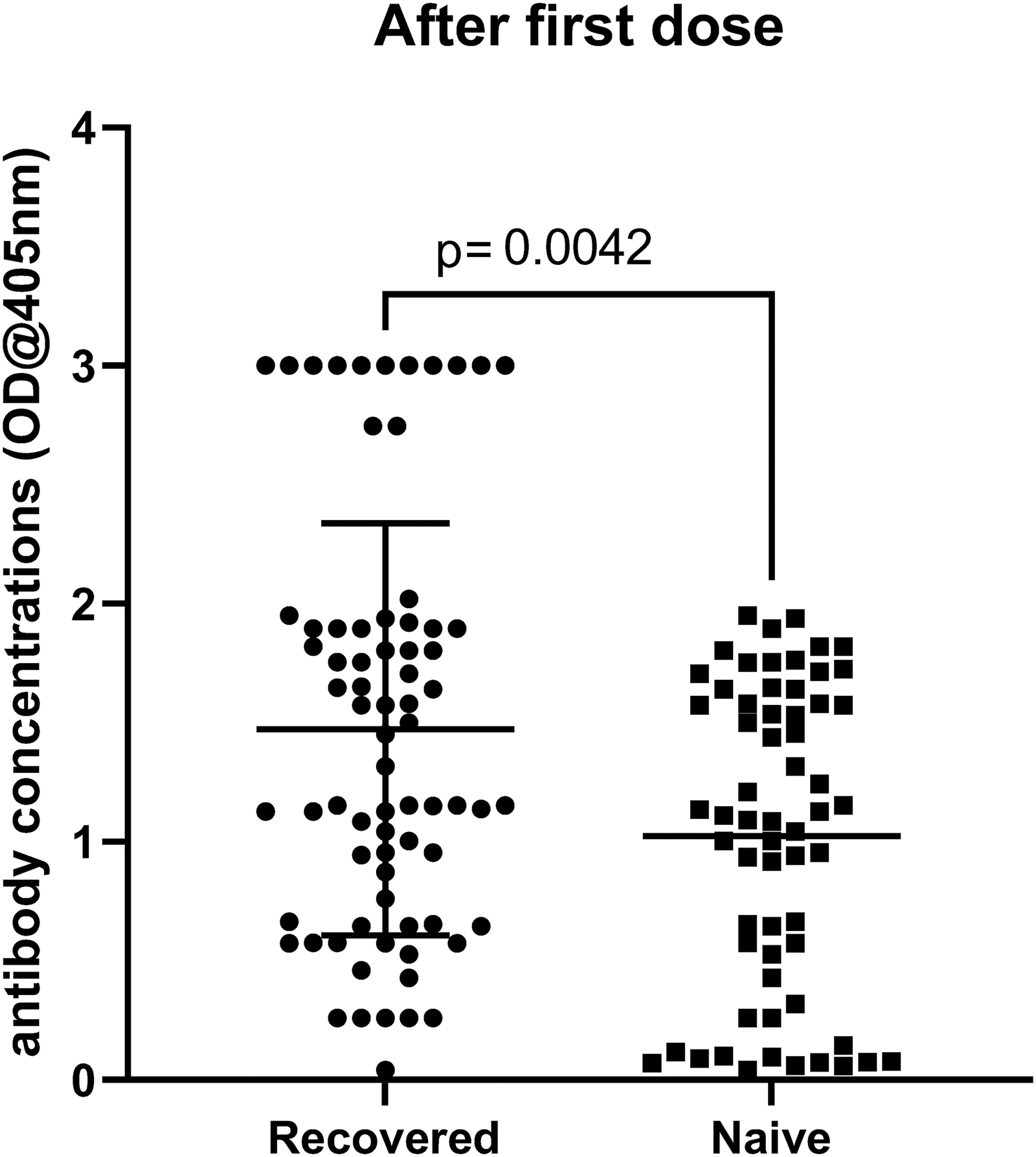
Comparison of serum anti-S IgG antibody concentrations measured in vaccinated COVID-19–recovered patients and COVID-19–naïve individuals after the first vaccine dose. Significantly (p < 0.001, n = 163) increased anti-S IgG antibody concentrations were observed in vaccinated COVID-19–recovered patients (mean OD = 1.47, n = 74) compared with those in vaccinated COVID-19–naïve individuals (mean OD = 1.03, n = 62). The antibody levels are shown as the mean ± SEM. OD, optical density.
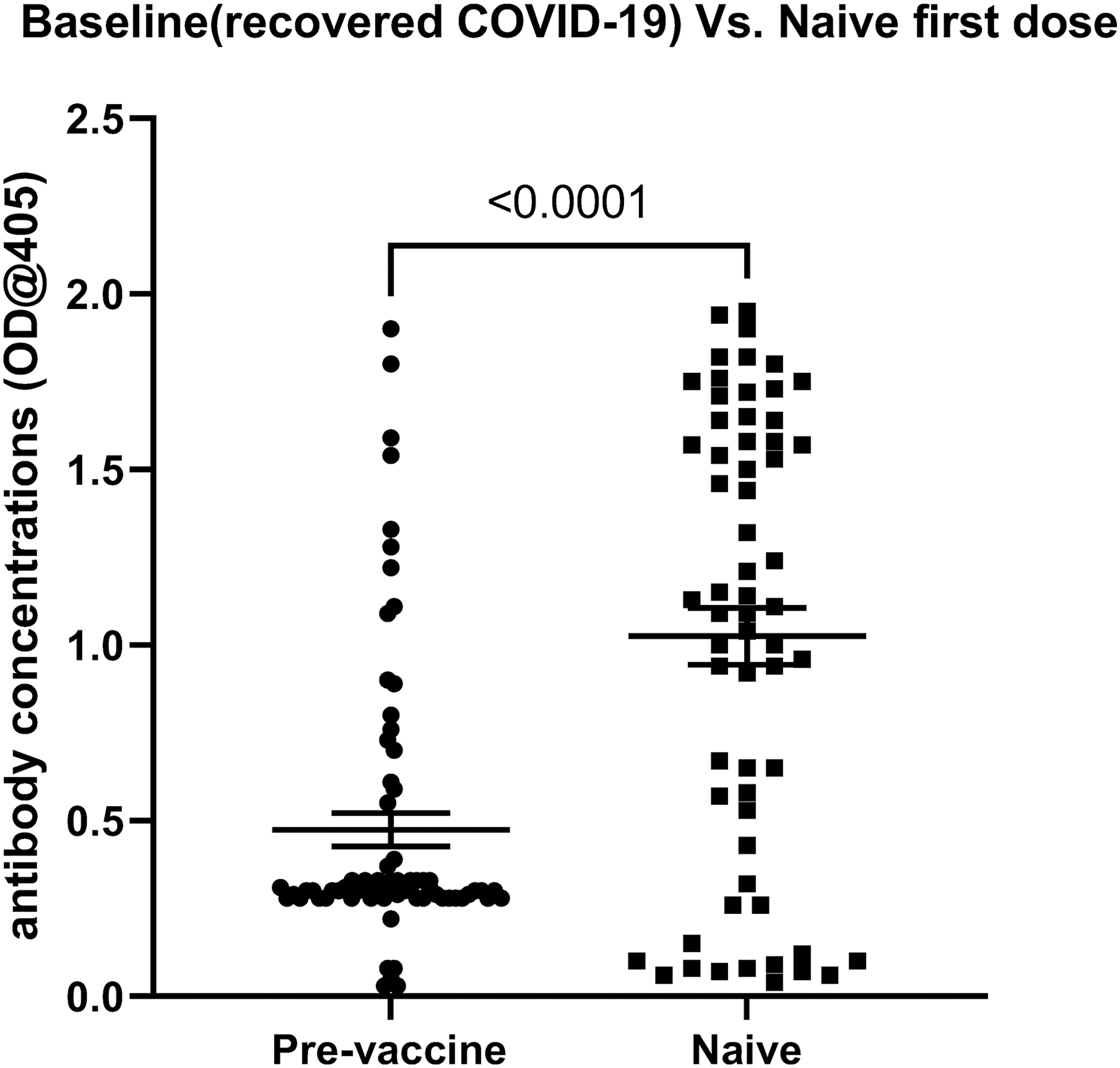
Comparison of serum anti-S IgG antibody concentrations measured in previously infected individuals before receiving the first dose (baseline) and those in infection-naïve people after a single vaccine dose. Significant difference in anti-S IgG levels was observed between infection-naïve people who received single vaccine doses (mean OD = 1.03, n = 62) and those previously infected individuals at baseline levels (mean OD = 0.47), n = 74, p < 0.0001).
Furthermore, the anti-S IgG levels did not differ significantly (Fig. 5) between previously infected individuals after a single vaccine dose (mean OD = 1.47, n = 74) and infection-naïve people after two vaccine doses (mean OD = 1.39, n = 62). The number of infection-naïve individuals who received two vaccine doses was only 46 of 62 (74%) due to the long time between the first and second doses of the AstraZeneca vaccine (3 months).
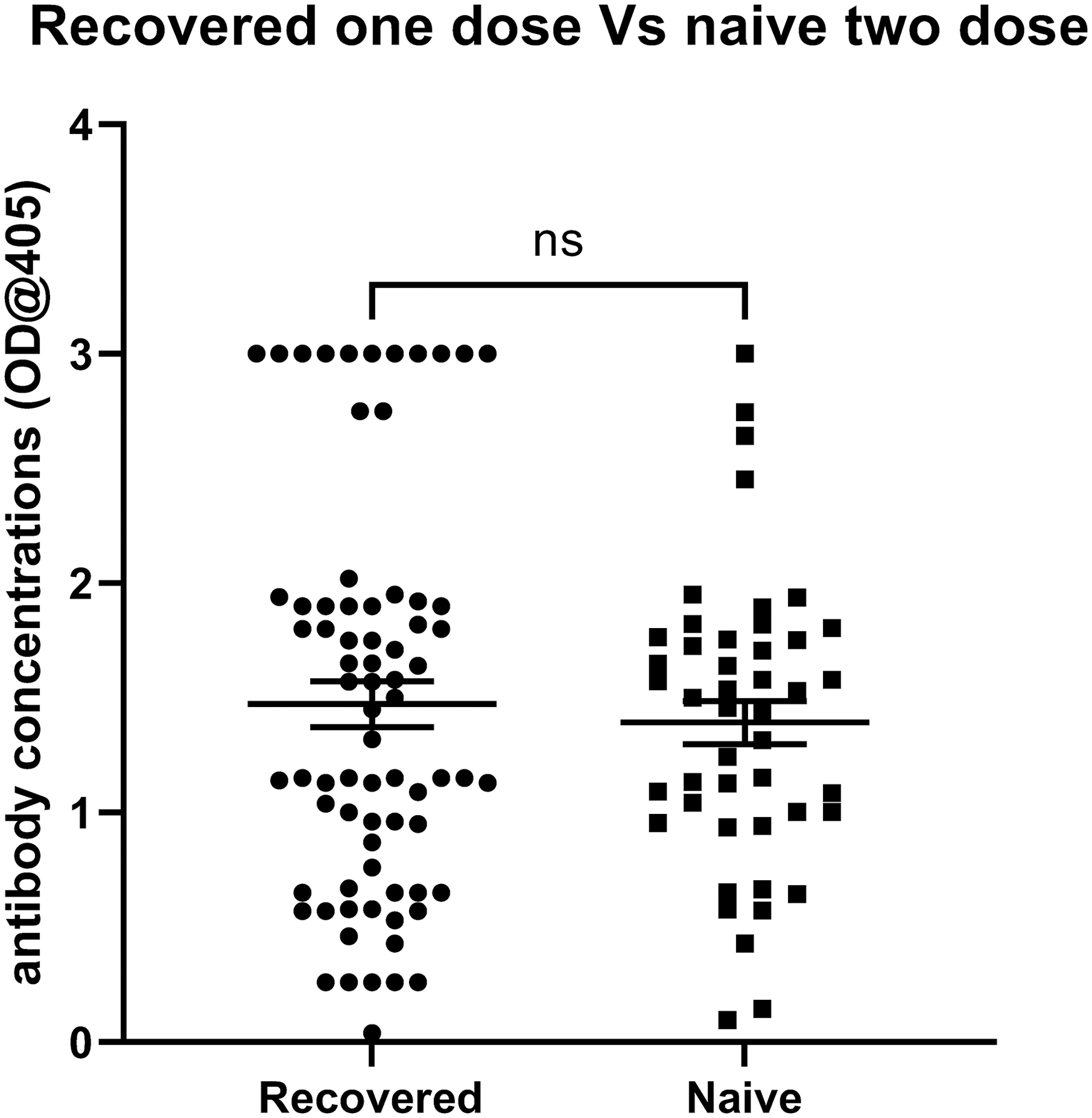
Comparison of serum anti-S IgG antibody concentrations measured in previously infected individuals after a single vaccine dose and those in infection-naïve people after two vaccine doses. No significant difference in anti-S IgG levels was observed between previously infected individuals after a single vaccine dose (mean OD = 1.47, n = 74) and those infection-naïve people after two vaccine doses (mean OD = 1.39, n = 62).
COVID-19–naïve individuals >60 years require two vaccine doses
To assess the vaccine dosing requirements among infection-naïve individuals ≥60 years, we compared the anti-S IgG antibody levels after the first and second vaccine doses. Within the COVID-19–naïve group (n = 62), 41 individuals (66%) were ≥60 years. A significant (Fig. 6, p < 0.001, n = 41) difference was observed between the anti-S IgG antibody concentrations of the same individuals after receiving the first dose compared with those observed after the second dose. No differences in the antibody response were observed between men and women. In addition, no age-dependent correlation in antibody levels was observed among all participants (data not shown).

Anti-S IgG antibody levels in vaccinated COVID-19–naïve individuals ≥60 years after two vaccine doses. A significant difference was observed when we compared the anti-S IgG antibody concentrations after receiving the first vaccine dose with those after receiving the second vaccine dose (p < 0.001, n = 41). The antibody levels are shown as the mean ± SEM.
Discussion
Developing immunity against SARS-CoV-2 is the best approach to taming the ongoing COVID-19 pandemic, protecting at-risk individuals from experiencing severe disease presentations, and hindering viral spread (27). Several studies have suggested that human immunity against the virus lasts from months to as long as 1 year postinfection (18,33,36). In addition, a recent study showed prolonged humoral and cellular immunity in COVID-19–recovered patients for a long time postrecovery (2).
SARS-CoV-2 vaccines are critically necessary, but the limited supply of these vaccines globally has led to the extensive implementation of cautious dosing plans, such as the use of a single vaccine dose among those with previous SARS-CoV-2 infections. In addition, whether the administration of a single dose rather than a double dose might be sufficient for certain groups of individuals has been explored, especially among those who have recovered from the past infection.
The permanence of vaccine-induced immunity relative to infection-induced immunity remains imprecise. We investigated this dispute by performing longitudinal assessments of the serum antibody levels in vaccine recipients with and without prior SARS-CoV-2 infection.
We clearly show that individuals with evidence of previous COVID-19 exposure require only a single vaccine dose to prime and recall their humoral memory immune response against the virus. Our results agree with those reported by several studies showing initial immune data, including the detection of measurable anti-SARS-CoV-2 antibodies in COVID-19–recovered individuals and reports that individuals who recovered from a previous infection develop a naturally acquired immunity that can be adequately boosted by a single vaccine dose (14,29). In addition, a recent study agreed with our findings, showing that in individuals with prior COVID-19 exposure, one vaccine dose was able to boost antibody levels to the high end of natural infection, regardless of the strength of response during the infection, with no further increasing observed upon receipt of a second dose (13). These data suggest that altered vaccination schemes among formerly infected people would continue to offer sufficient protection. Moreover, other studies have verified that vaccination induces all modes of the humoral response, resulting in serum neutralizing actions against variants of concern that are similar to the neutralizing actions against the novel Wuhan Hu-1 variant achieved after vaccination of infection-naïve persons (6,9).
Therefore, this would reflect the recall of memory humoral immune response upon priming of memory response by vaccination among those previously infected individuals, which led to antibody secreting memory B cell response to spike protein antigen. Thus, a single vaccine dose is needed to maximize immunity against the virus in those people. This result is in agreement with other studies conducted on health care workers (HCWs). That study showed after one dose, people with prior infection exhibited crossreactive cellular and humoral immunity to other variants differ from the one they were first infected with. On the contrary, HCWs who received a single dose of vaccine without prior infection presented reduced immunity against the other variants (28).
It is worth noting that immunity generated from natural infection and vaccine-generated immunity to SARS-CoV-2 are two different routes to protection (4). Although possible protection against reinfection resulted from taural infection has been reported (19), several studies concluded that immunity derived from natural SARS-CoV-2 infection combined with that induced from vaccination is leading to a notable synergy of the immune system “hybrid vigor immunity”; a larger-than-expected immune response rises (28,32).
We showed that anti-S IgG levels did not differ significantly between previously infected individuals after a single vaccine dose and infection-naïve people who received two vaccine doses. This result aligned with the results of a recent study performed on HCWs (7).
Interestingly, a recent study showed that sera obtained from both convalescent COVID-19 individuals and Pfizer vaccine recipients were able to neutralize the new Indian variant (B.1.617.2). The same study showed that sera from individuals who received just one dose of the AstraZeneca vaccine were also able to neutralize the same viral strain (24). These data collectively strengthen and support the need for the implementation of vaccination regimens by health authorities worldwide. Vaccination remains the best infection control measure for containing the emerging virus.
Due to immunosenescence, which refers to the weakening of the immune response with age and includes both quantitative and qualitative features of the immune response, the efficacy profiles of vaccines are expected to be reduced among older people (31). The effectiveness of vaccines in older individuals has not been well studied (11). Therefore, we investigated the humoral immunity that developed in response to vaccine doses in participants aged ≥60 years. We showed that older individuals required two vaccine doses to achieve higher antibody concentrations. Therefore, we recommend that health authorities consider this age group for the receipt of two vaccine doses due to their weakened immune system and their vulnerability to infection. Alterations of the immune system caused by aging affected the adaptive and innate immune cell components. It was also linked to the functional weakening of T and B lymphocytes. The most protruding aspect includes a reduction in the quantity of naïve cells due to thymic involution (16); moreover, a rise in memory/exhausted T cells and a decrease in B cell progenitors in the bone marrow (1). Recent studies relating patients with COVID-19 have perceived fall in peripheral lymphocytes (10,12), including lessened circulating CD4+ as well as CD8+ T cells (5,15,23).
Generally, we showed that individuals who have recovered from prior infection with SARS-CoV-2 displayed vaccine-induced antibody responses after the receipt of a single vaccine dose at similar levels to those observed among infection-naïve participants after two vaccine doses. Our findings in the current cohort aligned with the results of smaller studies, which showed higher levels of anti-S antibodies after a single mRNA vaccine dose among formerly infected persons relative to infection-naïve individuals (22,25). Therefore, our data suggest that a single dose of either the Pfizer–BioNTech or Oxford–AstraZeneca vaccines is adequate to boost the immune systems of individuals with previous SARS-CoV-2 infections. A recent study showed that neutralizing antibody concentrations against one of the SARS-CoV-2 variants of concern, B.1.351 (beta), in individuals who were previously infected with a different viral strain were ∼100-fold higher after vaccination than after infection alone and ∼25 times higher than after infection alone (4).
Interestingly, we found that individuals who were previously exposed to the virus showed no significant increase in antibody levels after receiving the second vaccine dose. Our results agree with the recommendations of several published studies suggesting the administration of a single dose to individuals who have recovered from the disease (8,29).
This study has some limitations. First, this study included a small sample size of vaccine recipients. Second, the number of samples from individuals who obtained two doses of the AstraZeneca vaccine was especially small, and we wished to take more blood samples in a sequential manner every 2–3 weeks, but that was not applicable. Third, the influence of vaccines on cellular immunity has not been investigated, which might present greater crossreactivity than the humoral response. Fourth, longer term follow-up can provide additional data regarding the interval of immunity that develops in response to a single vaccine dose compared with two vaccine doses. Last, due to lack of access to a biosafety level 3 (BSL3) facility, we could not perform antibody neutralization assays to verify the functionality of the anti-S antibodies induced by the vaccines in our study. We should mention that due to the lack of enough clinical data regarding the disease severity in those recovered patients, we could not be able to compare between antibody levels among this group. However, we have recently found significantly higher anti-S IgG antibody levels in hospitalized severe SARS-CoV-2 patients compared with those mild and moderate patients (20).
In conclusion, our results suggested that two doses are essential to induce a sufficiently strong humoral immune response in infection-naïve individuals, whereas one dose has the maximal effect in individuals with previous infection exposure.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.