
Abstract
Early evidence during the coronavirus disease 2019 (COVID-19) pandemic indicated high levels of interleukin (IL)-6 in patients with severe COVID-19. This led to the off-label use of tocilizumab (TCZ) during the first wave of the pandemic. While the monoclonal antibody blocks IL-6 pathway, its effect on other inflammatory cytokines remains poorly described. To better understand the effect of TCZ on the biological inflammatory profile, we monitored a large panel of inflammatory cytokines in critically ill COVID-19 patients receiving off-label TCZ. Twenty-three patients with polymerase chain reaction-confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection were included in the study, among which 15 patients received TCZ and 8 patients did not. Serum samples were collected for 8 days, before and following TCZ administration or hospital admission for the control group. Serum profile of 12 cytokines (IL-1β, -2, -4, -6, -8, -10, -12, -13, -17, -18, tumor necrosis factor α (TNF-α), interferon-gamma (IFN-γ), and sIL-6R were assessed in these two groups.
Although the increased IL-6 concentrations after TCZ infusion were expected, we observed an unexpected increase in IL-1β, -2, -4, -10, -12p70, -18, and sIL-6R levels in the treated patients with maximal values reaching 2 to 4 days after TCZ. In contrast, no change in cytokine levels was observed in the control group. Our results suggested that some inflammatory pathways escape IL-6R blockade and even appeared amplified. This finding highlights an old observation of the anti-inflammatory effects of IL-6 as already suggested over 20 years ago.
Clinical Trial Registration number: NCT04346017.
Introduction
More than 30 years have passed since discovery, cloning, and understanding of the biological role of interleukin-6 (IL-6) (3). The IL-6 signaling and its role in pathologies is currently well established and follow two different pathways involving the IL-6 receptor (IL-6R) and the glycoprotein130 (gp130) (3). The role of IL-6 dysregulation in various autoimmune and inflammatory diseases has been the rationale to target its pathway and led to the first antibody designed to block IL-6R, Tocilizumab (TCZ) (6,12,23).
TCZ is a humanized monoclonal antibody directed against both the soluble form and membrane-bound IL-6R and blocks the IL-6 signal pathway through competitive inhibition of the receptor (12,20,23,31). It was first introduced in Japan in 2008 followed by the European Union in 2009, under the name of RoActemra®, and the United States in 2010 as Actemra®, now licensed for use in more than 100 countries for treatment of rheumatoid arthritis, juvenile idiopathic arthritis, or Castleman's disease (6,23,31).
From the beginning of the current pandemic, TCZ has been proposed in an off-label application to manage critical cases of coronavirus disease 2019 (COVID-19) and has quickly been included in the Chinese treatment guidelines (22,32). Numerous clinical trials are ongoing to determine the most relevant target and therapeutic strategy in the management of COVID-19. TCZ is the purpose of ongoing nationwide (COV-AID), European (TOCIVID-19 in Italy, TOCOVID-19 in Spain), and international clinical trials (COVIDOSE in United States, TACOS in China), registered on
In this context, we aimed to monitor IL-6 and several other inflammatory cytokines in critically ill COVID-19 patients before and during 8 days following anti-IL-6 therapy administration.
Materials and Methods
Study design
Overall, 23 patients admitted to the CHU Saint-Pierre and Brugmann (Brussels, Belgium) between 18 March and May 6, 2020 with a confirmed diagnosis of COVID-19 by a real-time polymerase chain reaction assay on a nasopharyngeal swab were enrolled in our study.
Patients were classified as severe or critical according to WHO guidelines 2020 as follows: Severe cases that met any of the following criteria: respiratory distress (≥30 breaths/min); oxygen saturation ≤93% at rest; arterial partial pressure of oxygen (PaO2)/fraction of inspired oxygen (FiO2) ≤300 mmHg (1 mmHg = 0.133 kPa). Critical cases that met any of the following criteria: respiratory failure and requiring mechanical ventilation; shock; other organ failure that requires intensive care unit (ICU) care.
Demographics data and clinical outcomes were collected from the medical file.
Fifteen patients received TCZ and were further divided in two groups, patients who survived (TCZ/S, n = 6) and nonsurvivors (TCZ/D, n = 9). We performed serum sample collection and cytokine measurements before TCZ infusion, day 0, and during the 8 days following. In parallel, cytokine levels were measured at the admission, time identified as day 0, and during the following 8 days in 8 COVID-19-positive patients who did not receive TCZ (control group, NO TCZ). Each cytokine was measured three times (median, range 2–5) during the follow-up time post-TCZ or postadmission (Table 1).
Demographic and Clinical Characteristics
Data are expressed as median [min–max] or n (%).
ICU, intensive care unit; ns, non significant; TCZ, tocilizumab.
In the time frame of this study, all affected patients were treated with the institutional standard pharmacological protocol, including 2,400 mg of hydroxychloroquine in monotherapy over 5 days (4). When given, TCZ was administrated in a single intravenous dose of 8 mg/kg, except for one patient who benefitted from a second one 3 days after. Patients did not receive corticosteroids or others immunomodulatory drugs.
The study was approved by the local Ethics Committee of the CHU Brugmann (CE 2020/63) and Saint-Pierre (Reference CE/20-03-05) Hospitals and registered on
Cytokine measurements
The levels of 12 cytokines (IL-1β, -2, -4, -6, -8, -10, -12, -13, -17, -18, tumor necrosis factor α [TNF-α], and interferon-gamma [IFN-γ]) and of the sIL-6R were assessed in the serum of patients using an electrochemiluminescence plate-based assay (MSD, Meso Scale Discovery, MD).
Laboratory findings
Circulating inflammatory biomarker levels (C-reactive protein [CRP], procalcitonin [PCT], ferritin, fibrinogen, d-dimers, and neutrophils) were measured before TCZ administration and for 8 days following the treatment or admission using a Cobas 8000 Platform (Roche Diagnostics), a Sysmex CS-5100 analyzer (Siemens Healthcare Diagnostics), and a Lumipulse G600II analyzer (Fujirebio).
Statistical analysis
Demographic data were analyzed using the nonparametric Kruskal–Wallis analysis of variance, followed by a Dunn's multiple comparison test. Categoric variables were compared with the Fisher's exact test.
Linear mixed models were used to analyze the longitudinal evolution of cytokine levels (29). For all models, the next effects were tested to model the evolution of biological variables through time: a group effect and a time effect. When the residuals of the model were not normally distributed, we used the bestNormalize R package to transform the outcome and reported the results of this last linear mixed model.
Results
Fifteen patients receiving TCZ (survivors, TCZ/S group, n = 6 and nonsurvivors, TCZ/D group, n = 9) and eight controls were followed for cytokine measurements.
Demographic data are reported in Table 1. There was no statistically significant difference according to the sex, the age, and the state of illness between subgroups. The median delay time between symptom onset and hospital admission was of 7 days in the three groups. The median (min–max) time before administration of TCZ was of 9 days (5 –23) since symptoms emergence, 5 days (1 –10) since hospital admission and 3 days (1 –7) since ICU admission, without significant difference between the TCZ/S and TCZ/D group (Table 1).
Cytokine measurements assessed in each patient are listed in Table 2.
Cytokine Measurements
Cytokine levels (pg/mL) measured in each patient (n = 23), before TCZ administration or at the admission (day 0) and during the following 8 days.
IFN-γ, interferon-gamma; TNF-α, tumor necrosis factor α.
The baseline and maximum levels obtained for each cytokine were compared among patient groups and reported in Table 3. No difference was observed in cytokine baseline levels between groups, except for IL-2 and IL-6, which were found to be higher in treated patients before treatment administration. IL-6 concentrations rapidly raised and reached significantly higher maximum levels in TCZ-treated patients compared with the control group.
Cytokine Profiles and Comparison Among the Three Groups (Baseline Levels, Maximal Values, Time Associated with This Maximum and Time2 Effect)
Comparison of cytokine baseline levels (pg/mL), maximal values (pg/mL), time associated with this maximum (days), and time2 effect among the nontreated patients (NO TCZ, n = 8), treated survivors (TCZ/S, n = 6), and treated nonsurvivors (TCZ/D, n = 9).
Statistically significant differences are presented in bold.
Moreover, significantly higher levels of IL-1β, -2, -4, -6R, -10, -12p70, and -18 were also observed in patients receiving TCZ. These levels were elevated in both the TCZ/S group and the TCZ/D group, except for IL-4 and -10, which reached significantly higher values only in the TCZ/D group when compared with the control group and for sIL-6R. However, no statistically significant difference was observed in maximal values between the TCZ/S group and the TCZ/D group for the different cytokines on our studied population (Table 3).
Cytokine profiles, assessed before and 8 days after TCZ administration, are shown in Figure 1. Longitudinal changes in cytokine levels were analyzed using a linear mixed model and showed a significant transient effect (time2 effect) over time with a peak value that reached around day 2 to 4 for IL-2 (only in TCZ/D), -4, -6, -6R (only in TCZ/S), -12p70, -13, and TNFα (only in TCZ/D). Furthermore, the time associated with the maximal value for all cytokines was not significantly different among the three subgroups (TCZ-treated and nontreated patients) (Table 3).
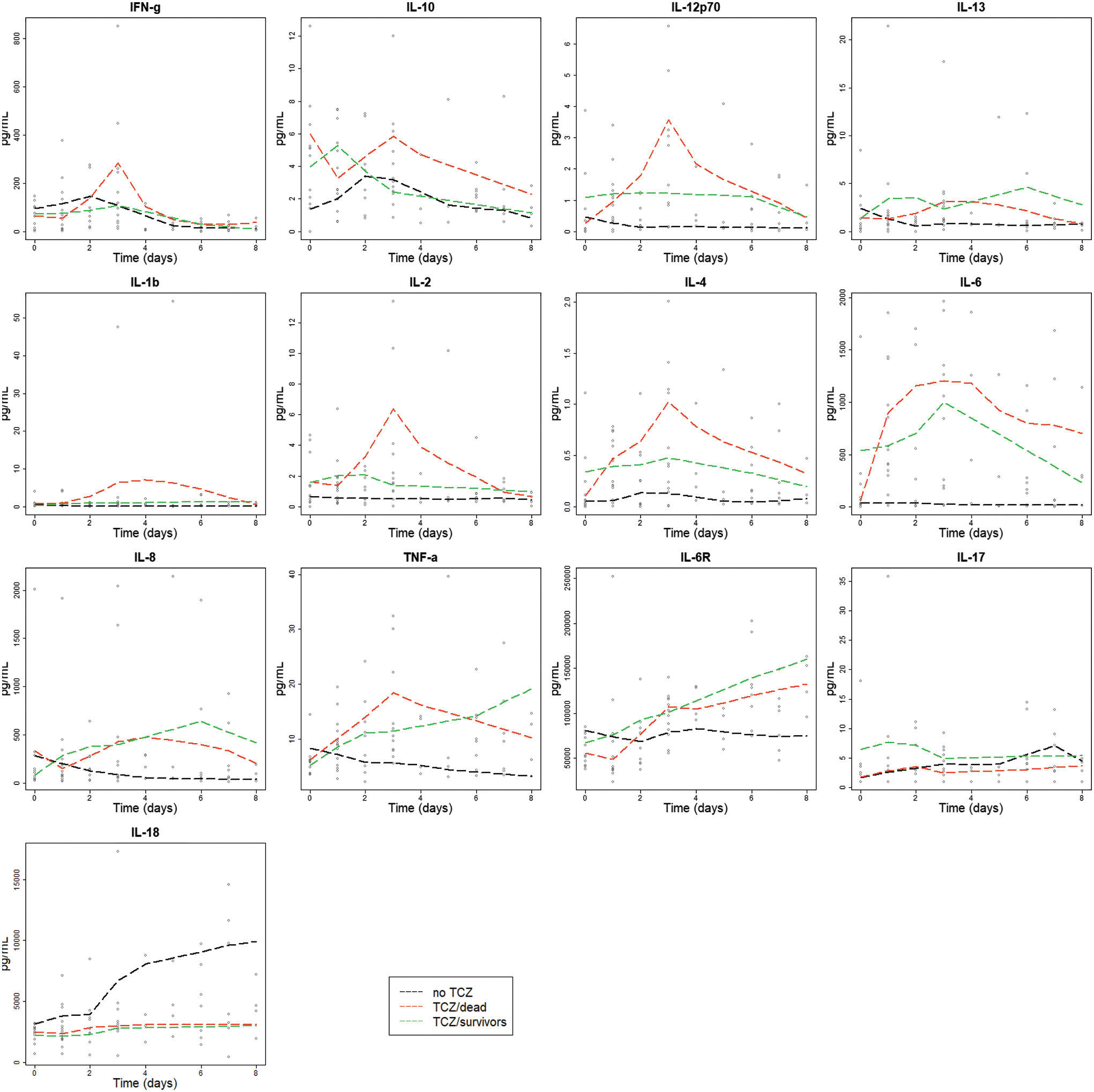
Kinetics of cytokines in the three groups. Kinetics of IL-1β, -2, -4, -6, -8, -10, -12, -13, -17, -18, TNF-α, and IFN-γ in nontreated (NO TCZ, n = 8) versus treated survivors (TCZ/S, n = 6) or treated nonsurvivors (TCZ/D, n = 9). Results were measured between day 0 and 8 after TCZ infusion, or from hospital admission for the NO TCZ group. IL, interleukin; TCZ, tocilizumab; TNF-α, tumor necrosis factor α. Color images are available online.
The laboratory parameter baseline results revealed high levels of inflammatory markers, including CRP, ferritin, fibrinogen, and neutrophils, for all patients enrolled. Most of them remained stable in the nontreated group during the 8 days of follow-up. In the treated patients, CRP and fibrinogen levels improved and decreased toward the normal range, whereas neutrophils and ferritin remained high above normal values, and d-dimers even increased in the TCZ/D group (Fig. 2).
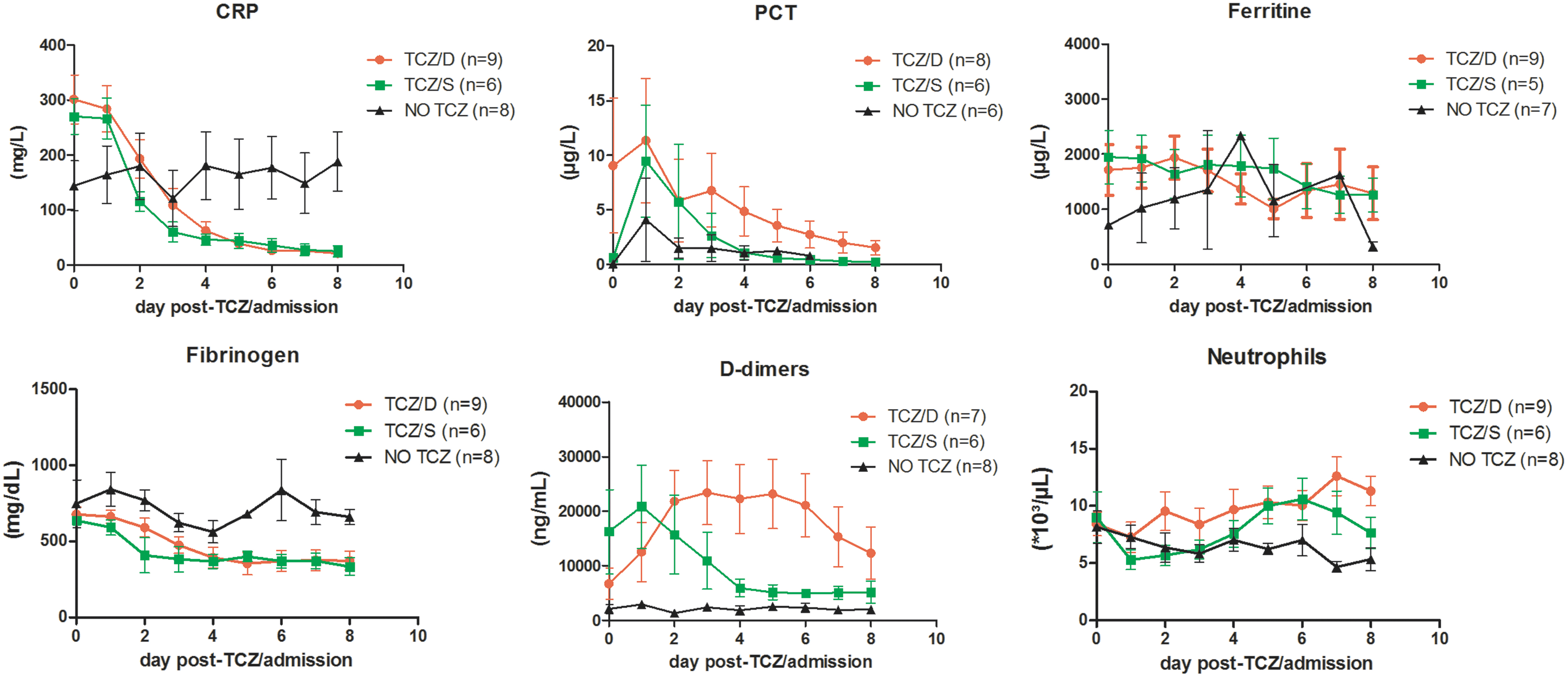
Tocilizumab effect on circulating inflammatory biomarkers. Kinetics of CRP, PCT, ferritin, fibrinogen, d-dimer and neutrophil* levels in nontreated (NO TCZ, n = 8) versus treated survivors (TCZ/S, n = 6) and treated nonsurvivors (TCZ/D, n = 9). Results were measured between day 0 and 8 after TCZ infusion, or from hospital admission for the NO TCZ group. Results are presented as mean ± SEM. *Not all patient received all relevant laboratory tests. CRP, C-reactive protein; PCT, procalcitonin; SEM, standard error of the mean. Color images are available online.
Discussion
The cytokine profile of some critically ill COVID-19 patients shares similarities to those observed in cytokine release syndromes, characterized by an increased production of cytokines followed by a dysregulation of tissue repair mechanisms, damages and, finally, multiple organ failure leading to death (5,19,28,32).
Recently, levels of IL-6 have been included to the criteria for COVID-19-associated hyperinflammatory syndrome (30). Cytokines IL-6 and TNF-α have revealed to predict severity and mortality in COVID-19 (9). Although the mechanisms leading to inflammation in COVID-19 are still poorly understood, immunomodulatory agents have rapidly been proposed and included into various clinical trials, most of them focused on IL-1β, -6, -8, and TNF-α (6,9,14). Azmy et al. suggested that TCZ was unable to calm the inflammatory storm focusing on increased IL-10 and IL-2 receptor levels in patients receiving TCZ (2). However, the profile of a large panel of cytokines immediately after TCZ administration is yet unknown.
In this study, we explored the longitudinal cytokine profile in critically ill severe acute respiratory syndrome coronavirus 2 (SARS-CoV2)-infected patients receiving anti-IL6R therapy. We focused on the trend of 12 inflammatory cytokines (IL-1β, -2, -4, -6, -8, -10, -12, -13, -17, -18, TNF-α, and IFN-γ) and of the sIL-6R in the treated group compared with patients without anticytokine therapy.
Regarding the longitudinal evolution, the levels of most of cytokines remained stable over time following the disease course in the nontreated group, supporting previously reported results (9). In contrast, IL-18 levels progressively increased during the follow-up in untreated patients. It is noteworthy that IL-18 has also been recommended as a biomarker for secondary hemophagocytic lymphohistiocytosis (8,13). However, whether the increase in IL-18 levels observed in a few COVID-19 patients is a witness of a SARS-CoV2-induced HLH remains questionable.
The significant difference observed for the baseline levels of IL-6 and found only in TCZ-treated survivors may indicate that a high IL-6 concentration before treatment is required to benefit from TCZ as observed by Galván-Román et al. (11).
In the treated patients, we confirmed the expected rapid increase of IL-6 levels after TCZ injection followed by a gradual decrease (9). This can be explained by the blockage of the IL-6R, resulting in the accumulation of IL-6, which can no longer bind to its receptor and thus cannot be internalized through IL-6R-mediated consumption (14,31). This elevation also reflects the endogenous IL-6 production related to the disease activity (18).
In parallel, therapeutic inhibition of the IL-6R blocks the IL-6 signaling pathway but not the generation of sIL-6R, which is unaltered in TCZ-treated patients (20). The binding of TCZ to the IL-6R and accumulation of the resulting TCZ/sIL-6R complexes might explain increased levels of IL-6R observed after TCZ injection as compared with the nontreated group since TCZ bound to sIL-6R has a higher molecular weight than sIL-6R alone and is therefore cleared more slowly from the circulation (Table 3).
More surprisingly, we also observed a transient but significant increase in proinflammatory cytokines: IL-2, -4, -6-12, -13 (only in TCZ/D), TNF-α (only in TCZ/D), and sIL-6R (only in TCZ/S), for patients receiving a single dose of IL-6R blockade therapy. This observation highlights that neutralization of the IL-6R pathway is not sufficient to completely prevent activation of all the inflammatory pathways. Our findings are in accordance with the Del Valle et al. (9) previous observations on TCZ effect on IL-6 and IL-8 levels, whereas we diverge about the profile of TNF-α presenting a transient increase following the treatment injection, as seen only in the TCZ/D group in our study (Table 3).
IL-6 signal transduction acts through both a soluble and a membrane-bound receptor involved in two different pathways with divergent functions: the classical one promoting anti-inflammatory responses and the trans-signaling pathway responsible for the proinflammatory effects (3,12,20,31,32). TCZ acts by blocking both and thus inhibits proinflammatory but also potentially protective anti-inflammatory IL-6-mediated responses (12).
In contrast to cytokines, circulating inflammatory biomarkers such as CRP, fibrinogen, and ferritin baseline levels were elevated but decreased shortly after TCZ administration, without any difference between survivor and nonsurvivor patients (Fig. 2). These laboratory findings corroborate with previous results of Toniati et al. (28), with a decrease of these biomarkers toward a normal range associated with a clinical improvement 10 days after TCZ. While the ferritin profile was stable over our follow-up time in all three groups, it remained above normal values. However, we noticed an increase in neutrophil and d-dimer levels in our treated population and especially in nonsurvivors, comforting that IL-6 pathway blockers act only partially on the inflammatory cascade.
Even if no statistically significant difference was observed in maximal values between the TCZ/S and the TCZ/D group for the different cytokines in our population, trends in increased levels of IL-12p70, IL-2, IL-4, IL-6, and TNF-α were noted in the TCZ patients who died. This group of patients also presented the highest d-dimers, neutrophils, and PCT at day 8 compared with other groups. Such a constellation allows supposition that disseminated intravascular coagulation with multisystem failure could have contributed to death in these patients and that TCZ failed to prevent this fatal issue.
In summary, on the one hand, some inflammatory biomarkers rapidly decreased in the 8 days following TCZ infusion and, on the other hand, levels of several inflammatory cytokines significantly increased after a single dose of TCZ, suggesting a partial effect of the drug on hyperinflammation. These findings enhance the pivotal role of the IL-6 pathway: it may have a downregulatory effect on several cytokines that disappears by blocking the binding of IL-6 to its receptor and thus resulting in an increased production of these cytokines.
This incomplete inhibition of the inflammatory response, shortly after one dose of TCZ, might explain why most clinical trials failed to meet their primary endpoints of improved clinical status in COVID-19 patients (14,25). Our hypothesis is in accordance with the findings of Angriman et al., suggesting that this rebound expression of non-IL-6 cytokines could be detrimental, and might reflect an activation of collateral inflammatory pathways (1).
The increased levels of several inflammatory cytokines observed after a single TCZ administration in SARS-CoV-2 severely ill patients might also explain why immunomodulatory therapies with a wider range of targets proved to be more efficient, as suggested by the benefit of dexamethasone use in the preliminary results of the RECOVERY study (26). Promising recent data suggest that, combined to dexamethasone, TCZ could decrease the use of mechanical ventilation and the mortality, compared with standard of care (10,17,24,26,31,21).
Finally, in January 2021, the REMAP-CAP trial released preliminary evidence that tocilizumab could reduce fatalities among severely ill Covid-19 patients having or have completed a course of corticosteroids, and the drug was added to the United Kingdom recommended list for COVID-19 treatment (27). The nationwide Belgian COV-AID trial that compares combination of anti-IL-6 and IL-1 blockade in patients with COVID-19-associated hyperinflammatory syndrome will provide an answer about the clinical benefit of targeting multiple inflammatory pathways (16).
Our work features several limitations and particularly the limited number of patients included in the study, which may explain why we could not observe a difference between survivor and nonsurvivor TCZ-treated patients.
To our knowledge, we are the first to fully investigate the kinetics of this wide panel of cytokines before and after anti-IL6R blocker while the recently published data focused on IL-6, IL-10, and IL-2R levels after TCZ administration (2).
Besides the predictable peak of IL-6 concentration, we highlight an immune dysregulation worsening in patients receiving TCZ, as evidenced by the increase of several other cytokines, among them some proinflammatory and potentially harmful ones. This observation reinforces the need to use another immunomodulatory strategy in critically ill COVID-19 patients, particularly for patients with low IL-6 baseline levels.
Our findings suggest that the IL-6 inhibition alone may not be sufficient to completely block the hyperinflammatory state described in critically ill COVID-19 patients and may constitute an argument pleading for a treatment that target more broadly the various pathways of inflammation. These biological results could explain why most of clinical trials using TCZ alone failed to meet their primary endpoints of improved clinical status, whereas studies in which a positive effect of TCZ has been observed included corticosteroids (4,10,22,27).
Footnotes
Authors' Contributions
Concept and design: C.N., F.C., F.P., and J.S. Analysis and interpretation of cytokine data: C.N., F.C., and J.-F.F. Patient enrollment and collection of clinical data: N.D., E.M., D.D.B., and T.B.-H. Writing original draft: F.P. and C.N. All authors critically reviewed the article.
Acknowledgments
The authors thank Asma Benslimane and Thao Tran Thi Thanh for their technical help. N.D. is a postdoctorate clinical master specialist of the F.R.S-FNRS.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.