
Abstract
Interferon (IFN) and nucleoside (nucleotide) analogs (NAs) are two effective antiviral drugs for chronic hepatitis B (CHB). More and more evidence shows that the combination of the two drugs can better inhibit viral replication and even achieve clinical cure. IFN intermittent therapy is also considered to be an important measure to resolve IFN fatigue when hepatitis B surface antigen (HBsAg) decline appears stagnated during IFN-based antiviral therapy. A 36-year-old male NA-experienced patient with hepatitis B e antigen (HBeAg)-positive CHB was admitted to our hospital. After a poor response to tenofovir disoproxil fumarate (TDF) monotherapy for 1 year, the patient was treated with pegylated interferon alfa-2a combination therapy and finally achieved HBsAg clearance. During the treatment and follow-up, HBsAg, HBeAg, hepatitis B virus (HBV) DNA, and serum alanine aminotransferase, etc. were monitored every 3 months. Between weeks 58 and 71 of combination therapy, IFN was discontinued because of a slow decline in HBsAg, and TDF alone was used for maintenance therapy. Complete virological response, HBeAg and HBsAg seroconversion were observed at weeks 44, 96, and 122, respectively. After 24 weeks of consolidation therapy, HBsAg, HBeAg, and HBV DNA were consistently negative, and hepatitis B surface antibody was 729.30 mIU/mL at week 146 of the combination therapy, then we stopped drugs. Following up after 28 weeks of cessation therapy, the patient still remained clinically cured.
Introduction
China is a highly endemic area of hepatitis B virus (HBV) infection, with ∼70 million people being infected, including 20–30 million cases of chronic hepatitis B (CHB) (4). Antiviral therapy is the most important measure to postpone the disease progression and improve the long-term prognosis of CHB patients. The ideal endpoint of antiviral therapy in CHB patients is the elimination of hepatitis B surface antigen (HBsAg) to achieve lasting immune control and clinical cure (4).
Interferon (IFN) and nucleoside (nucleotide) analogs (NAs) are two effective antiviral drugs for the treatment of CHB. Although NAs can effectively inhibit viral replication and make most people achieve complete virological response, there are still some patients who only achieve partial virological response after NAs treatment, which cannot completely prevent disease progression. Meanwhile, the hepatitis B e antigen (HBeAg) serological transformation rate of NAs is not satisfying, and it is more difficult to obtain the HBsAg disappearance (5). Therefore, how to make the patients with poor NAs response continue to obtain complete virological response, durable immune control, and even higher treatment goals are still problems to be solved in clinical treatment. IFN has the dual function of antiviral action and immunoregulation. Many studies (1,9,10,16) based on the combination therapy of pegylated interferon alfa (Peg-IFNα) and NAs indicated that compared with monotherapy, combination therapy played a stronger role in reducing the number of HBV-infected hepatocytes and load of covalently closed circular DNA (cccDNA), which could acquire a higher clearance rate of HBsAg. A typical case of a tenofovir disoproxil fumarate (TDF)-treated HBeAg-positive CHB patient combined with Peg-IFNα-2a obtaining clinical cure is reported as follows, hoping to provide help for clinical diagnosis and treatment of CHB patients with poor response to NAs.
Case Presentation
A 36-year-old male patient who was found HBsAg positive since childhood and had a poor response to TDF after 1 year of monotherapy was admitted to our hospital. The patient was infected with HBV by vertical transmission from mother to child, and his liver function was abnormal intermittently. The patient had no fatigue, oil aversion, poor appetite, and other discomforts and never used antiviral drugs before. The results of the analyses performed on February 6, 2017 before the initial treatment were as follows: HBsAg 26,522.70 IU/mL, hepatitis B surface antibody (HBsAb) 0.03 mIU/mL, HBeAg 1,352.77 signal-to-cutoff ratio (S/CO), hepatitis B e antibody (HBeAb) 4.55 S/CO, hepatitis B core antibody (HBcAb) 4.14 S/CO, and HBV DNA 5.55 × 108 IU/mL; liver function: alanine aminotransferase (ALT) 265.00 U/L, aspartate aminotransferase (AST) 157.10 U/L, and total bilirubin (TBil) 17.90 μmol/L; renal function: blood urea nitrogen (BUN) 3.22 mmol/L, creatinine (CREA) 42.20 μmol/L and glucose (GLU) 4.21 mmol/L; urine routine test: protein, blood, and glucose were all negative; blood routine test: white blood cell (WBC) 5.76 × 109/L, neutrophil count (NE#) 4.47 × 109/L, hemoglobin (HGB) 134.00 g/L, and platelet (PLT) 237.00 × 109/L; coagulation function: prothrombin activity (PTA) 80.00% and international normalized ratio (INR) 1.08; tumor markers were normal. The patient was diagnosed as HBeAg-positive CHB and treated with TDF (300 mg qd; Glaxo Smith Kline Co., Ltd., Tianjin, China).
On February 3, 2018, this patient was admitted to Beijing Ditan Hospital Affiliated to Capital Medical University. The examination results showed that HBsAg 16,102.20 IU/mL, HBsAb 0.03 mIU/mL, HBeAg 599.13 S/CO, HBeAb 4.51 S/CO, HBcAb 4.35 S/CO, and HBV DNA 9.21 × 103 IU/mL; liver function: ALT 17.90 U/L, AST 21.50 U/L, and TBil 21.10 μmol/L; renal function: BUN, CREA, and GLU were 2.78 mmol/L, 41.90 μmol/L, and 4.37 mmol/L, respectively; urine routine test: protein, blood, and glucose were all negative; blood routine test: WBC 6.34 × 109/L, NE# 3.96 × 109/L, HGB 144.00 g/L, and PLT 224.00 × 109/L; coagulation function: PTA 82.00% and INR 1.14. The results of HBV drug resistance test were negative. The patient had no previous noteworthy medical history, and did not smoke or consume alcohol. The patient denied the family history of cancer and mental illness. There was no obvious abnormality in physical examination.
According to the medical history and the corresponding examination results, reasons such as poor treatment compliance and drug resistance were excluded. The patient's HBV DNA load was still >2 × 103 IU/mL after 1 year of TDF monotherapy, suggesting that the patient did not respond well to TDF monotherapy. On February 7, 2018, the patient received TDF (300 mg qd; Glaxo Smith Kline Co., Ltd.) combined with Peg-IFNα-2a (180 μg qw; Shanghai Roche Pharmaceuticals Co., Ltd., Shanghai, China) antiviral therapy. HBV serological markers, HBV DNA load, biochemical indicators, and adverse reactions were monitored regularly.
At week 30 of combination therapy, HBsAg decreased >1 lg IU/mL (16,102.20–1,529.50 IU/mL); HBeAg decreased >1 lg S/CO (599.13–12.28 S/CO); HBV DNA decreased >2 lg IU/mL (9.21 × 103 to 3.26 × 101 IU/mL); at week 44 of combination therapy, HBsAg 682.40 IU/mL, HBeAg 6.32 S/CO, and HBV DNA <20 IU/mL, suggesting that a complete virological response was obtained. At week 58 of combination therapy, HBsAg decreased more slowly than before (682.40–669.90 IU/mL), thus IFN was stopped and only TDF was used to continue antiviral treatment, which was called IFN intermittent therapy. At week 71 of combination therapy, HBsAg decreased to 522.90 IU/mL, and then Peg-IFNα-2a was restored to combine with TDF again to continue the antiviral therapy. At week 96 of combination therapy, HBeAg seroconversion occurred (HBeAg 0.86 S/CO, HBeAb 0.52 S/CO); at week 122 of combination therapy, HBsAg seroconversion occurred (HBsAg 0.04 IU/mL, HBsAb 15.35 mIU/mL), achieving the clinical cure. After 24 weeks of consolidation therapy, HBsAg, HBeAg, and HBV DNA were persistently negative, and HBsAb further increased to 729.30 mIU/mL at week 146 of combination therapy, then TDF and Peg-IFNα-2a were stopped. Following up after 28 weeks of cessation therapy, the patient still remained clinically cured. During the treatment, the biochemical indicators and thyroid function of the patient remained normal. The adverse reactions such as NE#, platelet count, and HGB decreased within the normal range, and the fatigue and alopecia were minor. The serological, virological, and biochemical responses of the patient during treatment are shown in Table 1 and Figures 1 and 2.
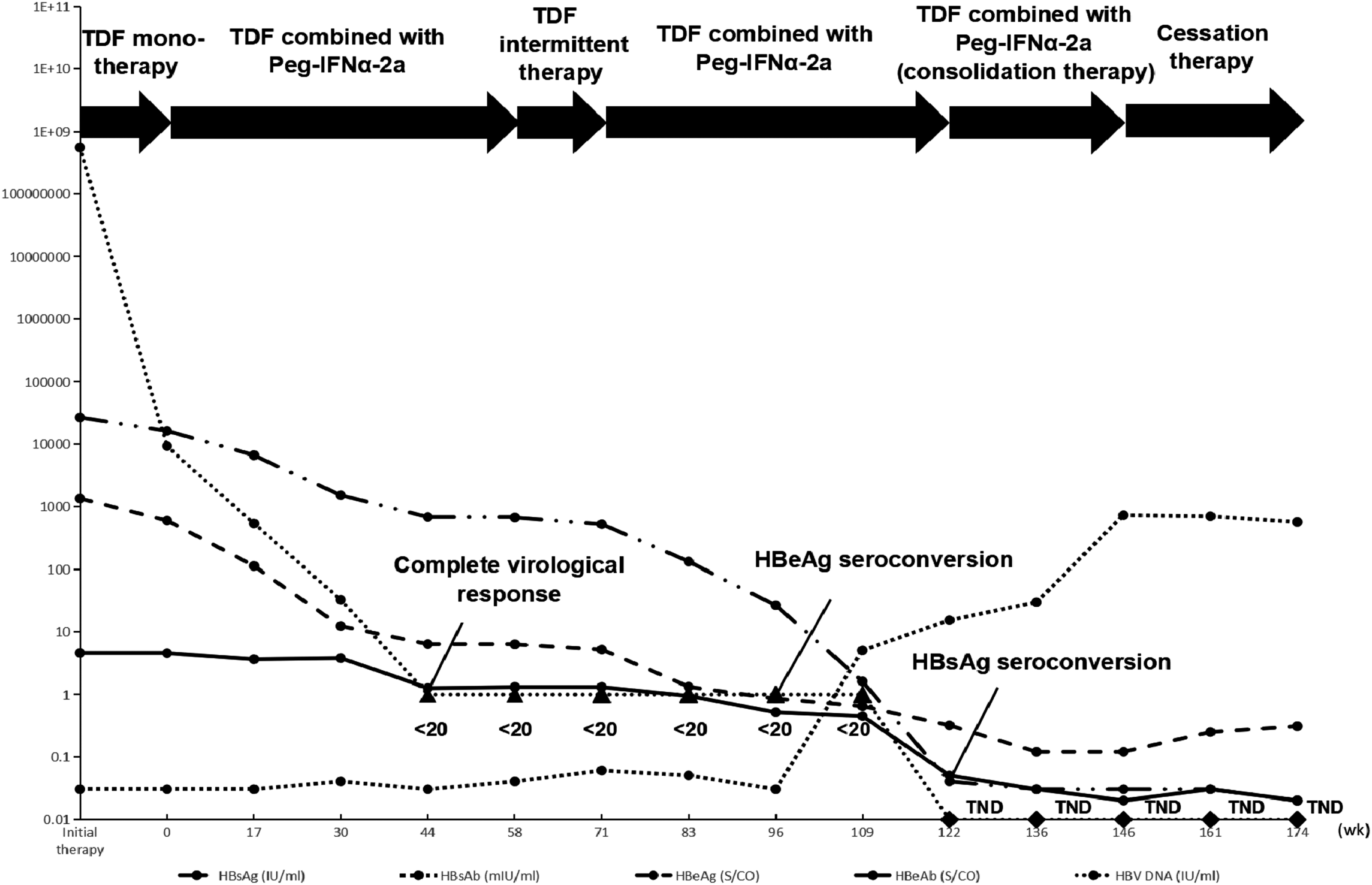
Serological and virological responses during treatment. HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; Peg-IFNα-2a, peginterferonalfa-2a; TDF, tenofovir disoproxil fumarate; TND, target not detected.
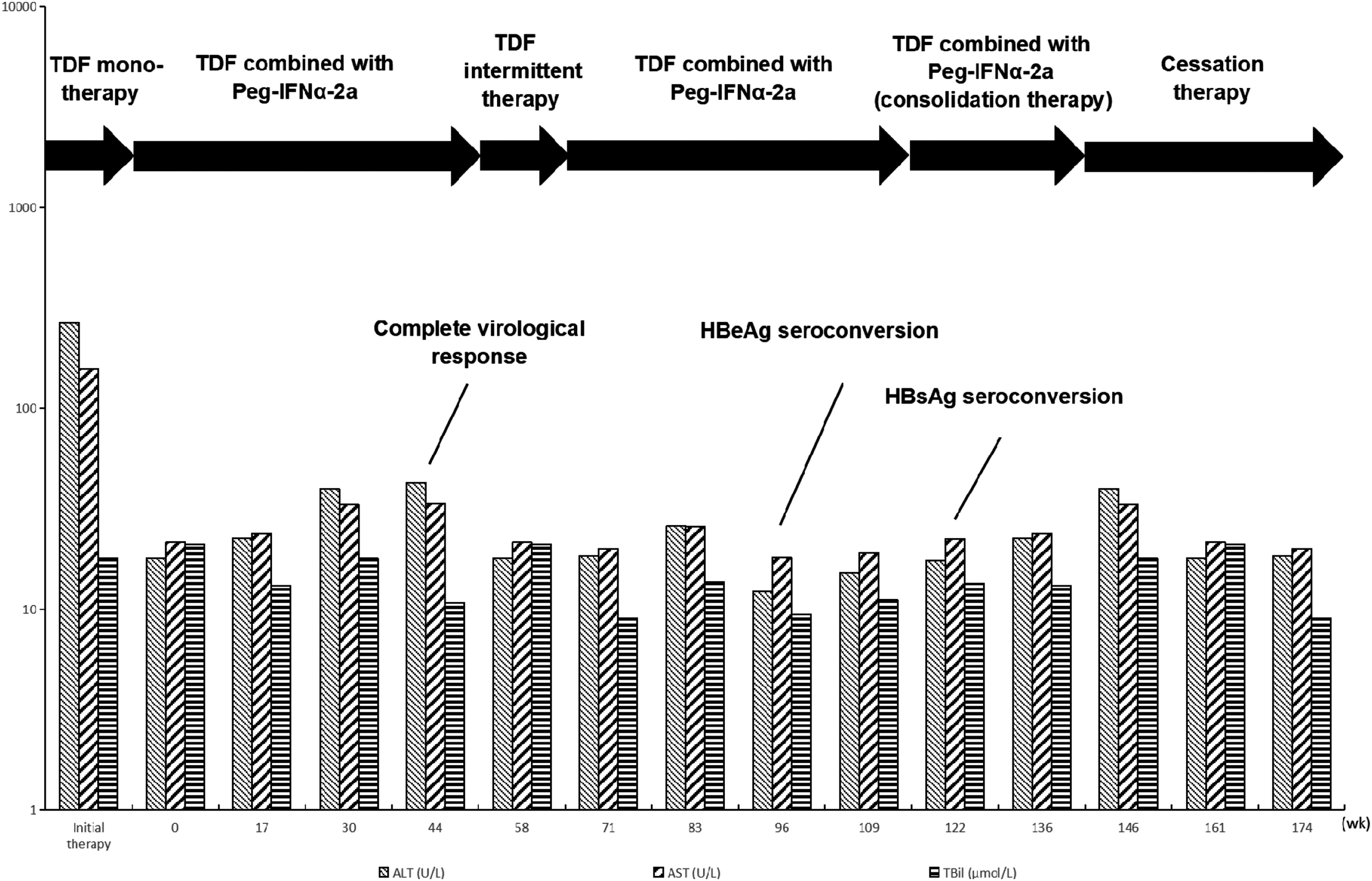
Biochemical response during treatment.
Serological, Virological, and Biochemical Responses During Treatment
ALT, alanine aminotransferase; AST, aspartate aminotransferase; HBeAb, hepatitis B e antibody; HBeAg, hepatitis B e antigen; HBsAb, hepatitis B surface antibody; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; Peg-IFNα-2a, peginterferonalfa-2a; S/CO, signal-to-cutoff ratio; TBil, total bilirubin; TDF, tenofovir disoproxil fumarate; TND, target not detected.
Discussion
The natural history of chronic HBV infection can be divided into four stages according to the natural course of disease, namely immune tolerance phase (chronic HBV carrier status), immune clearance phase (HBeAg-positive CHB), immune control phase (inactive HBsAg carrier status), and reactivity phase (HBeAg-negative CHB) (6). In this case, the patient's liver function was abnormally elevated, and the contents of HBsAg, HBeAg, and HBV DNA were all at the high level at the time of initial treatment in 2017, which meant that although the immune tolerance state had been broken, the nonspecific and specific immune functions were strongly inhibited (3,7,8,12). The low autoimmune status and active viral replication may be the reasons for the poor response to NAs monotherapy. At the same time, the high levels of HBsAg, HBeAg, and HBV DNA suppressed the nonspecific and specific immune responses, IFN alone may not play an effective role in immune regulation to achieve the enough antiviral effect in the initial treatment.
However, NAs can activate IFNα gene for a long time by inhibiting HBV replication (18), which can be beneficial to enhance the nonspecific immune activation mediated by IFN and lead to the enhancement of natural killer cell activity. It can not only eliminate the infected hepatocytes but also induce the compensatory proliferation of the hepatocytes while normal hepatocytes are injured, which increase the proportion of hepatocytes without cccDNA in vivo and promote the destabilization of cccDNA (13). Meanwhile, NAs can also relieve the inhibition of HBV-specific immune response in patients with high viral load by rapidly reducing the HBV DNA load, which contributes to the partial restoration of HBV-specific CD8+ T cells (7), so as to better play the immune regulatory role of IFN. Therefore, it is suggested that patients with high viral antigens and viral loads should be administered strong NAs and IFN-α antiviral combination therapy in the initial treatment (2). Li et al. (9) showed that the addition of Peg-IFNα-2a therapy could significantly improve the HBeAg seroconversion rate and HBsAg clearance rate in HBeAg-positive patients who did not achieve HBeAg seroconversion after long-term entecavir monotherapy. Meanwhile, many studies indicated that the combination therapy of Peg-IFNα and NAs was more effective than NAs monotherapy in inhibiting virus replication, realizing higher HBsAg clearance rate and maintaining a sustained immune response after cessation therapy (1,10,16). Thus, we promptly administered TDF combined with Peg-IFNα-2a antiviral therapy regimen when he was admitted to our hospital 48 weeks after initial monotherapy, which laid the foundation for clinical cure in the future.
Peg-IFNα treatment is often terminated in patients who cannot tolerate the side effects of Peg-IFNα such as fever, fatigue, decreasing leukocyte and platelet count, alopecia and anxiety. In this case, the patient's relevant symptoms were mild, and he was able to complete the entire course of the treatment. A complete virological response was achieved at week 44 of combination therapy, but HBsAg decline stalled from weeks 44 to 58, which may be due to the gradual depletion of HBV-specific CD8+ T cells in patient during IFN treatment (15), the decrease of IFN-α receptor 1 (IFNAR1) messenger RNA (mRNA) expression (14), and the appearance of IFN antibody in vivo (17). These reasons restricted the sustained response of body to IFN-α, resulting in the limitation of HBsAg clearance efficiency, thus Peg-IFNα-2a was discontinued between weeks 58 and 71, and only TDF was taken for maintenance treatment. At week 71, HBsAg began to decrease significantly again, indicating the necessity of intermittent therapy of IFN. The inhibition of high levels of HBsAg and HBeAg on HBV-specific CD8+ T lymphocytes was gradually relieved with the decrease of HBsAg and HBeAg titers, which was beneficial to the recovery of effective antiviral T cell response. Meanwhile, the number of HBV-specific CD8+ T cells and the expression of IFNAR1 mRNA gradually increased, and the titer of IFN antibody gradually decreased during the process of IFN being discontinued, allowing the body to restore its sensitivity to IFN. Therefore, the antiviral regimen of TDF combined with Peg-IFNα-2a was restarted, and the seroconversion of HBeAg and HBsAg occurred at weeks 96 and 122, respectively.
Our research (11) showed that consolidation treatment for 12–24 weeks after HBsAg clearance and higher HBsAb level could help achieve durable immune control and maintain clinical cure status. Therefore, the patient was treated with consolidation therapy for 24 weeks after HBsAg seroconversion. At week 146, HBsAg, HBeAg, and HBV DNA were persistently negative, and HBsAb was 729.30 mIU/mL, which meant sufficient protection. Then, TDF and Peg-IFNα-2a were stopped. After 28 weeks of follow-up, HBsAb was 566.62 mIU/mL at week 174, which still had the obvious protection and maintained the clinical cure effectively.
In conclusion, the course of treatment of this patient provides us with ideas for dealing with similar problems in clinical practice. For CHB patients with poor response to NAs, IFN can be combined to continue antiviral therapy, which not only reduces the incidence of NAs resistance but also produces synergistic antiviral effect, so as to control or even eliminate the virus. Therefore, even though Peg-IFNα has some side effects, this treatment strategy can still be attempted in some patients. At the same time, during the process of antiviral treatment based on IFN, intermittent therapy of IFN can be tried when HBsAg decline appears stagnated, which is conducive to better pursue the outcome of clinical cure.
Footnotes
Authors' Contributions
M.-h.L. and Y.X. contributed to the study design. Y.-j.L. and F.-f.S. contributed to follow-up with the patient. Z.Z., X.-y.B., and L.Y. contributed to data collection. Y.-j.L. wrote the first draft of the article. M.-h.L. and Y.X. revised the article and are the guarantors of the article. All authors approved the final version of the article.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
This study was funded in part by Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support (Nos. XMLX 201706 and XMLX 202127) and the Digestive Medical Coordinated Development Center of Beijing Hospitals Authority (Nos. XXZ0302 and XXT28).