
Abstract

Introduction
The mortality rate of coronavirus disease 2019 (COVID-19) patients is based on acute respiratory distress syndrome and coagulation abnormalities leading to thromboembolism associated with an increased risk of microvascular and pulmonary thrombosis. Thereby, venous thrombosis is more common than arterial thrombosis in patients with severe complications (2).
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection causes the initiation of numerous cellular pathways, such as coagulation, neutrophil extracellular trap formation, and complement system activation as well as hypofibrinolysis, endothelial dysfunction, cytokine storm, angiotensin-converting enzyme 2 (ACE2) downregulation, von Willebrand factor activation, and inflammation, which jointly contribute to thrombosis (2). Thus, investigation of these processes and interference with the productive infection of SARS-CoV-2 are crucial to mitigating severe clinical COVID-19 cases.
Thrombosis, which is generally caused by blood vessels becoming blocked with blood clots, is triggered by a variety of mechanisms, including thrombin formation and fibrin deposition (15). Indeed, not only thrombosis but also thrombocytopenia became a risk factor for the increased mortality of SARS-CoV-2 infection. Forty-five cases of auto-immune thrombocytopenic purpura (ITP), referred to as immune thrombocytopenia, were associated with COVID-19 infection (5).
Immune thrombocytopenia is considered to be an autoimmune hematological disorder that is characterized by low platelet counts due to platelet or megakaryocyte destruction through platelet recognizing autoantibodies and by increased bleeding risk. In this process, the binding of autoantibodies to thrombocyte receptors, namely membrane glycoproteins, leads to the formation of an antibody/thrombocyte complex that might result in thrombus formation and thromboembolism (16). Such an incident is common in hospitalized COVID-19 patients, indicating the need to investigate the cause of thrombosis and thrombocytopenia in SARS-CoV-2 infection.
Interestingly, severe thrombosis and thrombocytopenia were also observed in patients after SARS-CoV-1 infection (12). The exact origin of elevated blood clot formation in those patients is still unknown, but speculation has arisen that the activation of the coagulation pathway with increased levels of fibrinogen, SERPINs, thromboxane synthase, TLR9, and factors II, III, X are part of the SARS-CoV-1 pathogenesis (12).
The Spike protein (S protein), a homotrimer consisting of the S1 and S2 subunit, binds with the receptor binding domain (RBD) of the S1 subunit to ACE2 on the host cell followed by hydrolysis of the S protein, mainly by furin at S1/S2 interface and transmembrane protease serine 2 (TMPRSS2) at S2’ to mediate membrane fusion and entry of the virus (4).
The binding of SARS-CoV-2 downregulates levels of ACE2, thereby inhibiting the catalytic function of ACE2, which indicates enhanced angiotensin II activity. As a result, prothrombotic pathways are activated and Ang 1–7 signaling, which has an antithrombotic capacity, is inhibited (24). In this regard, administration of the anticoagulant drug heparin sulfate can also interfere with the attachment of the RBD of the S protein to the host ACE2 (11). Strikingly, it was demonstrated that binding of the SARS-CoV-2 S protein to ACE2 on platelets, which express TMPRSS2, provoked platelet hyperactivity (29). Moreover, the hydrolysis and partial release of the S1 subunit of the S protein trimer by furin can mediate thrombosis through binding and downregulation of ACE2 (18).
Thrombocytopenia and Complications of Post-SARS-CoV-2 Vaccination
To control the COVID-19 pandemic, numerous vaccines with promising efficacy have been developed and approved. However, the chimpanzee adenoviral AstraZeneca vaccine raises particular concerns regarding thrombosis leading to splanchnic-vein thrombosis, pulmonary embolism, and cerebral venous sinus thrombosis (CVST), which has been observed in patients (14).
A previous study reported that the ChAdOx1 vaccine of AstraZeneca results in the S protein embedding into the cell membrane of the target cell (27). Indeed, the tissue plasminogen activator (tPA) leader sequence, located at the N-terminus of the S protein sequence within the vector vaccine, allows the S protein to enter the secretory pathway; however, secretion might be interrupted, and the S protein could be integrated into the cell membrane through the hydrophobic transmembrane domain instead (27). In most cases, the leader sequence is cleaved from the S protein during or after polypeptide translation into ER, increasing secretion of the protein (26).
These findings give rise to speculation that the S protein, which is rapidly present on the cell surface, interacts with ACE2 on other host cells to activate prothrombotic signaling and results in thrombus formation. Furthermore, chimpanzee adenoviruses were used in AstraZeneca infected host cells, including megakaryocytes, through binding to the coxsackievirus and adenovirus receptor (8,9). Afterward, the S protein is expressed and traffics to the cell membrane, where the S protein is possibly embedded into the cell membrane and S protein-specific antibodies can bind to the surface of megakaryocytes. This S protein-antibody complex might provoke an immune response through antibody-mediated destruction of megakaryocytes, which results in reduced production of platelets. As a consequence, cases of auto-ITP are observed 7–10 days postvaccine.
In addition, these antibodies might trigger antibody-mediated thrombosis by activating the complement system, generating proteolytic active thrombin, which egresses the release of prothrombotic molecules from vascular endothelium (21). Furthermore, the Johnson and Johnson vaccine encompasses the replication-deficient human adenovirus serotype 26 and encodes the S protein with the tPA leader sequence in a similar manner to the AstraZeneca vaccine (6). CVST and thrombocytopenia were diagnosed in patients receiving the vaccine (19).
The Fc region of antibodies recognizing the S protein can activate platelets by binding to the cell surface Fc receptor FcγRIIa, which attach to vascular endothelial cells, and is also documented in COVID-19 patients with thrombotic complications (3,7). In rare cases after vaccination, CVST might be caused by the S protein antibody binding to endothelial cells. However, there is no evidence to support that S protein antibodies interact or bind to endothelial cells and might cause a CVST after vaccination. In contrast, thrombus formation might be caused by the binding of the S protein to endothelial cells through ACE2 and consequently complement deposition (22). Moreover, platelet activation is associated with an increased risk of thrombosis in people with diabetes, vascular diseases, stroke, fibrinolytic therapy, and unstable angina (1).
According to the European Medicines Agency report from March 24, 2021 (EPITT no: 19683), most patients experiencing thrombosis and/or thrombocytopenia had underlying conditions, including a history of diabetes and cardiovascular disorders. Contrarily, adenoviruses might not reach megakaryocytes located in the bone marrow, explaining a rare occurrence.
Recently, in a study involving 23 participants with thrombosis and thrombocytopenia after receiving the AstraZeneca vaccine, 22 cases were identified with antibodies specific for the platelet factor 4 (PF4) (25). In this regard, one following study refuted the possibility of molecular mimicry, suggesting epitope sharing between pathogens and self-proteins that possibly trigger autoimmune diseases (B cell mediated through autoantibodies and/or T cell mediated by being activated through pathogen-derived peptides bound to MHC molecules), of the SARS-CoV-2 S protein present in the vaccine compared with PF4 (13).
Given the evidence from this study and the fact that other S protein-based vaccines do not generate PF4 antibodies, the conclusion can be drawn that the translation and secretion of the tPA leader sequence together with the S protein might trigger the generation of “autoantibodies” recognizing PF4; due to homology to PF4, an autoimmune reaction occurs (23). For this purpose, we performed a comparison search between tPA and PF4 using the LALIGN program (
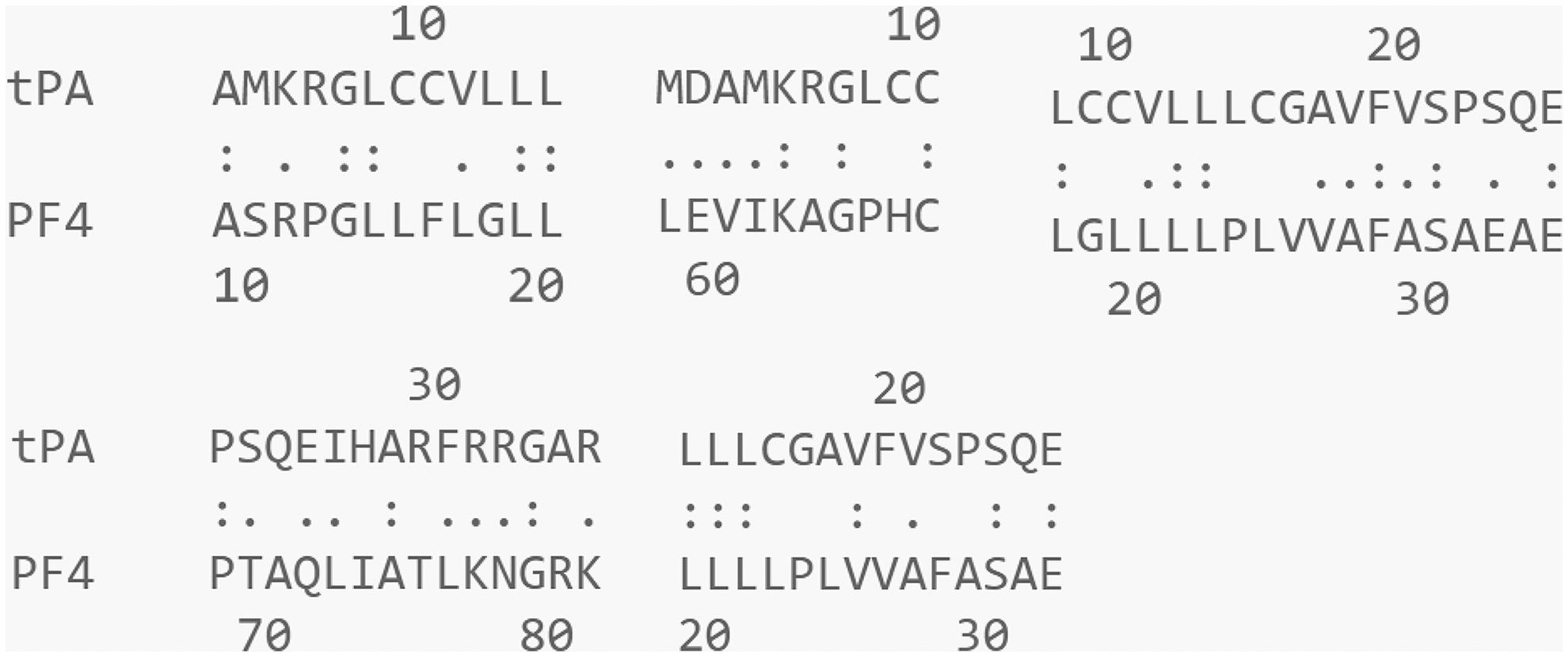
Amino acid sequence of the tissue plasminogen activator (tPA) leader sequence and platelet factor 4 (PF4). The corresponding regions were aligned using LALIGN program, and the homology of amino acids is depicted as follows: (:), identical; (.), conservative; (), different.
Discussion
Molecular and antigenic mimicry between the tPA leader sequence and the PF4 has not been reported previously. Using the LALIGN software, indicated regions of similarity were identified between the tPA leader sequence and PF4. Significant similarities were determined by the presence of at least 50% identical/conservative amino acids, sharing potential antibody epitopes among the tPA leader sequence and PF4. Although the observed similarities are not very high, flexibility and low affinity of antibodies to PF4 might be sufficient; however, this needs to be proven experimentally.
The Sputnik V vaccine, coding the full-length S protein, does not contain the leader sequence (17). We hypothesize that the absence of the 13 amino-acid-long wild-type signal peptide, which is generally responsible for the transport of the S protein to the membrane (28), and the lack of a leader sequence consequently prevents the guidance of the S protein toward the cell membrane. Ultimately, the S protein does not become integrated into the membrane. The S protein might remain inside the cell for antigen processing and loading to MHC molecules to be presented to T cells for an anti-SARS-CoV-2 immune response. This might avoid thrombosis.
Notably, the mRNA vaccines against SARS-CoV-2 by Moderna and Biontech/Pfizer encode the full length of the S protein and harbor a leader sequence, sec, which prepares the S protein for secretion (10,20). In contrast, there is no evidence that the S protein is immobilized into the cell membrane causing thrombosis. Further investigations are required regarding the leader sequence and possible association to thrombosis.
Summary
Thrombosis and thrombocytopenia are risk factors of the SARS-CoV-2 infection, but, in rare cases, also of two SARS-CoV-2 vaccines. ChAdOx-S and
Data Availability Statement
Data are available within the article or its supplementary materials.
Footnotes
Authors' Contributions
Writing, reviewing, and editing of the article by Z.M. and T.B.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
T.B. was funded by the Nazarbayev University Faculty-Development Competitive Research Grants Program, reference: 280720FD1907.