
Abstract
On March 11, 2020, the World Health Organization declared the coronavirus disease 2019 (COVID-19) outbreak a global pandemic. Although molecular testing remains the gold standard for COVID-19 diagnosis, serological testing enables the evaluation of the immune response to severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) infection and vaccination, and can be used to assess community viral spread. This review summarizes and analyzes the current landscape of SARS-CoV-2 testing in the United States and includes guidance on both when and why it is important to use direct pathogen detection and/or serological testing. The usefulness of monitoring humoral and cellular immune responses in infected and vaccinated patients is also addressed. Finally, this review considers current challenges, future perspectives for SARS-CoV-2 testing, and how diagnostics are being adapted as the virus evolves.
Introduction
In 2020, a worldwide public health pandemic resulted from the spread of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2), the virus responsible for coronavirus disease 2019 (COVID-19) (87). By the end of August 2021, >39 million COVID-19 cases and >600,000 deaths were reported in the United States, with numbers continuing to escalate (15). The emergence of new and highly contagious SARS-CoV-2 variants has created an increasing threat to public health, and certain variants appear to be responsible for increasing occurrences of breakthrough infections—those occurring in vaccinated individuals (49).
SARS-CoV-2 diagnostic tests have been critical in addressing the rapidly evolving COVID-19 pandemic. Molecular assays were the first to be developed and validated and were followed by serological tests. More than 1 year into the pandemic, >250 molecular and 87 serological assays have been granted Emergency Use Authorization (EUA) by the Food & Drug Administration (FDA) (36,37). Molecular and serological testing strategies must be continuously evaluated and updated as variant mutations occurring in certain parts of the viral genome could potentially impact the performance of SARS-CoV-2 testing (86).
In this review, we provide a general overview of SARS-CoV-2 infection and immune response to better understand the usefulness of molecular and serological tests and ultimately review the current and future diagnostic approaches for COVID-19.
SARS-CoV-2 Infection
SARS-CoV-2 is the fifth known beta-coronavirus with the ability to infect humans (12,87). It is an enveloped single-stranded RNA virus composed of four main glycoproteins, which are membrane (M), nucleocapsid (N), envelope (E), and spike (S), along with other nonstructural proteins encoded by the open reading frame region (Fig. 1) (3).

Schematic representation of the SARS-CoV-2 structure. The spike (S) protein enables host cell attachment and fusion. The nucleocapsid (N) protein is responsible for packaging the viral genome RNA and for viral assembly. The S1 subunit of the S protein contains the RBD that binds to the host ACE2 receptor. Neutralizing antibodies block the binding of SARS-CoV-2 to the ACE2 receptor. ACE2, angiotensin-converting enzyme 2; RBD, receptor-binding domain; SARS-CoV-2, severe acute respiratory syndrome-coronavirus-2. Color images are available online.
The S protein mediates receptor binding and membrane fusion activities. It consists of S1 and S2 subunits. The S1 subunit contains the receptor-binding domain (RBD) that binds to the host angiotensin-converting enzyme 2 (ACE2) receptor (Fig. 1) (6,114). The ACE2 receptor is present in respiratory tract epithelial cells, alveolar epithelial type II cells, and in tissues, including the lungs, intestines, heart, and kidney (3). After binding to the ACE2 receptor through the RBD, the S protein is proteolytically activated by human proteases resulting in cleavage at the S1/S2 site and S2 site, followed by fusion of the virus with the host cell (6,88,114). Once the virus enters the host cell, viral RNA is released leading to replication and transcription through protein cleavage (3).
The N protein's main function is to bind the viral RNA genome to make up the nucleocapsid (3). The N protein is largely involved in the replication cycle and host cell response to viral infection. The M protein promotes stabilization of the viral envelope and interacts with the E protein to release virus-like particles demonstrating its importance in complete virus production and maturation (83,96).
The primary route of SARS-CoV-2 transmission is through respiratory droplets by direct or indirect close range contact and when viral particles are inhaled or deposited on the mucosal membrane of the respiratory tract (21). The average incubation period, from viral exposure to symptom onset, is about 4–5 days (69,85). Most symptomatic individuals present with mild to severe symptoms within ∼12 days (85). The most commonly reported symptoms of SARS-CoV-2 infection include pyrexia, cough, dyspnea, myalgia, anosmia, ageusia, and gastrointestinal symptoms such as nausea, vomiting, or diarrhea (85). After the virus enters the host cell, its recognition triggers an immune response in the body (99). Both innate and adaptive immune responses are required for an effective response against SARS-CoV-2 infection.
Direct Detection of SARS-CoV-2
Direct detection of SARS-CoV-2 viral components includes molecular techniques to detect viral RNA and immunologic techniques for viral antigen detection. Both techniques detect active infections in respiratory specimens (Table 1).
Overview of Testing of Severe Acute Respiratory Syndrome-Coronavirus-2
IGRA, interferon-gamma release assay.
Molecular testing offers high sensitivity and specificity. The sensitivity relies on the viral load in the sample tested, the sampling site, and the timing of testing. Furthermore, the gene targets also affect the sensitivity and specificity of the molecular test (39,52). Studies on SARS-CoV-2 viral load kinetics in respiratory specimens showed the viral load peaks in the first week after symptom onset and then declines after day 10 of symptom onset, but viral RNA can be detected up to 14–17 days postsymptom onset (21,22,50,76,80,103,105,110). Therefore, the sensitivity of molecular testing decreases after day 10 of symptom onset. In addition, studies have reported detection of infectious virus up to day 10–12 after symptom onset (22,52).
Currently, molecular testing does not distinguish the presence of infectious and noninfectious virus (RNA traces) (62,64,74). Therefore, molecular testing cannot predict the risk of transmission by an infected person. The viral load may help to provide a better understanding of the risk of transmission and severity of the disease (43,65,93).
Molecular detection using isothermal amplification, CRISP-diagnosis, or real-time reverse transcriptase-polymerase chain reaction (RT-PCR) are currently the primary methods for diagnosis (39,52). Additional technologies, such as flow virometry, are also being explored for the direct detection of SARS-CoV-2 (101). As of November 16, 2021, the FDA provided EUAs for molecular-based detection and/or diagnosis of COVID-19 to 269 tests and 27 high-complexity laboratories that developed molecular-based laboratory-developed tests (36). Quantitative molecular tests have not received EUA so far (36). Therefore, the cycle threshold (Ct) values obtained in qualitative assays must be interpreted correctly. The use of Ct values to assess viral load is restricted to quantitative assays (18,48).
Recently, four different SARS-CoV-2 variants B 1.1.7, B 1.351, P.1
In addition to next-generation sequencing, commercial molecular assays have been developed to detect some of the new variants (2). These assays are important for public health laboratories for surveillance studies to investigate if these new variants can spread faster, reduce vaccine effectiveness, and/or cause more severe disease. It is important to consider that new variants will continue to emerge. Therefore, molecular assays will need to be continuously updated.
The Delta (or B 1.617.2) variant is the fastest spreading form of SARS-CoV-2 and is currently the predominant strain worldwide. “Breakthrough infections” refer to the development of SARS-CoV-2 infections in vaccinated individuals and are believed to be associated with the spread of the Delta variant. The discovery that the Delta variant results in a higher viral load may explain why vaccinated individuals are becoming susceptible to breakthrough infections, as they could be encountering a higher number of viral particles if exposed (16,72).
Antigen tests detect viral proteins. The main target of SARS-CoV-2 antigen-based tests is the N protein because it is abundantly expressed during infection (23,61,77). Antigen tests are currently authorized to be performed on nasopharyngeal or nasal swab specimens. As of November 16, 2021, the United States FDA provided EUAs for antigen-based detection to 39 tests consisting of 31 rapid tests and 8 automated laboratory tests for use in asymptomatic and symptomatic persons within the first 5–12 days after symptom onset (35). Antigen-based tests can be used as an alternative or in conjunction with molecular testing to increase testing capacity.
The sensitivity of antigen testing is favorable only when the viral load is high, thus indicating an infectious virus. Therefore, a positive result is associated with an increased risk of transmission (107). Proper interpretation of antigen tests is critical for accurate clinical management of patients with suspected COVID-19, or identification of infected persons when used for screening (82). The Center for Disease Control and Prevention (CDC) released interim guidance for antigen testing for SARS-CoV-2 to support clinicians in interpreting the results (13).
B Cell Immune Response and Antibody Detection
After SARS-CoV-2 infection, a majority of patients have a virus-specific immunoglobulin (Ig) response (92). Specifically IgA, IgG, and IgM antibodies are detected at varying times after the onset of the virus (Fig. 2).
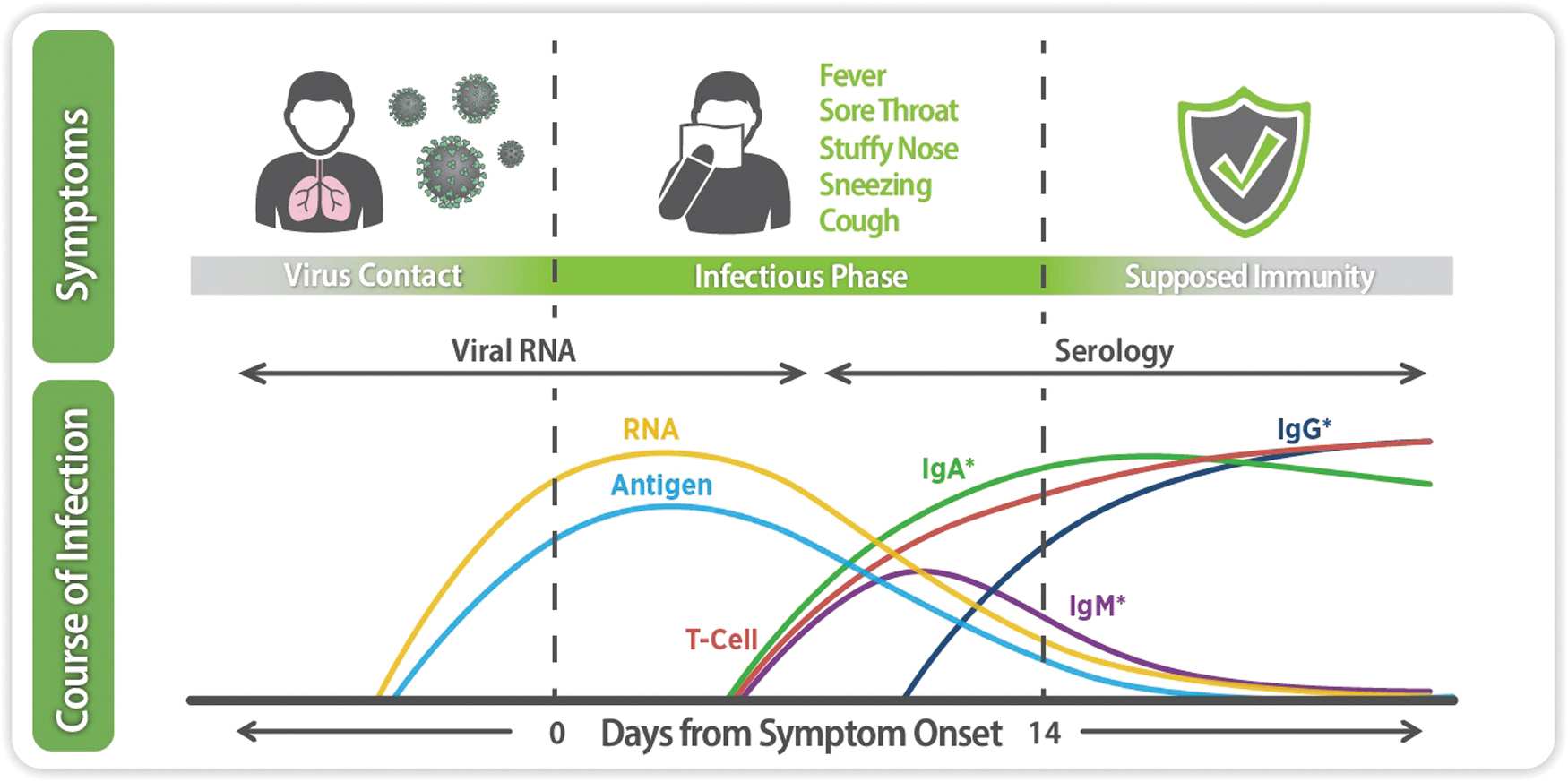
Serological response to SARS-CoV-2 infection. After a person comes in contact with SARS-CoV-2, antibodies (IgA, IgM, and IgG) are produced at different time points. In addition to the antibody response, T cell response aids in viral clearance. Levels of antibodies and T cell response remain in the body even after symptoms of the disease subside, providing potential protection from a repeat infection. *IgA, IgG, and IgM seroconversion may take place at different time points after contact with the pathogen. Ig, immunoglobulin. Color images are available online.
IgA antibodies are produced early (usually within the first 7 days) and peak by day 16–22 (5,51,79,92). IgA antibodies also have substantially higher affinities than IgM antibodies (5,51,79,92,99). This could reduce cross-reactivity commonly seen among coronavirus epitopes. In addition, studies have reported that during the early phase of the infection, there is a higher positivity rate for IgA antibodies (92.7%) compared with IgM antibodies (85.4%) (47,54,102). This suggests that IgA antibodies could also serve as a good marker for the early phase of the infection.
IgG antibodies can usually be detected within 14 days after the onset of initial symptoms, peaking by day 21–25 (51,79). IgM antibodies can be detected 5 days after symptom onset and start to decrease after 3 weeks postonset of symptoms (73). A study by Zhao et al. observed that within 1 week of SARS-CoV-2 symptom onset, <40% of patients (n = 173) had total antibodies (IgA, IgM, and IgG antibodies). Antibody levels drastically increased after 15 days postonset of infection to 100% of total antibodies and 79.8% of IgG antibodies (116).
Neutralizing antibodies have been detected in some patients in the early phase of the infection and peak during the second to third week after symptom onset (94,111). A recent study has reported the importance of IgA as a neutralizing antibody in the early phase of the infection (102). Additional studies have revealed that at least part of the neutralizing activity is mediated by anti-RBD IgM (42,66). Recently, it has been shown patients who have recovered from SARS-CoV-2 infection continue to produce antibodies, including neutralizing antibodies after 5–7 months postsymptom onset (55,56,104,112,117). IgM and IgA antibody levels against the S protein drop rapidly, with a duration of about 2 months postonset of symptoms (56). On the contrary, IgG levels persist up to 7 months postsymptoms onset suggesting prolonged immunity against SARS-CoV-2 (112,117).
To date, it is still unclear whether antibody-mediated responses in SARS-CoV-2 patients provide defensive immunity and how long immunity lasts.
T Cell Immune Response and Its Detection
In addition to B cells, T cells play a crucial role in adaptive immunity for viral clearance. A T cell response is a robust and broad response toward several SARS-CoV-2 viral proteins and is detected in most infected patients (7).
SARS-CoV-2 T cell responses can be detected at 3–5 days postsymptom onset (7) and functional SARS-CoV-2-specific T cell responses up to 6 months after infection (117). As reported in different studies, T cell responses against the S protein correlate well with IgA and IgG antibody titers in SARS-CoV-2 patients (98,99). This may have important implications for long-term immune response and vaccine technology. Interestingly, one study showed high levels of some cytokines seen in COVID-19 patients, as part of a cytokine storm, which may prevent the development of long-term immunity to SARS-CoV-2. However, this phenomenon, known as “immune amnesia,” is unlikely to occur after vaccination, suggesting that vaccination is the best way to generate effective herd immunity (63).
A robust T cell immune response has also been seen against the M and N proteins (99). It has been reported that 20% of patients who recovered from SARS-CoV-2 infection without detectable antibodies showed a T cell response against the virus (10,97). Therefore, it is important to measure both B and T cell mediated responses in postnatural infection as well as vaccinated individuals (Table 1).
More research is necessary to measure how strong the T cell response has to be to provide protection and for how long protection lasts (24,98). Therefore, the current use of assays to detect T cell responses is concentrated in research laboratories but not in routine clinical testing laboratories. SARS-CoV-2 T cell responses can be measured by different techniques: enzyme-linked immunospot (ELISpot) (70,97,117), interferon-gamma release assay (9,68), intracellular cytokine stain followed by flow cytometry (70,117), activation-induced marker followed by flow cytometry (46), and next-generation sequencing (100). As of November 16, 2021, the FDA granted one EUA for T cell response detection (37).
Serological Testing for Monitoring SARS-CoV-2 Immune Response
It has been reported that beyond 11 days postonset of symptoms, the viral replication time window is missed and false-negative RT-PCR results can be observed. At this stage of infection, the patient's humoral immune response is triggered, leading to the production of antiviral antibodies (47). Therefore, serological testing complements molecular testing. A positive test by serology indicates previous exposure to the virus. Depending on the antibody type detected, the stage of the infection (early or late) can be evaluated.
Several serological technologies exist for the identification of antibodies against SARS-CoV-2 (67). Enzyme-linked immunosorbent assays (ELISAs) and chemiluminescent immunoassays are used to detect the presence of virus-specific binding and neutralizing antibodies in a patient sample by monitoring the production of either an enzymatic color reaction or chemiluminescent signal, respectively. Lateral Flow Assays (LFAs) have been developed to detect antibodies against SARS-CoV-2 present in patient samples using antigens included in the test, which results in a color change.
Plaque reduction neutralization tests (PRNTs) are considered the gold standard in determining whether a patient sample contains neutralizing antibodies. PRNT assays are time- and labor-intensive, BSL-3 facilities are required and automation is not available, affecting turnaround times (106). Surrogate virus neutralization tests in ELISA format have been developed for the detection of neutralizing antibodies against SARS-CoV-2 (1,37). These surrogate ELISAs are rapid and easy to use compared with PRNT. In addition, these assays can be automated and performed at BSL-2 facilities.
The antigens most used to detect antibodies in serological tests are the S and N proteins since they are the primary viral antigens against which antibodies are raised.
Although the S protein is well known to be highly immunogenic due to its location on the surface of the virus, the N protein has also been found to have strong immunogenic activity due to its high expression during infection (28). However, there are potential disadvantages associated with detecting antibodies against the N protein in serological tests, including cross-reactivities among other endemic coronaviruses and a higher false-negative rate compared with that of targeting the S1 subunit of the S protein (45,60). One study reported a stronger cross-reactivity of SARS-CoV-2 for alpha-rather than beta-human coronavirus (HCoVs) (26). Considering SARS-CoV-2 has a lower amino acid sequence homology with alpha-HCoVs, the authors concluded that in addition to sequence homology, cross-reactivity is due to conformational homologies (26).
As of November 16, 2021, the FDA provided EUAs for antibody detection to 89 tests, including rapid tests, neutralizing tests, and quantitative, semiquantitative, and qualitative assays (37).
Clinical Significance of Serological Testing
Serological assays aid in understanding the immune responses to SARS-CoV-2, to identify individuals who were infected compared with those who were not (Table 1).
These data can be also used for epidemiological studies to assess community viral spread and to determine infection-related fatality rates (25). Such seroprevalence surveys identify individuals with antibodies against SARS-CoV-2 and are used by organizations such as the CDC and public health laboratories to better understand how the virus spreads over time across different regions.
Serological assays based on the N protein can help distinguish an immune response arising from an infection versus that from a spike-based vaccine. It is important to consider that antibody concentration decreases several months after infection and may become negative (44). In addition, serological tests can be used to identify potential donors of convalescent plasma for the treatment of patients with an active SARS-CoV-2 infection (38,53) and monitor the immune response of a plasma recipient (27,81).
Most serological assays on the market are qualitative, providing results as positive or negative depending on the presence or absence of antibodies. Fourteen semiquantitative assays have received EUA (37). These assays include several calibrators, allowing the creation of a standard curve. As a result, these assays can be used as an aid in measuring the antibody concentration over a broad linear range. Semiquantitative assays can be converted to quantitative when the calibrators are validated with an international standard (NIBSC code 20/136) (109). As of November 16, 2021, the FDA granted EUA to one quantitative serological assay (37). Semiquantitative and quantitative assays support the assessment of immune response to SARS-CoV-2 after infection or vaccination, providing a more accurate result on the rise or depletion of antibody levels.
The detection and measurement of neutralizing antibodies are critical to better understand long-term immunity. However, as we are still learning about protective immunity, it is unclear if surrogate neutralization tests are needed in routine clinical testing laboratories.
It is also important to consider that not all the patients recovered from SARS-COV-2 infection have a detectable antibody response and hence, it is critical to also consider the T cell responses in patients (24,98).
Serological Testing and Vaccine Development
In December 2020, the first two mRNA vaccines, Pfizer-BioNTech and Moderna were granted EUA by the FDA for the prevention of COVID-19 in the United States (17,84,91). Very recently, the Pfizer-BioNTech vaccine received full FDA approval (34). Both mRNA S-based vaccines are given in a two-dose series, 21 and 28 days apart for Pfizer-BioNTech and Moderna, respectively (4,17,84,91). Serological testing played an important role in confirming vaccine efficacy in both the Pfizer-BioNTech and Moderna phase 1 clinical trials (57,95). Binding antibody responses against the SARS-CoV-2 antigens and vaccine-induced neutralization activity were assessed by ELISA and neutralization assays, respectively. Vaccine recipients were also found to develop cellular immunity in both the Moderna and Pfizer-BioNTech clinical trials (57,95).
Further clinical trials are underway to test the efficacy of additional SARS-CoV-2 vaccines utilizing serological testing (40,78). A recent study found that binding antibodies to SARS-CoV-2 variants decayed faster over 6 months than antibodies to the first virus strain described in January 2020 (90). The effects on antibody potency of a third mRNA dose are currently under investigation, but early results show a boosting of response to SARS-CoV-2 variants (113).
In February 2021, the third vaccine against SARS-CoV-2 received FDA EUA in the United States. Johnson & Johnson (JNJ-78436735) developed a viral vector S-based vaccine (17). Findings from clinical trials indicated that Johnson & Johnson's COVID-19 vaccine efficacy is 66.3% ≥ 14 days after vaccination inducing neutralizing antibodies and T cell response (14,59).
Johnson & Johnson (JNJ-78436735) COVID-19 vaccine EUA was paused for 11 days in the United States after six cases of a rare and severe type of blood clot were reported in individuals vaccinated with this vaccine. On April 23, 2021, CDC and FDA resumed the use of this vaccine among people 18 years and older. The Advisory Committee on Immunization Practices and CDC also stated that women <50 years old especially should be aware of the rare but increased risk of a serious condition that involves blood clots (11,33,58).
Although serological testing is helpful for testing vaccine efficacy, the CDC and FDA do not recommend serology testing to assess immunity to COVID-19 after vaccination or the need for vaccination in an unvaccinated person (13,32). This might change once we better understand protective immunity to COVID-19 (75).
Although antibody-dependent enhancement (ADE), in which medical interventions such as vaccines exacerbate the disease, has been observed in certain human respiratory virus infections, studies have not yet fully established a role for ADE in human COVID-19 pathology. One study used molecular modeling to show that enhancing antibodies have a higher affinity for Delta variants than for the original Wuhan/D614G strains; however, clinical data have not yet confirmed this mechanism (115). Regardless, it is important to note that immunotherapies that induce or deliver high doses of neutralizing antibodies are advantageous for limiting the potential risk of ADE (71).
Future Perspectives
Despite the efficient and reliable diagnostic testing available to detect SARS-CoV-2 and antibodies, some limitations include the harmonization of current diagnostic assays. It is critical to be able to compare the results between different assays to unify the patient test results, irrespective of the test performed. Such measures will help the community better understand the immune response to both the virus and vaccine, assess community spread of the virus, and determine accurate herd immunity status.
Initiatives, such as those organized by the Foundation for Innovative New Diagnostics (FIND) (39) and the FDA, are critical to select the most accurate and reliable diagnostic assay.
The FDA also established the SARS-CoV-2 Reference Panel to allow for a direct evaluation of specificity and sensitivity between SARS-CoV-2 tests (31). The WHO has released the first Reference Standard for anti-SARS-CoV-2 Ig (NIBSC code: 20/136) for calibration of serological assays and aiding in the determination of antibody levels needed to build protective immunity and produce efficacious vaccines (109). Based on this International Standard, results can be indicated as Binding Antibody Units (BAU)/mL when using assays to detect binding antibodies (109). In addition, for better comparability of results, results are indicated as International Units (IU)/mL when using assays to detect neutralizing antibodies (109).
New diagnostic assays that could distinguish the vaccine response from an initial infection or reinfection are required to better understand long-term immunity response. For example, multiplexing using blot technology can aid in detecting and differentiating antibodies against different antigens (e.g., antibodies against nucleocapsid vs. spike protein) (30). Immunofluorescence assays using SARS-CoV-2-infected cells as a substrate have a very high sensitivity but due to the cross-reactivity with other common coronaviruses, a confirmatory ELISA, chemiluminescence or blot would be required (29). Furthermore, avidity assays would help distinguish a recent infection from a past vaccine or infection antibody response (41).
The field of SARS-CoV-2 diagnostics, therapeutics, and vaccines is rapidly evolving, as is the virus. With 50% of the U.S. population being vaccinated (89), there is a need for understanding the level and longevity of antibodies (especially neutralizing antibodies) and T cell response. This information will aid in determining the appropriate timing for receiving booster shots to protect against reinfections in naturally infected people or to prevent severe COVID-19 infections after vaccinations. It is also crucial to learn how existing and novel diagnostic tests may be able to assist in such a determination and/or include them in routine clinical testing. There is an urgent need for longitudinal studies using various types of serological assays, to better understand the long-term immune response against SARS-CoV-2.
With a recent surge in COVID-19 cases, new CDC recommendations mandate both vaccinated and unvaccinated individuals to wear masks in public indoor settings (20).
Currently, the CDC recommends third vaccine doses for immunocompromised individuals who may not have had a successful immune response after the completion of their second dose to provide an adequate immune response. In one study, 46% of organ transplant recipients did not exhibit an antibody response after two doses of an mRNA vaccine (8). Booster shots are also expected to be available this Fall for healthy individuals who had received either the Pfizer-BioNTech COVID-19 vaccine or Moderna COVID-19 vaccine 6 months prior. It might be useful to screen patients for their antibody levels using the EUA approved semiquantitative or quantitative S protein-based serological tests to better understand the need for a third vaccine shot in vaccinated individuals.
The recent surge in COVID-19 cases further emphasize the importance of early and accurate diagnostic testing to control the spread of the disease. In addition, social distancing guidelines and masking policies should be followed.
Footnotes
Author Disclosure Statement
Maite Sabalza, Ilana Heckler, Aya Elhage and Iswariya Venkataraman are EUROIMMUN US employees. Brandon Henry has no competing financial interests.
Funding Information
No funding was received.