
Abstract
COVID-19 is a life-threatening respiratory disease triggered by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). It has been considered a pandemic viral infection since December 2019. The investigation of the effective prophylaxis or therapeutic strategies for emergency management of the current condition has become a priority for medical research centers and pharmaceutical companies. This article provides a comprehensive review of antibody therapy and its different categories with their advantages and disadvantages for COVID-19 over the last few years of the current pandemic. Antibodies can be generated by active immunization, including natural infection with a pathogen and vaccination, or by the passive immunization method such as convalescent plasma therapy (CPT) and antibody synthesis in laboratories. Each of these ways has its characteristics. Arming the immune system with antibodies is the main aim of antiviral therapeutic procedures toward SARS-CoV-2. Collecting and discussing various aspects of available data in this field can give researchers a better perspective for the production of antibody-based products or selection of the most appropriate approach of antibody therapies to improve different cases of COVID-19. Moreover, it can help them control similar viral pandemics that may happen in the future appropriately.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the name of the virus that caused the COVID-19 pandemic. It is a single-stranded RNA virus of the betacoronavirus genus belonging to the Coronaviridae family. Having a high rate of mortality and severe complications in the critical organs of the body, SARS-CoV-2 has endangered the lives of many people around the world (41,127). The main transmission route is through inhalation of infectious respiratory droplets produced by the infected person, but the other ways of transmission, such as postnatal, fecal–oral routes, and the contact with contaminated surfaces, have been reported (10,108).
Clinical manifestations of COVID-19 are varied depending on the individual condition of patients and their symptoms, including headache, diarrhea, sputum production, hemoptysis, the loss of smell or taste, and severe inflammatory responses such as acute respiratory syndrome disease (14). However, the primary concern about novel coronavirus is the vital organ damage caused by the virus, such as lung and heart damage, which can lead to death in severe cases (57). Discovering a suitable approach to prevent any infectious disease requires enough knowledge about the pathogenicity pattern of its microbial agent (54,102).
It has been demonstrated that the potent immunogenic factor of SARS-CoV-2 is the spike (S) protein. S protein, through its receptor-binding domain (RBD), attaches to the angiotensin-converting enzyme 2 (ACE2) expressed on the surface of the human host cells. It subsequently leads to infection and causes tissue damage due to the virus entry (70). Therefore, researchers have considered S protein the most important therapeutic target for designing drugs and vaccines to combat SARS-CoV-2 (79,114).
Among the various therapeutic methods for COVID-19, immunotherapy by antibodies has attracted a wide range of attention. Antibodies are glycoproteins that belong to the adaptive immune system and play a critical role in protecting our health. Nowadays, antibodies have a notable proportion of immunotherapeutic strategies to overcome different diseases (11).
This article aims to review the recent antibody therapy studies of COVID-19. Moreover, this topic is discussed coherently from various aspects, including the importance of antibodies in immunity, prognosis, and the treatment of COVID-19. This study can be helpful in recognizing the suitable viral target for antibody-related therapeutic strategies, such as vaccine design, antibody therapy principles, its different subtypes, and their advantages and disadvantages in preclinical and clinical studies. Therefore, the new update of the latest available data for 2020–2021 was collected comprehensively to serve as the road map for future investigations.
Immune Responses Against SARS-CoV-2 Infection by Focusing on Neutralizing Antibodies
The pathogenesis of SARS-CoV-2 and immune-related mechanisms during infection can provide an excellent potential therapeutic target. Evidence has shown that immune responses play a double-edged role in the process of COVID-19 (91). Immunologically, the SARS-CoV-2 entry into the ACE-expressing cells, particularly lung epithelial cells, can overactivate the innate and immune responses. Neutrophils accomplished by alveolar macrophages serve as the substantial innate immune cells to recruit the other immune cells into the engaged organ, and enhance the inflammatory responses through producing cytokines and chemokines, such as interleukin-6 (IL-6), IL-1β, and tumor necrosis factor-α (TNF-α).
Subsequently, cytotoxic CD8+ T cells (CTLs), CD4+ Th (T helper) cells, and B cells are derived from adaptive immunity against the virus. Moreover, antibodies have a vital role during the infection. The evaluation of COVID-19 patients revealed that immunoglobulin (Ig)A, IgM, and IgG are almost produced against nucleocapsid (N) and spike (S) proteins of SARS-CoV-2 (31,53). Actually, neutralizing antibodies (nAbs) create antiviral protection through various mechanisms. Antigen-binding sites of the antibodies compete with ACE2 to bind to RBD.
In addition, IgG can support viral clearance and help the improvement of infection by specific activities, including antibody-dependent cellular cytotoxicity and complement-dependent cytotoxicity. These mechanisms are mediated through the interaction between the FC region of IgG and FC receptors of effector cells (natural killer cells and phagocytes) or binding to the complement 1q (C1q), respectively. Furthermore, FcRn expressed by several types of cells, such as endothelial cells, can help the recycling of IgG in the fluid phase of uptake, and contributes to its long half-life (21 days) and humoral immunity against the virus (74).
On the contrary, nAbs can also exert detrimental effects during COVID-19 by inducing hyperinflammatory responses and vital organ damage. Indeed, robust nAb responses seem to be correlated with the severity of the disease. The uncontrolled nAbs binding to the virus without blocking infection leads to pathological conditions (131). In this regard, antibody-dependent enhancement (ADE) has been characterized as a vaccines response prominent phenomenon. ADE occurs in viral infection under distinct pathways. Phagocytes are involved in enhanced antibody-mediated virus uptake by their FcγRs, and cause increased viral replication, excessive immune complex formation, and hyperinflammation through a high amount of inflammatory mediators' production (110).
Reports have shown that diminished frequency and dysfunction of regulatory T cells and also the increased Th1 and Th17 cells are effective in inducing the inflammation (137). Altogether, all the above immune alterations cause cytokine storm, a common complication in severe cases of COVID-19. Cytokine storm or cytokine release syndrome (CRS) is elicited by upregulation of proinflammatory mediators, such as IFN-γ, TNF-α, IL-1β, IL-6, IL-8, IL-17, granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), membrane cofactor protein (MCP-1), and macrophage inflammatory protein-1 alpha (MIP-1α) during SARS-CoV-2 infection, which leads to vital organ damage of patients and even death (43).
Farmani et al. assessed the role of IgE as the main component of postinfection sensitivity in their review study. They concluded that specific IgE and the activation of mast cells play an important role in exacerbating SARS-CoV-2 infection (32). Fodor et al. summarized the correlation between inflammation, endothelial dysfunction, and COVID-19 and its pathogenesis importance in microvascular-related complications to extend therapeutic approaches (36).
S Protein Antigen as the Potent Target for nAbs Against SARS-CoV-2
Identifying an appropriate target antigen throughout the pathogen structure is the most critical point in designing immunotherapeutic strategies to eradicate or control infectious diseases. According to the valuable data from the previous coronavirus, SARS-CoV, and the recent studies regarding the COVID-19, the S protein of SARS-CoV-2 is considered the best option for vaccine development.
Exhaustively, the S protein is one of the four structural proteins of SARS-CoV-2 composed of two functional subunits, including S1 and S2. S1 subunit, through its RBD, is responsible for virus binding to ACE2 on the surface of host cells. However, the S2 subunit has a transmembrane anchor involved in the fusion of cell membranes of the host cells and virus, followed by internalizing the particles into acidified endosomes (122,143).
S protein contains multiple neutralizing epitopes. Thus, it causes the production of nAbs, which can disrupt various steps of the pathogenicity process (11,87). Consequently, the S protein can provide protective immunity against SARS-CoV-2, the golden aim of antiviral therapeutic approaches (45).
Arashkia et al. discussed the potential of S protein as the candidate antigen to design COVID-19 vaccines. They collected data from different vaccine platforms using the S protein of SARS-CoV-2 and its various related segments, including RBD, NTD, S1, and S2, to induce humoral and cellular immunity. They concluded that the S1 subunit or RBD of S protein is the most suitable immunogen to induce nAbs production (6).
Antibody Therapy for COVID-19
It has been considered to use antibody therapy to deal with the pandemic of COVID-19 because of the vital role of strengthening the immune system at the optimal level to overcome viral diseases and the proven therapeutic efficacy of antibodies for some of the viral infections developed by Ebola, HIV, and MERS (3,25,39,111,136). Investigations have shown that nAbs with high scalability, safety, and broad-spectrum functions could be a helpful therapeutic weapon to fight against novel coronavirus and its mutant escape variants (61,119).
It has been concluded that the evaluation of specific nAbs against SARS-CoV-2 is critical to early diagnosis, therapeutic strategy, and preanalysis of vaccine responses to plan for the perfect design (74). However, to take any therapeutic measure, we must know the exact principles of using antibodies to treat COVID-19 patients. Three significant factors, including specificity, time, and the number of antibodies, are essential in the efficacy of antibody therapy against SARS-CoV-2. The antibody must be specific and prescribed at the optimum dosage at the early stage of infection to achieve a favorable outcome.
Optimum dosage is influenced by multiple factors, such as viral load, epitope specificity, isotype composition, and antibody–virus interaction in each patient. Also, it has been recommended that frequent prescription of lower doses is more effective than the high single dose, and the initial regimen should be high enough to mediate rapid viral clearance (24,125). Ning et al. focused on corresponding challenges of antibody therapy for COVID-19, including standardization, quality control, ADE occurrence, and antibody-resistant variants of SARS-CoV-2 (87).
It has been indicated that the recombination and amino acid mutation in RBD are associated with the enhancement of infectivity, viral replication capacity, and structural stability (60,89). In this regard, the cocktail of monoclonal antibodies (mAbs) with varied targets and also Fc engineering could be the solution to avoid escape mutations and reduce the risk of ADE (78). For example, using techniques such as sequence modification of the IgG-related amino acid by inserting LALA mutations has been recommended to detect and delete the ADE-associated epitopes (74).
Antibody therapy can be discussed in two main subgroups to improve COVID-19. The first is related to the isolation of nAbs from the plasma of infected patients after recovery (convalescent plasma therapy [CPT and intravenous immunoglobulin
The common principle in all routes is to consider the S protein of SARS-CoV-2 as the most crucial target for antibodies (Fig. 1). In addition, detrimental immune responses (i.e., mediators, cells, and pathways) toward SARS-CoV-2 infection are the other potential therapeutic targets (40).
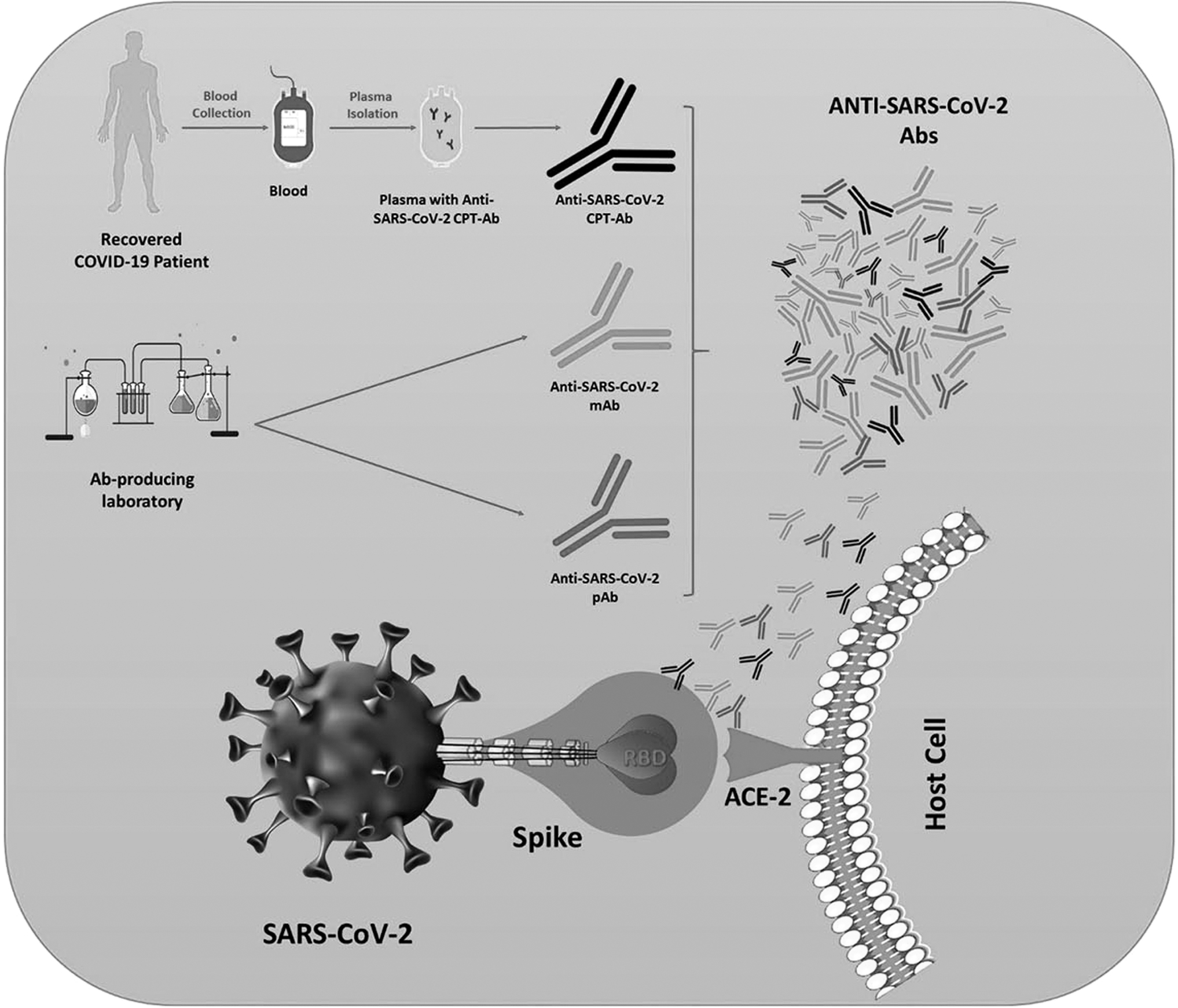
Mechanism of action of CPT-Ab, mAb, and pAb on binding and entry of coronavirus into the host cell. “S protein” of SARS-CoV-2 is the most important therapeutic target for the designing of antibodies in multiple antibody therapy approaches by using mAbs, pAbs, and CP to battle the COVID-19. CP, convalescent plasma; CPT, convalescent plasma therapy; mAbs, monoclonal antibodies; pAbs, polyclonal antibodies; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Convalescent plasma therapy for COVID-19 patients
Convalescent plasma (CP) is rich in nAbs collected from hyperimmune patients recovered from viral infection. CPT is a helpful method to ameliorate viral infections. It was introduced during the Spanish influenza pandemic in 1918–1920 (19). Then, it was suggested as a safe and effective therapeutic approach candidate for the Ebola virus in 2014. Moreover, CPT has been reported to treat and prevent the other viral diseases, including Junin (which is responsible for Argentine hemorrhagic fever), avian influenza A, MERS, and SARS-CoV (2,104,112). Based on the evidence, CPT has a good potency in managing SARS-CoV-2; especially it is useful for prophylaxis in high-risk persons, including health care workers, and susceptible individuals with any underlying diseases (18,94,128,139).
Results have shown that the administration of CP with a high titer of nAbs could significantly reduce the viral load and severity of the complications, such as ARDS, rate of ICU hospitalization, and mortality in COVID-19 patients (12,47,58,103).
A narrative review study suggested a novel route of CPT by using pulmonary aerosolized formulation to improve clinical symptoms of COVID-19 cases (33). In addition, the safety and efficacy of CPT have been shown in immunocompromised cases (113). It is speculated that COVID-19 patients with immunodeficiency disorders are more vulnerable due to their insufficient antibody levels during antiviral responses. Therefore, CPT could be a promising strategy in these cases.
It also has an excellent capacity to prevent the severity of manifestations and reduce the risk of death in transplanted COVID-19 patients (35). Feasibility and well toleration are the common preference points of CPT considered by researchers. Moreover, treatment through CP can suppress virus activity at both the entry and replication stages (103,128). It can also inhibit ARDS (118). Thrombotic events are the most horrible complications of COVID-19, which explain the therapeutic function of CP (37,74).
CP must be administered in the early phase of SARS-CoV-2 infection and before seroconversion observation to affect better. Preferably, the fifth day is the best time for its maximum efficacy. Furthermore, CP should be transfused in optimal doses. The recommended dose of administration for COVID-19 patients (weighing 50–80 kg) is two plasma units (200–250 mL each) (73,126,149).
Although CPT has been suggested as a promising approach to ameliorate COVID-19, it has several disadvantages, including the risk of infection transmission, nonscalability, and the contingency occurrence of host reactions, such as rash, fever, hemolysis, and ADE. This occurs when the patient is contaminated with other virus serotypes and has generated antibodies during the previous infection. Therefore, patients under CPT should be monitored carefully to avoid any unexpected severe side effects (18,150).
Polyclonal antibodies for COVID-19
It is established that polyclonal antibodies (pAbs) are a type of antibody derived from different B cell lineages. Therefore, they can recognize various epitopes of a specific antigen, in contrast to mAbs designed to identify a unique epitope (5).
According to various investigations, researchers have suggested that the treatment of COVID-19 cases with pAbs can cover the weak points of CPT. Generally, the application of pAbs to the urgent treatment of COVID-19 has been justified for two main reasons: (i) Their production process in the laboratory for clinical use is more cost-effective and faster than mAbs. (ii) Targeting multiple epitopes instead of a single epitope can increase the effectiveness of passive immunotherapy techniques by pAbs.
On the contrary, pAbs seem to be more effective and safer than plasma-derived antibodies due to the production technology by immunized animals or specific cell lines. Clinical administration of pAbs has reduced the risk of crosscontamination and prevented host-related acute immune responses. In addition, since pAbs have the potency to target more than one epitope, using them can diminish the possibility of escape-mutants and enhance the effect of nAbs synergically (49,90,98). In this regard, several pharmaceutical companies have determined to design pAbs to fight against novel coronavirus.
For example, the SAB biotherapeutic company has manufactured anti-SARS-CoV-2 full human pAbs in genetically engineered cattle (69,132). rCIG is a recombinant anti-SARS-CoV-2 pAb produced by GigaGen pharmaceuticals. Emergent BioSolutions companies also developed hyperimmune pAbs against SARS-CoV-2, called COVID-EIG/HIG. This type was isolated from human plasma or immunized horses. Researchers under the Regen company also succeeded in producing the fully human multivalent antibodies against the spike protein considered as a cocktail of the nAbs, including REGN3048-3051. In addition, it was derived from ameliorated COVID-19 patients or genetically modified mice (68,90,117).
mAbs for COVID-19
The development of mAbs is a turning point in treating many diseases because of their specificity, scalability, long half-life, and purity. mAbs have been described as a novel strategy to manage viral infections (21,116). Prominent examples in this regard are mAb114 and REGN-EB3, which comprise a single cocktail of mAbs toward the Ebola virus (63).
mAbs are generally generated by cloning unique white B cells, so they have a monovalent affinity for binding to just the same epitope. There are several techniques to manufacture mAbs, including hybridoma technology, using phage-display systems, isolation of memory B cells from CP, and immortalizing them by EBV transformation (4,80,93). The exciting novel generation of mAbs is dewetting mAbs developed to promote the antibodies' efficacy.
Dewetting transition is the phenomenon that can be involved in disrupting cellular activity by preventing water transition due to hydrophobic pores formation in the ion channels. This is a solid tool to block pathogens such as viruses. For example, one kind of ion channel called viroporins is detected in SARS-CoV-2, which accounts for a critical function in the pathogenesis cycle of the virus. Viroporins have been suggested as a target for dewetting mAbs against novel coronavirus (7,130).
Scientists designed specific SARS-CoV-2 dewetting mAbs based on available data (52,92,124,142). A substantial body of clinical trial investigations indicated the successful outcomes of dewetting mAbs therapy in COVID-19 patients, including respiratory disorders, reduction of fever, decreasing the risk of hospitalization, and worsening of the disease (59,75,115,116). Recent evidence demonstrated that dewetting mAbs could decrease the risk of hospitalization and worsening of the disease in high-risk COVID-19 patients (115).
The immunological reactions, which are probable after mAbs treatment, are fever, irritation at the site of injection, dermatological reaction, and even anaphylaxis. Also, the administration of mAbs may lead to CRS, which is one of the most dangerous side effects of mAb therapy (9). Therefore, the utility of mAbs must be monitored by experts and with medical supervision, although they have precise performance. Nevertheless, mAbs are valuable therapeutic tools, and further investigations in the future are required to find solutions and minimize their drawbacks (90).
Antibody candidates interrupt the SARS-CoV-2 structure in the virus attachment and entry to the host cell level
The highlighted point in designing these types of dewetting mAbs is their ability to be detrimental to the formation of the S protein–ACE2 receptor complex. Evaluation of the SARS-CoV-2 pathogenesis has shown that the RBD domain located in the S1 unit of spike protein, especially in the residue of amino acids 319–591, plays the most important role in the viral attachment to the host cell, which leads to virus entry and infection (Fig. 2) (26,140). Therefore, RBD has been purposed as the best effective target for mAbs against SARS-CoV-2 (101,147).

Coronavirus spike protein structure and its binding site to the host cell. The spike (S) protein known as the most potent immunogenic part of the SARS-CoV-2 structure attaches to the ACE2 on the surface of the human host cells through its RBD to infect them. ACE2, angiotensin-converting enzyme 2; RBD, receptor-binding domain.
For instance, S304 and S315 are human mAbs that targeted the RBD domain of SARS-CoV-2 but did not compete with RBD–ACE2 binding. However, P2C-1F11, P2B-2F6, and Vh–Fc ab8 are human mAbs produced to compete with ACE2 to bind the RBD domain and neutralize novel coronavirus (65,98). Also, the other human mAbs, such as CC6.29, CC6.30, CC12.1, n3088, and n3130, can target SARS-CoV-2 RBD to neutralize pseudotyped and live SARS-CoV-2 infections (51,105). The other RBD-specific antibody is scFv-human Fc 5C2, which was found recently to neutralize SARS-CoV-2 by preventing ACE-2–S protein attachment (148).
Multiple factors, including dosage, mAb properties, and the expression level of some viral-related receptors such as FCRs, can influence the consequence of antibody binding to the RBD domain. Indeed, conformational alteration in the RBD domain might lead to the halt of the virus activity or trigger the ADE (135).
Nevertheless, the domains, such as S-ectodomain, HR1, and HR2, can be recognized through antibodies (30,153). For example, nAbs, including 1A9, 2B2, 1G10, and 4B12, have been defined to neutralize SARS-CoV-2 by targeting its HR2 domain (151). It has been found that 4A8, 5–24, 2–17, and 4–8 could target SARS-CoV-2 NTD to neutralize the pseudotyped and live SARS-CoV-2 infection. Furthermore, S309, CA521 FALA, 2–43, 2–51, VIR-7831, LY-CoV555, scFv 80R, and REGN-COV-2 (REGN10933 + REGN10987) are defined as the other neutralizing mAbs that prevent the interaction between SARS-CoV-2 and ACE2 (22,29,42,50,95,120).
Nanobodies, the single variable domain (VHH) generated by camelids, have opened a new window to the antibody therapy for COVID-19 due to their capacity of access to more epitopes, small size, scalability, and cost-effective manufacturing process. Also, they can be administered directly to the site of respiratory infection through an inhaler (17,76,86). VHH-72-Fc is a nanobody with a bivalent structure, which rendered the neutralizing activity against the S protein of SARS-CoV-2 pseudoviruses (123).
Several studies have stated that the other cellular agents, such as DS-SIGN, intercellular adhesion molecule 3 (ICAM-3), cytoskeleton protein, and vimentin, are related to the formation of ACE2–SARS-CoV-2 complex, which is defined as the possible target of mAbs against COVID-19 (11,66).
Antibody candidates interfere with the SARS-CoV-2 replication and transcription
Preventing the biological functions of viruses, such as blocking their replication, is one of the targets of interest in producing mAbs. So far, various humanized antibodies have been produced to intrude the infected cells and inhibit viral replication in some infections caused by hepatitis C, Ebola, and influenza (90). In this regard, it has been demonstrated that cysteine-like protease (3CLpro), papain-like proteases, and even other nonstructural proteins (nsps) of novel coronavirus have an excellent potential to be targeted as suitable mAbs against SARS-CoV-2 replication (146).
Antibody candidates adjust innate and adaptive immune responses
Currently, most mAbs designed against COVID-19 target the individual's innate and acquired immune response system (Fig. 3).
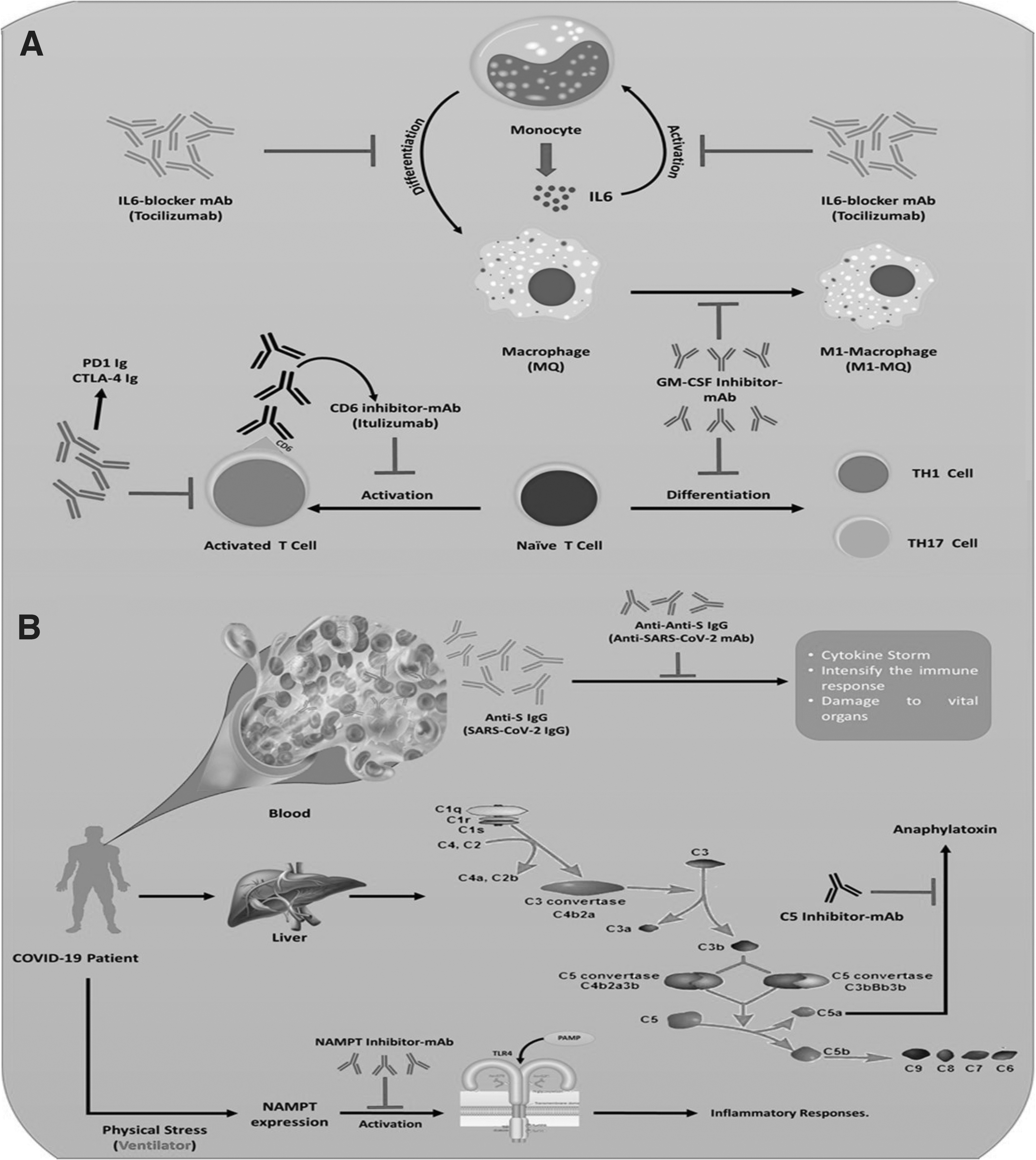
Mechanism of action of mAbs in regulating innate and acquired immune responses in COVID-19 patients.
In this context, the mediators involved in cytokine storms can be the main target
Oxygen reduction was also observed in 90.5% and 75% of COVID-19 patients, respectively (145). Moreover, several effective combination therapies using Tocilizumab have been reported recently (44,46). An interesting data from the clinical trial studies indicated that Tocilizumab could be considered for pregnant COVID-19 patients with hypoxia and hyperinflammation as a safe therapeutic option without the risk of teratogenicity (1).
Clazakizumab is another anti-IL6 mAb with a high affinity for binding to the human IL-6 (27). Another therapeutic option to modulate the immune response in COVID-19 patients is using mAbs as the GM-CSF blockers. It has been established that GM-CSF is involved in stimulating a cascade of inflammatory responses through enhancing the proinflammatory cytokines, such as IL6, IL-23, and TNF. Moreover, it can change the condition to hyperinflammation by stimulating the M1 phenotype of macrophages and the differentiation of Th1/Th17 (77,141,152). Lenzilumab and Mavrilimumab have been introduced as the anti-GM-CSF mAbs with a high affinity (27).
According to the previous experiences with SARS-CoV, researchers have been recommended TNF-α, IFN-γ, IL-33, IL-17, CD16, TLR3, G-CSF, immunoreceptor tyrosine-based activation motif, MCP1, IL4, and IL10 as the targets of interest to manufacture mAbs toward COVID-19 (67,107). In this regard, infliximab and adalimumab are the mAbs acting against TNF-α. Emapalumab (Gamifant®) is a human IgG1 mAb known to suppress both forms of free and receptor-bound IFN-γ.
Wilkinson et al. have shown that MEDI3506, as the anti-IL-33 mAb, has an excellent potential to improve respiratory disorders resulting from SARS-CoV-2 infection. mAb, which has been characterized to inhibit respiratory failure and hyperinflammation caused by COVID-19, is a fully human IgG1κ monoclonal antibody named secukinumab (Cosentyx) toward IL-17A (138). Also, for reducing respiratory dysfunction, pamrevlumab is a suitable mAb, which can regulate the connective tissue growth factor activity and its associated pulmonary edema during COVID-19 (31).
It was illustrated that physical stress induced by ventilators might increase the expression level of the nicotinamide phosphoribosyl transferase (NAMP) gene, which causes Toll-like receptor 4 (TLR4) activation in favor of the lung inflammation (14,100,106). C5a, known as anaphylatoxin and chemotaxin of the complement system, plays a critical role in the inflammatory reaction occurring during COVID-19 (64). Consequently, C5a and its receptor have been proposed to design anti-SARS-CoV-2 antibodies. Avdoralimab is a mAb with an antagonist activity for the receptor C5aR1 or CD88 (23).
Scientific evidence has shown that targeting T cells and their related CD markers or receptors by artificial mAbs is a fascinating approach to improve viral infection (16,129). For example, mAbs against c-chemokine receptor 5 (CCR5), expressed on CD4+ T cells, could be suggested in COVID-19–developed patients (99). Furthermore, restraining immune checkpoints, such as PD-1 and CTLA-4, by mAbs can regulate T-cell activity (48,97). Itolizumab is a well-known mAb that distinguishes human-activated T cells through their CD6 marker and can be administered for mild-to-severe cases of COVID-19 (20,34).
Sometimes, antibodies might be targeted by mAbs. Herein, the results of studies have shown that anti-S IgG, produced during the SARS-CoV-2 infection, has a pathological role in lung failure. Therefore, its neutralization can effectively cure the disease (15,121). IgE is the leading cause of allergies and hypersensitivity, which acts as the major player of inflammation, mainly through activating mast cells. There is a direct correlation between IgE level and the susceptibility to respiratory infections and also the severity of SARS-CoV-2 infection. It has been illustrated that anti-IgE mAbs such as Omalizumab can alleviate the severe symptoms of COVID-19 (32).
Ultimately, the results of a recent meta-analysis have shown that mAbs are helpful in reducing the morbidity caused by SARS-CoV-2 infection without any critical safety concerns (56).
IVIg for COVID-19
One of the popular immunotherapeutic methods that has attracted a wide range of attention during the last decades is antibody therapy by IVIG. IVIg is a blood product containing pooled IgG with a high varied capacity to identify microbial antigens. Hence, it can directly exert specific activity depending on the pathogen encountered by the pool's population in the human body (8).
IVIg therapy primary was administered for the patients with immunoglobulin deficiencies, but it is known as a qualified therapeutic approach to improve certain neurological, immunological, and hematological disorders nowadays. Moreover, it alleviates certain bacterial or viral infections (83,84,96,109,134). The underlying mechanism for IVIg involves inducing passive immunity through interfering with detrimental inflammatory mediators and complement components. It can block FcγRs on phagocytic cells, suppress Th1 and Th17, and enhance the number of Treg cells in peripheral blood (14,38,88).
This is a pivotal point that IVIg has a dose-dependent effect, so it should be prescribed at a suitable dosage based on the type of the disease (13,72). The risk of pathogen transmission, immediate infusion-related reactions, and the adverse effects of elevated serum IgG are the significant challenges in IVIg. In this regard, some measures could be taken to resolve these drawbacks. For example, using heat treatment (60°C), detergents, and nanofiltration has been recommended to eliminate possible microbial agents from serum as a source of antibodies (55,82).
There are valuable data that confirm the IVIg efficacy in controlling COVID-19 at the early stage of the disease (53,62,127). The case series investigations of IVIg therapy for five critically ill COVID-19 patients have shown that a high dose of IVIg administration (0.3–0.5 g/kg) for five consecutive days could alleviate the clinical manifestation of the disease (81). Moreover, Xie et al. observed that using IVIg as an adjuvant therapy within 48 h after the beginning of hospitalization in ICU caused patients to be discharged earlier, and their mechanical ventilation requirement was remarkably reduced (17,144). In addition, IVIg therapy has been reported to improve the quality of life of COVID-19 patients with lymphocytopenia (85).
Two well-known IVIg products, which have been proven for SARS-CoV-2 infection, are Gamunex®-C and Flebogamma® DIF (Grifols). These products contain specific antibodies against novel coronavirus (28). However, it is required to do more experimental and clinical trial studies to make a better judgment on the therapeutic effects of IVIg on SARS-CoV-2 infection.
Conclusion
In conclusion, due to the dangerous nature of SARS-CoV-2 for humankind, researchers worldwide have been exploring effective strategies to control this infection from the beginning of its outbreak. According to our literature review, it can be concluded that various methods based on antibody therapy are beneficial in two main aspects for managing COVID-19, including its role as a prophylaxis weapon, especially in more vulnerable persons, such as hospital staff and people with some underlying diseases. Although implementing them has multiple challenges in clinical trials, it is more cost-effective and less time-consuming than the vaccine production process.
It is proven that due to the lack of specific antiviral drugs for novel coronavirus, the administration of nAbs as a treatment option at the early stages for COVID-19 patients seems to have an accepted potential to reduce the disease exacerbation and mortality rate. Collectively, antibodies are considered a valuable source to pave the way to fight against similar pandemics in the future. Nevertheless, there are several gaps in the clinical trial level of antibody therapy for the COVID-19 that need to be filled by further investigations.
Footnotes
Authors' Contributions
N.S. and S.M. provided conception and article design; H.Z.M., H.R.J., M.R., N.SE., M.N., K.H.A., N.S., and S.M. performed collection of data; H.Z.M., H.R.J., M.R., N.SE., M.N., K.H.A., N.S., and S.M. contributed to article writing; N.S. and S.M. made important revisions and confirmed the final revision. All the authors reviewed and approved the final version of the article.
Author Confirmation Statement
H.Z.M. and N.SE. are from Birjand University of Medical Sciences (Birjand, Iran); M.R. and M.N. are from Islamic Azad university (Tehran, Iran); S.M. is from Alzahra University and Cancer Biomedical Research institute (both in Tehran, Iran); and N.Sa. is from Mashhad University, all where education and research are the primary functions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.