
Abstract
Cytokine storms can be triggered by various infectious or noninfectious diseases and cause severe damages to multiple organs. Cytokine storm plays an important role in the pathogenesis of severe cases of coronavirus disease 2019 (COVID-19). The pathogenesis of COVID-19 involves a potent inflammatory response involving a complex group of mediators, including interleukin (IL)-6 and IL-10. In this study, the serum levels of IL-6 and IL-10 cytokines were evaluated in 79 COVID-19 infected patients from the National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt. And 20 healthy individuals served as a control group. The patients were divided into moderate, severe, and critically ill. In this study, IL-6 and IL-10 levels were significantly elevated in COVID-19 patients compared with healthy controls. IL-6 levels were significantly higher in patients compared with controls (p = 0.001), although it was not varied within different severity groups except for moderate-critical ill cases (p < 0.033). IL-10 only showed a significant difference between critically ill and control cases (p < 0.002). Receiver operating characteristic curve analyses showed that IL-6 levels >120 pg/mL can predict moderate and critically ill patients with a sensitivity of 90.48% and a specificity of 62.50%, Area Under the Curve <0.0001. In conclusion, the serum levels of IL-6 cytokine are important noninvasive biomarkers to differentiate between moderate and critically ill COVID-19 infected patients.
Introduction
Coronavirus disease 2019 (COVID-19) is a clinical condition caused by a mutated RNA virus known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). After the first occurrence, in December 2019, in China, the outbreak spread exponentially across the globe; then, on the 11th of March 2020, it was proclaimed a pandemic by the World Health Organization (20).
According to the Egyptian Health Ministry tracking, the reported positive cases in Egypt during the period between the first reported case on the 14th of February 2020 and the 19th of April 2021 are 216,334 cases (2.1% of the total population of 100 million), total deaths are 12,738 cases (5.8% of positive cases), and 163,479 (75.5% of positive cases) confirmed cases have fully recovered (2a).
Although the majority of SARS-CoV-2 patients are asymptomatic or experience only mild symptoms, the infection may progress to severe respiratory illness in some cases, especially in older patients and comorbidities (8). This subgroup of patients has elevated levels of D-dimer and serum ferritin, abnormal hepatic functions, thrombotic tendency, and disseminated intravascular coagulation, which implies macrophage activation syndrome, also known as secondary hemophagocytic lymphohistiocytosis (17).
The previous laboratory studies revealed that SARS-CoV-2 is a cytopathic virus and could cause lung damage, as shown by pathological examinations (8). Although appropriate immune responses are needed to control viral infections, a hyperactive immune system might have serious consequences. In the case of SARS-CoV-2, when the virus replicates, host immune responses become triggered, which is expected to clear the infection and cure the patients. However, in some cases, patients may develop more severe illness, such as Multiple Organ Dysfunction Syndromes and the reason was unclear until recently.
Some reports hypothesized that cytokine storm, acute systemic inflammatory response, has a very important role in the pathogenesis process in severe cases of COVID-19 (3,14,17). In this regard, there are a broad range of immune-active molecules such as interleukins (ILs), and tumor necrosis factor-alpha have been suggested to contribute to the development of cytokine storm (1,18). Among ILs, IL-6 is a key pro-inflammatory cytokine released from immune cells, especially T-helper 17 (TH17) in the acute phase of COVID-19 inflammation, which results in a variety of local and systemic changes such as fever, leucocyte recruitment and activation, and hemodynamic implications (2). IL-6 is associated with rapid disease progression and higher complication risk.
Besides IL-6, IL-10 is produced by regulatory T cells and even TH 1 cells and has immunoregulatory and inflammatory roles in COVID-19 infected patients (18,21). It has been reported that IL-6 and IL-10 levels significantly rise in the cytokine storm observed in coronavirus infection (13,18). In addition, IL-6 levels in the plasma and/or bronchoalveolar lavage have been discovered as early biomarkers of lung injury and predictors of extended mechanical ventilation, organ dysfunction, morbidity, and mortality in lung disorders (19).
As cytokines could be easily measured in serum, they have been suggested as potential immunological biomarkers to predict COVID-19 progression (10). This study aims to investigate the potential role of IL-6 and IL-10 in the cytokine storm of COVID-19 and whether IL-6 and IL-10 cytokine levels can help predict disease severity in Egyptian patients with COVID-19.
Materials and Methods
Study design
This is a single-center observational study. It has been reviewed and approved by Egypt Center for Research and Regenerative Medicine Ethical Committee (IRB No. 00012517, Organization No. 0010559). All patients (n = 79) with COVID-19 enrolled in this study were diagnosed with SARS-CoV-2 infection and admitted to National Hepatology and Tropical Medicine Research Institute (Cairo, Egypt) between November 2020 and January 2021. Patients above 18 years of age have been included. Serum samples for all cases were collected immediately after hospital admission and further divided into moderate (n = 48), severe (n = 10), and critical (n = 21), according to China's novel coronavirus pneumonia diagnosis and treatment guideline (5th edition) (5,9). The detailed criteria are listed as follows: Moderate group: showing fever, respiratory symptoms, and radiological finding of pneumonia. Severe group: patients have one of the following criteria: respiratory distress, respiratory rate ≥30 times per minute; oxygen saturation at rest ≤93%; oxygen partial pressure/oxygen concentration in arterial blood ≤300 mmHg; >50% lung imaging lesion progress within 24–48 h. Critical group: patients have one of the following criteria: respiratory failure requiring mechanical ventilation, shock, and combining other organ failure requiring intensive care unit (ICU) admission.
Serum samples collected from healthy volunteers were served as controls (n = 20).
Viral detection
The nasopharyngeal swabs of all patients were used for viral RNA extraction using the QIAMP VIRAL RNA mini kit (Qiagen, Hilden, Germany) following the manufacturer's protocol. The extracted viral RNAs were quantified using a real-time RT-PCR kit (Primer Design Ltd., UK).
Cytokine assay
Levels of IL-10 and IL-6 serum cytokines were measured using human enzyme-linked immunosorbent assay (ELISA) kits (Elabscience®, Houston, TX) according to manufacturer's instructions. In brief, 100 μL of samples (or standards) were added to the micro-ELISA plate wells and combined with the specific antibody. Then a biotinylated detection antibody specific and avidin-horseradish peroxidase conjugate were added successively to each well and incubated. The substrate solution was added to each well. The enzyme-substrate reaction was stopped by the addition of stop solution. The optical density was measured spectrophotometrically at a wavelength of 450 ± 2 nm. The sensitivity of the assay was 4.69 pg/mL for both IL-6 and IL-10.
Further laboratory analyses, including white blood cell, hemoglobin, platelets, and creatinine, were assessed.
Statistical analysis
Data were not normally distributed, so data were expressed as median and interquartile range. For comparative analysis, nonparametric Mann–Whitney or Kruskal–Wallis tests were performed using GraphPad Prism 9 (GraphPad Software, San Diego, CA). Receiver operating characteristic (ROC) curve analysis was used to assess the diagnostic performance using MedCalc Statistical Software (Version 14.8.1). A p-value <0.05 indicates statistical significance.
Results
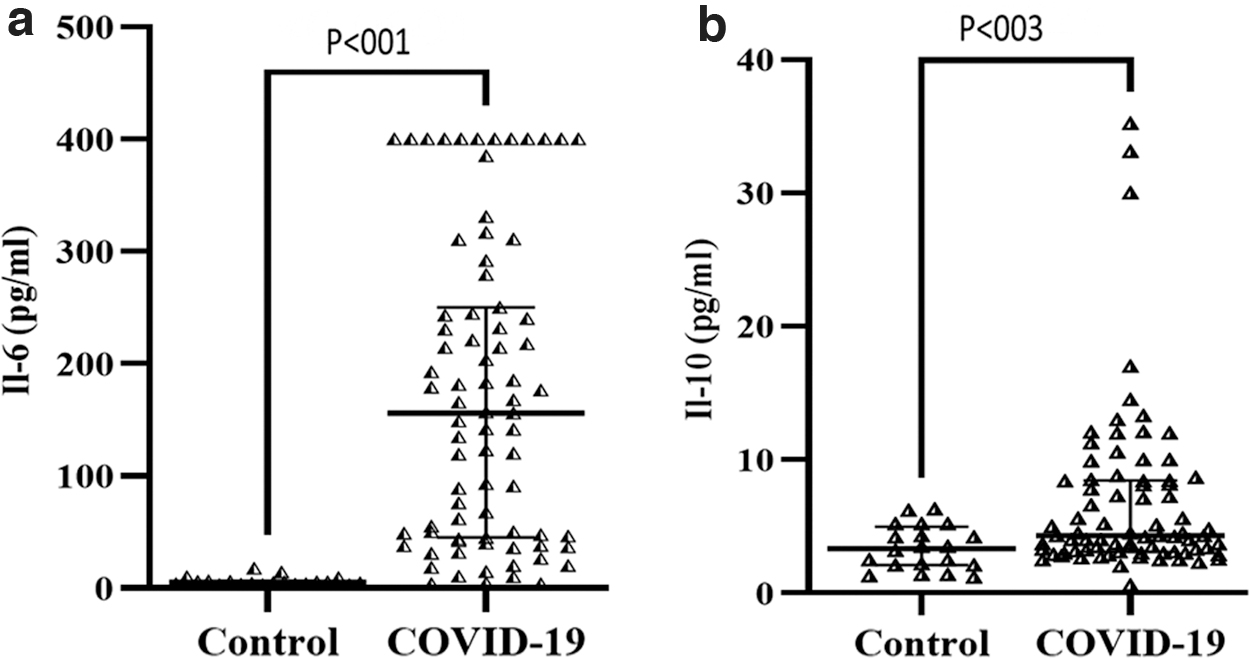
The baseline characteristics of patients and controls are presented in Table 1. In this study, a total of 79 patients were enrolled, including 45 (57%) males and 34 (43%) females, median age 52 years (interquartile range [45, 60]). Patients were divided into moderate (n = 48 [60.76%]), severe (n = 10 [12.66%]), and critical (n = 21 [26.58%]). Thirty-two patients (40.51%) were admitted in the ICU. Total number of deaths in the study = 33 patients (41.77%). First, the serum levels of IL-6 and IL-10 were evaluated in the control group versus the COVID-19 infected patients. As shown in Figure 1, our data revealed that IL6 and IL-10 levels were significantly increased in COVID-19 patients than in healthy individuals (median IL-6 = 156 vs. 5.35, p < 0.01; median IL-10 = 4.30 vs. 3.35, p < 0.003, respectively).
Serum concentration of
The Baseline Characteristics of Patients and Controls
Hb, hemoglobin; ICU, intensive care unit; IQR, interquartile range; WBC, white blood cell.
We further compared different severity groups (moderate, severe, and critically ill) versus each other and versus control in terms of the concentration of IL-6 and IL-10. Figure 2a showed that there were significant differences (p < 0.001) between each severity group and healthy control in IL-6 concentration; however, there were no significant differences in between the different severity groups except for moderate-critical ill cases (p < 0.033). For IL-10, the only significant difference was detected between critically ill and control cases (p < 0.002) as shown in Figure 2b.
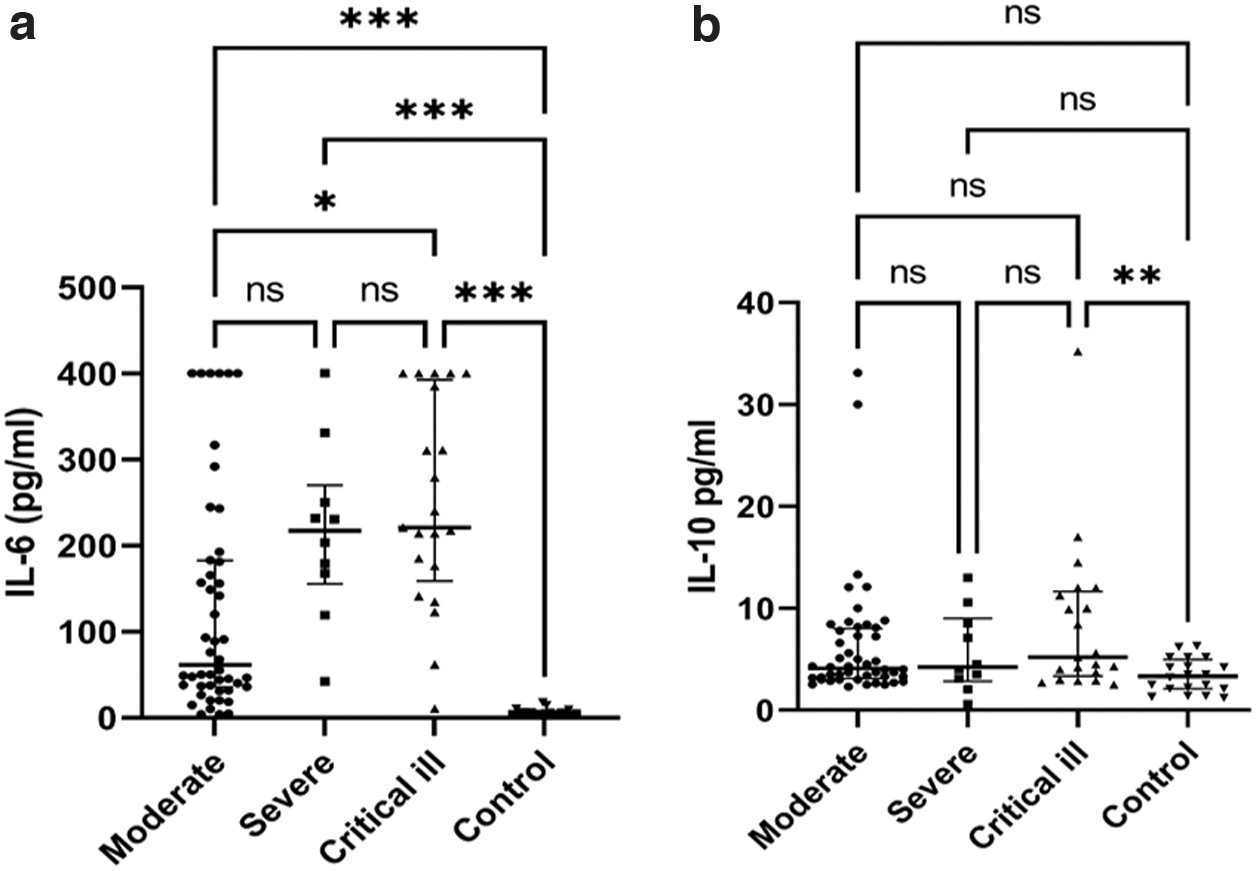
Concentration of inflammatory cytokines IL-6
To evaluate the diagnostic value of IL-6 and IL-10 for COVID-19 patients, ROC curves were calculated from 79 COVID-19 infected patients and 20 healthy controls (Fig. 3). The Area Under the Curve (AUC) of IL-6 was larger than that of IL-10 AUC = 0.972; 95% confidence interval [CI] = 0.917–0.994; p < 0.001). The concentration of IL-6 > 17.6 pg/mL was the optimal cutoff value for predicting COVID-19 infection (sensitivity = 92.41% and specificity = 100%). The AUC of IL-6 was larger than that of IL-10 (AUC = 0.717; 95% CI = 0.618–0.803; p < 0.0007). The concentration of IL-10 > 2.5 pg/mL was the optimal cutoff value for predicting COVID-19 infection (sensitivity = 92.41% and specificity = 45%).
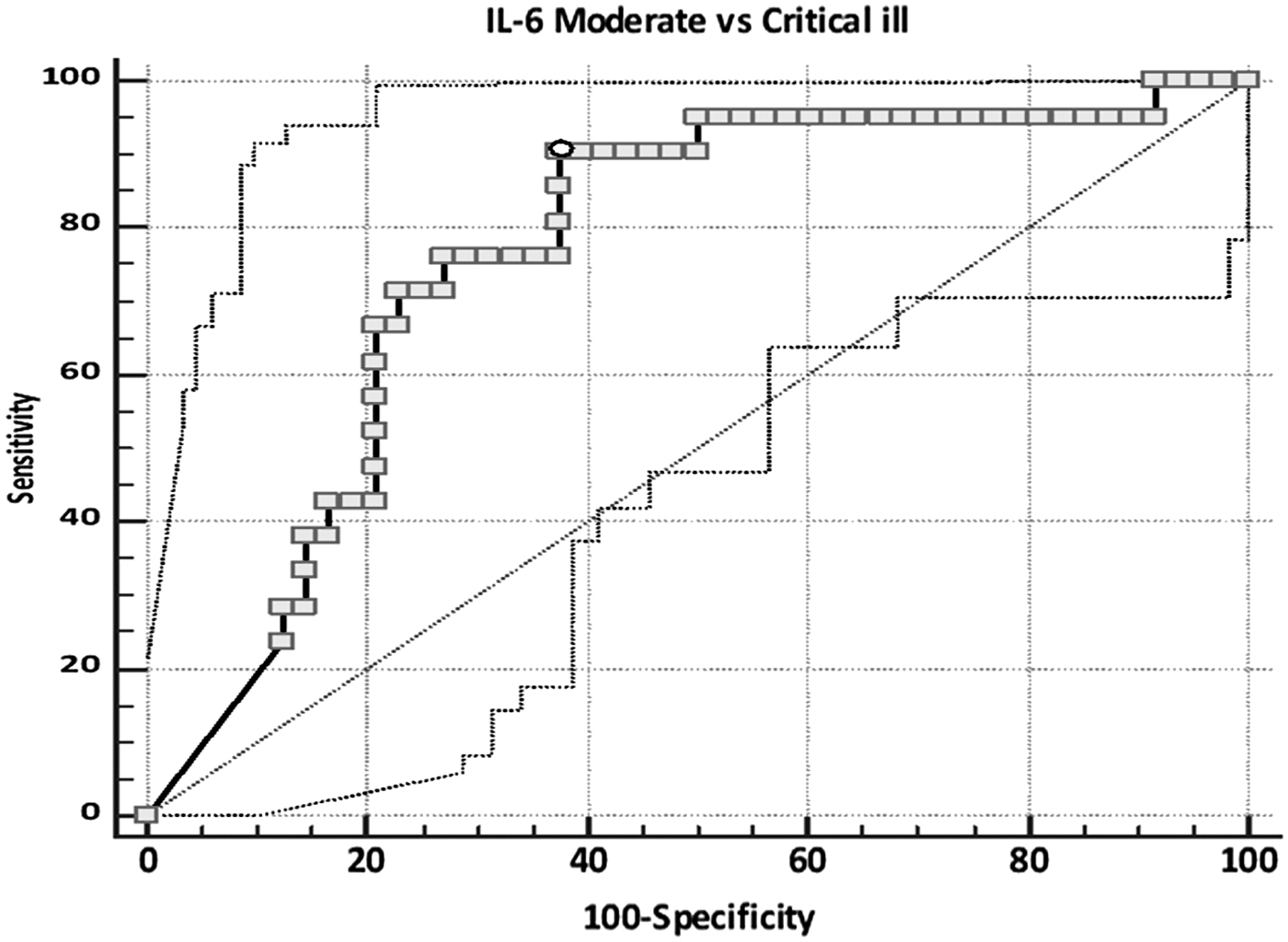
Receiver operating characteristic curve of IL-6 in moderate (n = 48) and critically ill (n = 21) COVID-19 patients.
ROC curve analysis reveals that IL-6 levels of >120 pg/mL can predict the moderate and critically ill individuals with 90.48% sensitivity and 62.50% specificity (AUC = 0.763; 95% CI = 0.645–0.857; p < 0.0001; Fig. 3). However, differentiating between moderate and severe and between severe and critically ill was not applicable.
Discussion
SARS-CoV-2 infection is currently a leading global pandemic. It is responsible for about three million deaths around the globe (22). In this study, hospitalized COVID patients were divided into moderate (n = 48 [60.76%]), severe (n = 10 [12.66%]), and critical (n = 21 [26.58%]). In agreement with Xu et al. (23), that divided 88 hospitalized patients into moderate (47 [53.41%]), severe (32 [36.36%]) and critically ill (9 [10.23%]) groups according to the classifying criteria (5). Although most cases were considered subclinical or mild, 14% of the reported cases were severe, including severe pneumonia and breath shortness.
Besides, 5% of COVID-19 patients were critical cases. These patients have developed respiratory failure, septic shock, and multiorgan failure, which may result in death (5). Clinical studies have observed a link between serum levels of pro-inflammatory and anti-inflammatory cytokines and COVID-19 severity (15), suggesting that the early inflammatory response may have a potential role in the disease deterioration and also could be a useful tool for the early management of patients with severe forms.
IL-6 and IL-10 are key inflammatory cytokines. IL-6 is a cornerstone pleiotropic mediator in various inflammatory processes such as tissue damage and infection. During viral diseases, including COVID-19, IL-6 and IL-10 are produced at the sites of tissue inflammation and released into the circulation by a range of different cells, including macrophages, lymphocytes, fibroblasts, endothelial, and epithelial cells. Once produced, these cytokines increase blood flow near the infection site and activate macrophages and other phagocytic cells for clearance of virus, as well as infected cells (16). Moreover, The SARS-CoV-2 virus triggers both innate and adaptive immune responses, resulting in the production of IL-6 and other cytokines, increased vascular permeability, and respiratory failure (4). The fact that IL-6 is primarily produced by injured lungs could explain the observed correlations between cytokine levels and oxygen requirements.
Similarly, in this study, inflammatory cytokines, including IL-6, IL-10, were significantly increased in COVID-19 patients compared with healthy controls, suggesting the activation of the immune response against SARS-CoV-2 infection.
In contrast, IL-10, is an anti-inflammatory cytokine that regulates both innate and adaptive immune responses and, therefore, suppressing pro-inflammatory signals and preventing tissue damage (7). Therefore, during the acute phase of viral infection, the activity of T cells, macrophages, and natural killer (NK) cells has been suppressed by the IL-10. Despite the essential role of these cells in viral elimination, they are also involved in the tissue damage process. Hence, IL-10 may prevent successful viral elimination while minimizing collateral tissue damage. Thus, the balance between the levels of IL-6 and IL-10 cytokines in serum may be a valuable tool to predict disease severity (11,12). Similar to our results, many studies have reported the elevation of both IL-6 and IL-10 levels in some COVID-19 patients and this cytokine imbalance can predict disease severity in those patients (5,6,12).
This study revealed no significant difference in IL-6 concentration between moderate and severe cases; however, there was a significant increase between critically ill and moderate patients so that it can be used as a differentiating parameter between them. Since IL-6 has higher sensitivity (90.48%) and lower specificity (62.50%), it could be used to confirm the diagnosis rather than decline it (good positive test).
We noticed that IL-6 could achieve significant differences between moderate and critically ill groups, whereas IL-10 did not, and these findings were consistent with previously published literature (5). IL-10 also did not give any significance between moderate and severe, which also matches with Han et al. (5). In contrast, no significant difference was detected between the severe and critically ill groups, which could be due to the limited sample size.
This study has two limitations. First, all subjects enrolled in the study were from one center with inevitable selective bias. Second, not all laboratory tests were done on all patients. The inhibition of the IL-6 signal could provide a potential treatment for hospitalized patients with COVID-19 due to the involvement of IL-6 in the inflammatory process.
Conclusion
The serum levels of IL-6 cytokine are important noninvasive biomarkers to differentiate between moderate and critically ill COVID-19 infected patients.
Footnotes
Authors' Contributions
Study concept and design by R.M.D., L.M., and M.S. Acquisition of laboratory data by R.M.D., L.M., and R.S.A. Analysis and interpretation of data by R.M.D. and M.S. Literature search by R.M.D. and M.H.E. Drafting of the article by M.H.E. and R.M.D. Editing in the article by L.M. Critical revision of the article for important intellectual content by R.M.D. and L.M. Sample collection and clinical evaluation by L.M., R.S.A., and A.F. Statistical analysis by M.H.E. L.M.: Conceptualization (equal), resources (equal), writing review and editing (equal), visualization (lead), and data curation (lead). M.S.: Resources (equal), project administration (lead), supervision (equal), and funding acquisition (lead). R.S.A.: Resources (equal), methodology (supporting), visualization, and data curation (supporting). A.F.: Resources (equal), methodology (supporting), visualization, and data curation (supporting). M.H.E.: Software (lead), formal analysis (lead), and writing original draft (supporting). R.M.D.: Conceptualization (equal), methodology (lead), writing original draft (lead), investigation (lead), validation (lead), writing review and editing (equal), and supervision (equal). All authors read and approved the final article.
Author Agreement/Declaration
All authors have seen and approved the final version of the article being submitted. All authors confirm that this work is original and that all data, tables, and so on used in the article were prepared originally by the authors and have not been published elsewhere, nor is it currently under consideration elsewhere.
Author Disclosure Statement
All authors have none to declare.
Funding Information
No funding was received for this article.