
Abstract
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is responsible for the COVID-19 pandemic. COVID-19 has a broad clinical spectrum from asymptomatic patients to multiorgan dysfunction and septic shock. Most of the common symptoms of COVID-19 are classified as respiratory disorders, but some reports show neurological involvements. During the COVID-19 pandemic, a case series of neurological complications, such as Guillain–Barré syndrome (GBS), were reported. GBS is a neuroimmune disorder with acute inflammatory radicular polyneuropathy in different parts of the peripheral nerve. Some studies have reported GBS as an inflammatory neuropathy related to various viral infections, such as cytomegalovirus (CMV), Epstein–Barr Virus (EBV), herpes simplex virus (HSV), human immunodeficiency virus (HIV), influenza, and Zika virus. There are some immunomodulation approaches for the management of GBS. Studies have evaluated the effects of the various therapeutic approaches, including intravenous immunoglobulin (IVIG), plasma exchange (PE), complement inhibitors, and corticosteroids to regulate overactivation of immune responses during GBS in experimental and clinical studies. In this regard, the possible association between GBS and SARS-CoV-2 infection during the outbreak of the current pandemic and also the mentioned therapeutic approaches were reviewed.
Introduction
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is responsible for the COVID-19 pandemic. It originated from Wuhan, China, in December 2019 and continues to spread in the world quickly (104). COVID-19 has a broad clinical spectrum from asymptomatic patients to multiorgan dysfunction and septic shock. Indeed, the disease can be divided into mild, moderate, severe, and critical stages. Some common symptoms of COVID-19 are fever, dry cough, diarrhea, and fatigue. Severe symptoms lead to acute respiratory distress and septic shock (27,51).
Guillain–Barré syndrome (GBS) was recognized for the first time in 1916 by French physicians, Guillain, Barré, and Strohl (117,139). GBS is mostly considered as a postinfectious disease and investigation of the history from GBS patients has shown that about 50% of them have experienced a specific kind of preceding infection that Campylobacter jejuni causes at least one-third of these infections. Other types often have been related to microorganisms, including cytomegalovirus (CMV), influenza A, Epstein–Barr virus (EBV), Mycoplasma pneumonia, and Haemophilus influenzae (126). Interestingly, the increasing number of GBS case reports that occurred in SARS-CoV-2 pandemic may show the possible link between SARS-CoV-2 and GBS, and it also raised concerns in the world (1).
GBS is the most important cause of acute flaccid paralysis and incidence of this syndrome is 1–2 cases per 100,000, annually with the mortality rate 3–10% in patients who developed respiratory failure and cardiac arrhythmias (74). GBS may occur at any age (89), but it is more common in adults and males (139). The most common clinical symptoms are the lack of reflexes, the weakness of motor, and paresthesia with sensory deprivation (10). Patients usually have neurological symptoms, and pain starts from the lower limbs to the upper limbs (74). Moreover, weakness in GBS patients has a pyramidal distribution, with ankle dorsiflexion and pain in arms more severe than shoulder abduction (139). GBS is often with respiratory failure, and it makes mechanical ventilation necessary. Reports showed that about 20–30% of patients with GBS need respiratory support (4,36,55,132). The differential diagnosis will be made after ruling out other diseases with these symptoms, according to serological, immunological, and electrodiagnostic tests (120).
This neural disorder has several subtypes with different immunological mechanisms. Antibodies against the peripheral nervous system (PNS) gangliosides were defined as the most common and essential elements of neuron damages (138). Furthermore, it has been clear that gastroenteric and respiratory infections can induce this disease (101,139) and that antimicrobial produced antibodies eventually crossreact with PNS gangliosides during infections (89). Besides, another explanation of this situation is activated macrophages, whose role in myelin destruction has been shown by electron microscope images. Indeed, activated macrophages produce cytokines and free radicals that can damage myelin and axon (15,71). Also, activated cytotoxic T cells (CTL) producing proinflammatory cytokines cause degradation of myelin and Schwan cell demyelination (11).
It has been recorded that although most of the common symptoms of COVID-19 are classified as respiratory disorders, some reports showed neurological involvement such as headache, dizziness, seizure, neck stiffness, stroke, and insomnia, which are simple signs of viral neurotropism (39,134,137). As the COVID-19 outbreak started, some neurological complications, such as GBS, were also reported (39,134). GBS is one of the severe complications that should be considered important. In this review article, the immunopathogenesis of GBS and its association with viral infections, the possible link of SARS-COV-2 with GBS, and immunomodulatory therapeutic approaches are discussed.
Immunopathogenesis of GBS
According to the clinical symptoms, the underlying pathology, and neurophysiological characteristics, GBS is classified into different subtypes, of which acute axonal motor neuropathy (AMAN), acute inflammatory demyelinating polyneuropathy (AIDP), acute motor sensory axonal polyneuropathy (AMSAN), and Miller Fisher syndrome are the most common subtypes (143). It causes chronic disorders, such as chronic inflammatory demyelinating polyneuropathy (CIDP), and multifocal motor neuropathy polyneuropathy.
These disorders are linked to monoclonal gammopathy (with or without anti-myelin-associated glycoprotein antibodies or anti-MAG) and neuropathies (102). Although it may be known as a postinfection disorder, there are many cases of GBS patients who were not infected with GBS-associated viruses or bacteria. On the other hand, there are cases of GBS patients who were infected with strains of C. jejuni with no molecular mimicry to self-antigens (58,115). It is revealed that microbial agents such as EBV, CMV, Herpes simplex virus (HSV), human immunodeficiency virus (HIV), Zika virus, Influenza A, and C. jejuni can induce the immune system and cause GBS (101,143).
Classical complement activation leads to demyelination of nerve cells through membrane attack complex (MAC) (C5b-C9), inflammation produced by anaphylatoxins (C3a and C5a), and infiltration and invasion of macrophages producing cytokines such as tumor necrosis factor-α (TNF-α), as well as free radicals such as nitric oxide. Crossreactive antigens are recognized by components of the immune system such as macrophages and T CD4+ cells that help B cells to turn into plasma cells and produce neutralizing antibodies that may react with gangliosides as autoantibodies. Macrophages with Fc receptor and complement receptor for C3b can also damage the PNS by receptor-mediated phagocytosis and induction of myelin destruction. Infiltration of activated T CD4+ cells can enhance the activity of macrophages through inflammatory cytokines such as interferon gamma (INF-γ) and TNF-α. It can lead to the demyelination of PNS and GBS symptoms (92) (Fig. 1).
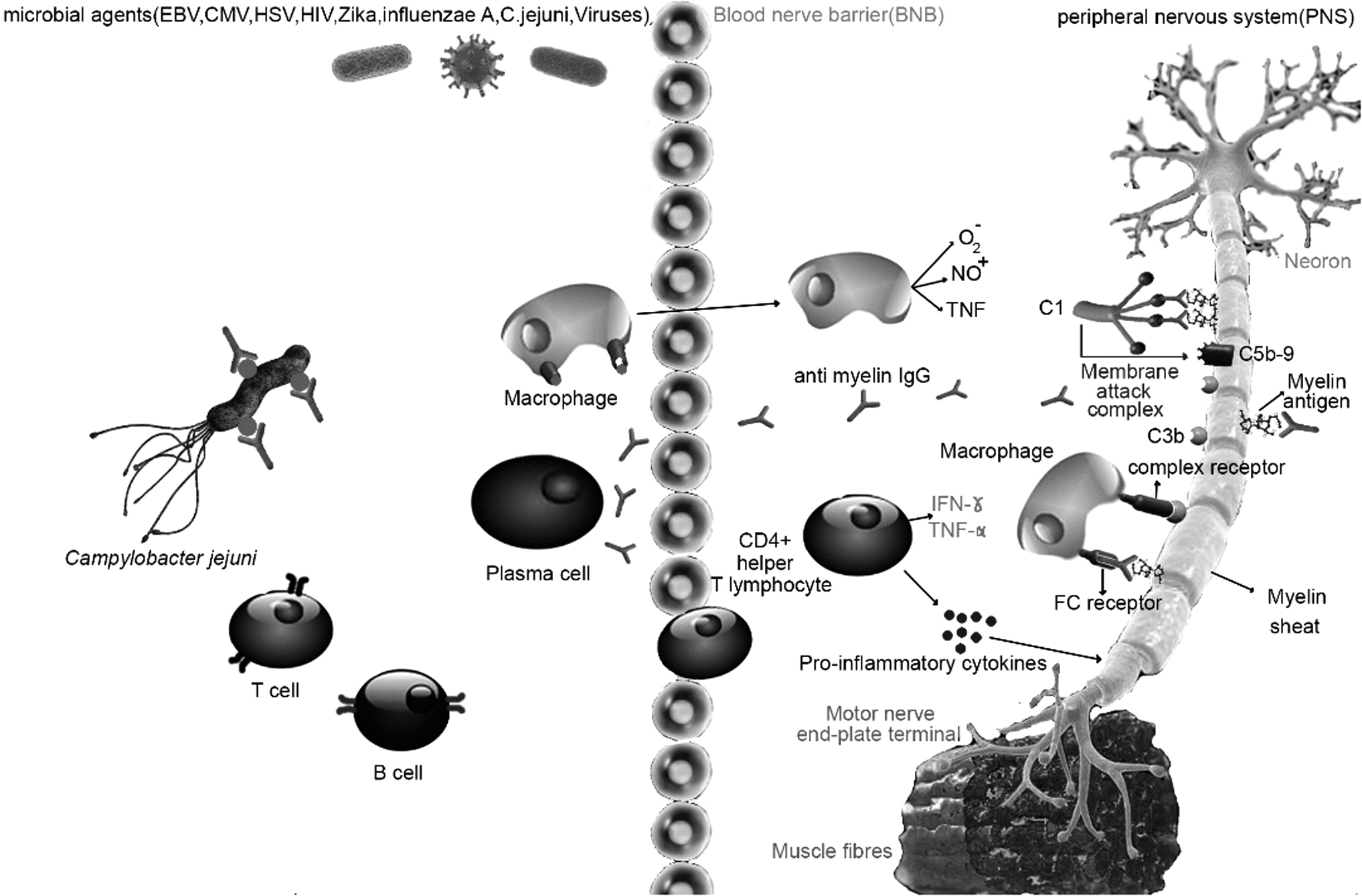
Immunopathogenesis of GBS. Some infectious agents can evoke immune system responses and cause GBS. Complement activation, macrophages infiltration, inflammatory cytokines cause tissue damages in the PNS. Crossreactive antigens are recognized by B and T cells for antiganglioside antibody production (autoantibody production). Besides, macrophages expressing FC receptors and complement receptors facilitate myelin destruction based on receptor-mediated phagocytosis. Autoreactive activated T cells (TCD4+) produce inflammatory cytokines such as TNF-α and INF-γ that lead to myelin damage and further activation of macrophages. Ag, antigens; BNB, blood–nerve barrier; CMV, cytomegalovirus; EBV, Epstein–Barr virus; HIV, human immunodeficiency virus; HSV, herpes simplex virus; INF-α, interferon-alpha; MAC, membrane attack complex; MQ, macrophage; NO, nitric oxide; O2−, superoxide; PNS, peripheral nervous system; TNF-α, tumor necrosis factor-alpha.
According to the studies, different T cells in response to myelin-derived proteins and gangliosides are involved in the GBS pathogenesis. In some cases, infiltration of T cells in the peripheral nerves, increasing of the circulating T cells, and the overexpression of the interleukin 2 (IL-2) and interleukin 2 receptor (IL-2R) have been reported in the GBS patients (19,32). However, most of the studies have been focused on the humoral responses rather than the T cell-mediated responses. Alternatively, most evidence showed that patients who received intravenous immunoglobulin (IVIG) and plasma exchange (PE) could improve, approximately. Therefore, B cell-mediated immune responses seem to have a dominant role in GBS immunopathology (129). Conflicting data about T helper 1 (Th1) and Th2 responses during GBS. While most of the studies believe in the central role of Th1 responses during the acute phase, the others believe in the similar role of Th1 and Th2 responses during the early stages. However, some other studies determined the role of Th2 responses within recovery time.
Based on some reports, cytokines that have been produced by Th1 cells are detectable at the early stages of the disease, and cytokines of Th2 cells can be recognized at the recovery stages, which highlights the hypothesis as mentioned earlier (115,116). Th1-associated cytokines increase in the acute phase and can lead to more polarization of naive T cells to Th1 cells. No T cell reactivity has been found against P0, P2, and PMP22, whereas some evidence has confirmed the Th1 expansion-related anti-GM1 accompanied by producing IFN-γ. By decreasing cytokines, including interleukin 1 beta (IL1β), IFN-γ, and TNF-α at the recovery phase, Th2 cytokines begin to rise (81,114).
Based on findings presented in other studies, increased extent of IL-17 and IL-22 was detected in serum as well as cerebrospinal fluid (CSF) in response to intense expression of RAR-related orphan receptor gamma (RORγt) and signal transducer and activator of transcription 3 (STAT3) in Th17 immune cells, which is reversible by IVIG treatment. It should be noted that T follicular helper 2 (Tfh2) and Tfh17 immune cells, which play a critical part in B cell maturation, and increase during GBS (93,116).
It has been illustrated that T cells proliferate in response to nonprotein antigens named Tγt, which play a stimuli role for natural killer cell (NK cell) expansion and surface receptor expression, in addition to IL-4 secretion. These T cells can infiltrate myelin sheath and be a part of antibody production against ganglioside-like epitopes (28). Many T cell subtypes, including T regulatory cells (Treg) participated in self-tolerance, have a regulatory function in GBS. Furthermore, reduction of Treg numbers during the acute phase of the disease (Human leukocyte antigen-DR isotype or HLA-DR+ and Fokhead box protein P3 or FOXP3+ Treg cells) has been recorded in several studies. One of the significant molecules involved in self-tolerance is cytotoxic T-lymphocyte-associated protein-4 (CTLA-4) expressed on Treg cells and gets affected by GBS, conversely. Also, there is another key molecule named B7 expressed on the wide range of immune cells responding to CTLA-4. It gives a united response that results in self-tolerance. Therefore, dysregulation of these molecules might cause autoimmune diseases, such as GBS (33,88).
One of the main immunopathological reasons for GBS is humoral immune responses due to the molecular mimicry related to preceded infections such as CMV, C. jejuni, and H. influenza. It has been found that there is a structural similarity between lipo-oligosaccharide structures (LPS) of infectious microorganisms and human gangliosides that can lead to crossreactivity through B cell and likely T cell (58). Postinfection autoantibodies such as IgG3 and IgG1 react against GM1 or GD1a and cause reversible neurological disorders (68).
It should be noted that different gangliosides can be affected by different infections. For instance, CMV infection causes autoantibodies against GM2 (9,58). Moreover, the heterogeneity of gangliosides leads to various forms of GBS with different clinical circumstances. Interestingly, all the infections, which may cause GBS are common, but not all the infected patients suffer from GBS. Therefore, there might be a relation between individual susceptibility and GBS, such as epitopes, which T cells detect as immunogenic sites (58). After antibody binding to the peripheral nerves, complement gets activated and also macrophages are infiltrated through the spinal–blood barrier (22).
Released cytokines and induced endothelial cells take part in facilitating leukocyte migration to the peripheral nerves. Antigangliosides are the most common type of antibodies detected in the major percent of AMAN patients compared with AIDP patients (138). High titers of LPS-specific IgM antibodies gained affinity maturation through T cell-independent pathway, which is vital for GBS manifestations, based on reports. Nonetheless, other antibodies, such as IgA and IgG, have been detected in sera of GBS patients besides IgM (64).
Reviewing the history of agents and their immunopathogenic mechanisms involved in the development and exacerbation of this neuroinflammatory disease are helpful to choose an appropriate therapeutic approach to overcome this disorder during the emergency viral pandemic like SARS-CoV-2. Nerve damage in GBS can be mediated through stimulation of various immune responses by some of the viruses. As an explanation, it was demonstrated that CMV is the most important viral cause of GBS. The incidence of CMV-related GBS has been reported about 0.6 and 2.2 per 1,000 cases of primary CMV infection (100). Steger et al.'s study illustrated the elevated levels of anti GM1, GM2, and GQ1b in CMV-GBS patients (117).
These gangliosides express on PNS and crossreaction between CMV glycoproteins and gangliosides is probable because of their similarities. Some studies have been reported that infectious fibroblasts express epitopes that are like gangliosides and can be recognized by anti-GM2 (101). On the other hand, CTL counts in CMV-GBS patients in progressive and plateau phases are increased. Khalili et al. have shown elevated levels of anti-GM2 in CMV-GBS patients compared with GBS patients without CMV, but this antibody has not been detected in CMV patients without GBS (62). Moreover, crossreaction in primary infection is more probable than the recurrence infection (118).
The production of autoantibody against gangliosides has been observed in the infection by HSV. High-serum titers of HSV-1 anti-GQ1 b IgG and molecular mimicry can lead to inflammation and damage nerves (9,37,149) by changing the glial and neuronal surface molecules' composition, such as gangliosides that can result in GBS (83,143). In addition, in patients with Zika virus, crossreaction between specific antibodies against the virus with neurons, which leads to induce GBS, has been reported as the most recent infection concerning GBS (14,73). Moreover, high levels of viral loads can stimulate the generation of proinflammatory antibodies that increase the risk of GBS (9). Another GBS-correlated viral infection is caused by EBV. This virus may infect nerves and damage them, directly (122) and cause vasculitis by complex-mediated vessel inflammation, which leads to neural damage. The role of humoral immunity has been suggested after AntiQ1b detection in the serum of EBV patients. Indeed, it has been discovered that there is a homology between microbial sequence and p0 protein of myelin in 54–58 amino acids (101).
Furthermore, detected IgM against LM1, and GM1 may play a part in neuropathy occurrence (26). There is another hypothesis in EBV-GBS cases that EBV infection may cause GBS by disturbing the balance of B cell proliferation (16). In the following, influenza virus is a member of the Orthomyxoviridae family that can increase the risk of GBS up to 16–18 times (52). Although, influenza-related GBS is rare and usually leaks out in influenza outbreaks. It seems other mechanisms, except humoral immunity, are effective in this phenomenon and antiganglioside antibodies have no significant role (40,113). However, other studies explained that a lipid bilayer of influenza A envelope consists of some glycoproteins, such as hemagglutinin and neuraminidase. It revealed the possibility that during the infection, the antiglycoprotein antibodies are produced, and the molecular similarity between glycoproteins of influenza virus and those located on the human peripheral nerves lead to damages of these cells (143,146).
Another viral infection, which could be GBS inducer, is HIV (18). Correlation between HIV infection and lots of neuropathies has been described during the last decade (91). GBS usually appears in the acute phase, viremia recurrence, and after IVIG injection (101). Increasing the levels of TNF-α nerve trunk suggested that HIV infection can cause nerve injury. In this manner, severe HIV infection opportunistic pathogens such as CMV begin to appear, and it may be a route for neurological damage during the HIV infection (20).
GBS and COVID-19
The SARS-CoV-2 causes a wide range of complications, such as neuroinflammatory disorders. It can inflame the detrimental immune responses, which lead to nervous system damages and postinfection neural diseases, such as GBS. Evidence has illustrated the correlation between infection by corona viruses and possibility of GBS occurrence. The AMAN and AIDP cases have been reported after SARS-CoV-1 and MERS-CoV infections (56,63,124). In this regard, the possible association between this neuroimmune disorder and SARS-CoV-2 infection cannot be ignored. Multiple cases of GBS have been reported since the outbreak of the current pandemic (6). There is some growing evidence of neurological complications of COVID-19, including headache, febrile seizures, polyneuropathy, encephalopathy, stroke, and acute peripheral nerve disease (107,119).
However, the mechanism and possibility that this virus can induce antiganglioside antibodies causing GBS is unclear (13). In critical COVID-19 patients, predicting the time and phase of GBS is not possible, but some cases of previous studies illustrated the time interval of 5–24 days between COVID-19 clinical presentations and GBS (119). So far, several cases of COVID-19 patients who showed GBS symptoms have been reported (2,38,77,96,107,108,134,137,153). It has been recorded in some cases of GBS in countries such as Italy, Iran, Spain, USA, UK, France, Switzerland, Germany, Austria, Brazil, Canada, China, India, Morocco, Saudi Arabia, Sudan, the Netherlands, and Turkey that most of them had shown GBS after COVID-19 infection and more than 70% of them recovered after IVIG. In these cases, the data showed the resemblance of classic, the COVID-19, and Zika-associated GBS.
In addition, there was no RNA of viruses in CSF and the response to IVIG therapy illustrated the immune-associated mechanisms of postinfections rather than parainfections. In addition, it was observed that most people with GBS were symptomatic COVID-19 patients, but there were some cases of asymptomatic COVID-19 patients who made it urgent to take SARS-CoV-2 diagnostic tests from suspected people during COVID-19 outbreak. Moreover, variable data of biochemical and hematological results, such as IL-6, IL-1, IL-8, CRP, TNF-α, LDH, ferritin, thrombocytosis, leukocytosis, thrombocytopenia, leucopenia, ESR, and fibrinogen, were reported and it was shown that most people did not have anti-GD1b and anti-GM1 antibodies expected of the two cases (3).
COVID-19-related GBS patients mainly experienced severe disease symptoms like pneumonia and interstitial pneumonitis (CT chest) that the mean time of GBS clinical presentation was 5–14 days (46). However, it should be noted that some patients may have an overlap of symptoms that could mask GBS in COVID-19 patients (120).
GBS can arise in both asymptomatic and moderate COVID-19 patients (106). The nerve conduction is AMSAN, AIDP, and AMAN, and caudal nerve root increase is reported in these patients. Areflexic quadriparesis is the most common clinical presentation of COVID-19-related GBS. Moreover, initial symptoms of GBS in these patients are lower limb weakness, facial weakness, and paresthesia. Usually, older people and males constitute the most affected with COVID-19-related GBS. Preceding illnesses such as hyposmia and ageusia, dyspnea, cough, and fever were observed in these cases, of which ageusia and dyspnea were the unique symptoms of COVID-19-related GBS. IVIg therapy and prescription of drugs, such as Lopinavir, Ritonavir, Azithromycin, and HCQ, are recommended to decrease the dysphagia, weakness, and duration of ICU hospitalization in patients (46).
In addition, the damages of tissues caused by the immune response such as cytokine storms (enhancement of IL-6 level), an increase of T cells, macrophages, and endothelial cells resulted in vascular leakage, complement activation, coagulation, and even death (79). In the following paragraphs, it aimed to provide a review of published data of case reports and case series related to COVID-19-related GBS.
Valuable data from a review article that investigated 37 GBS patients with a history of coronavirus infection have shown that about 65% of COVID-19-related GBS cases belonged to the male gender and also the mean age of the patients and mean time from COVID-19 manifestation to GBS symptoms was 59 years and 11 days, respectively. The severity of GBS symptoms and the clinical complications of the disease in these cases were not different from patients with no history of COVID-19. Demyelinating was defined as the specific clinical or electrodiagnostic (EDX ( pattern in about 50% of patients. The recommended treatment approach for patients was the single course of IVIG, which led to improve most of the patients, approximately within 8 weeks (24).
Biassoni et al. report the case of a 79-year-old man with approved SARS-CoV-2 infection who was hospitalized and showed symptoms of dysautonomia after 10 days. In this case, GBS was confirmed as the cause of his neurological manifestations after monitoring. We think his study could be a suggestion to strengthen the possibility of a link between GBS and COVID-19 (16).
The other case report in this regard is about a 67-year-old female with relevant GBS-neurological presentation, including rapidly progressive quadriparesis, paresthesia, and low back pain, and that there is no report of neuropathy in her medical history. She was tested for SARS-CoV-2 infection by RT-PCR test because of her symptoms such as nonproductive cough, nausea, and anorexia, which manifested a few days period of complaints related to neurological disorders. According to the positive result of RT-PCR and neurological evaluation, which revealed hyponatremia, coagulopathy, and neuromuscular respiratory failure, this patient is the highlighted case of COVID-19-induced GBS (2).
One of the other case report studies that increase the concern toward the significant association between COVID-19 and GBS is the study done by Nejad et al. They recorded a case of SARS-CoV-2-infected patient with confirmed acute GBS who died and the cause of death was cardiac arrest due to autonomic dysfunction despite receiving IVIG and respiratory support (90).
GBS symptoms, such as lower limb weakness, paresthesia, and facial diplegia, were also reported after COVID-19 infection in 5 Italian patients (123). In another study, one patient with symmetrical weakness in the four limbs accompanied by sensitivity alteration at the distal level, progressive intensity, and motor disability was introduced by Galán et al. Their patient represents these neurological disorders followed by SARS-CoV-2 infection. Therefore, this case can display the possible correlation between GBS and COVID-19 (41).
Arnaud et al. indicated another probable case of post-COVID-19 GBS. He was an old male patient who complained of neuronal disorder, including apyretic areflexia, progressive lower limb weakness, and severe flaccid paraparesis specially in proximal muscles about 1 week after recovery from SAR-CoV-2 infection (12).
A couple of studies also described two older men ages 57 and 72 years, respectively, with GBS-associated symptoms, including acute motor-sensory axonal neuropathy for case 1 and acute progressive and ascending lower limb weakness for case 2, after SARS-CoV-2 infection (60,154). Meshref et al., reported manifestation of the neurological disorder, including difficulty in swallowing and acute quadriparesis of both upper and lower limbs in the young female who was infected by SARS-CoV-2. The severity of her symptoms attenuated after treatment (80).
Case report studies on the Iranian society have also shown neurological complications associated with COVID-19.
For instance, Mozhdehipanah et al., introduced 4 elderly patients (3 men and 1 woman) with confirmed COVID-19, who represented GBS-related complications 21–30 days after onset of SARS-CoV-2 symptoms. They suffered from lower limb weakness, facial paresis, and paresthesia controlled by using therapeutic approaches, including IVIG therapy for three of them and PE for one case. In another similar study, two COVID-19 male patients (43 and 65 years of age) were reported who display neural disorders about 18 and 10 days after diagnosis of their SARS-CoV-2 infection (87).
Ellul et al. indicated in their study that SARS-CoV-2 could infect the CNS and PNS (39). Nearly, 2/3 of GBS patients complained of SARS-CoV-2 infection about 6 weeks before their GBS-related clinical symptoms. Likewise, a case report in London illustrated GBS symptoms in a patient a week after symptoms, such as cough and myalgia (137). Parainfectious neuropathies may occur due to the overreaction of the immune system or direct effects of microbial implication.
In a case series associated manifestation in Italy, 5 patients with GBS and COVID-19 were diagnosed, and antiganglioside antibodies, including anti GM1, GM2, GM3, GD1a, GD1b, GT1b, and GQ1b, were evaluated. However, the result was negative. Furthermore, CSF samples were collected and the polymerase chain reaction (PCR) test was performed, but the result was also negative (77). Interestingly, an increased level of ILs, such as IL-16 and IL-8, especially IL-8 was found in 3 patients who illustrated active inflammatory conduction in CSF (77). IL-6 was also found in another case report investigation in Germany by Scheidl et al. (107), which showed the role of IL-6 in multiple organ dysfunction that can lead to death (107,153).
Moreover, there was a patient who showed respiratory symptoms 7 days after the onset of GBS signs in another case report article. Therefore, there could be another explanation that SARS-CoV-2 infection may be nosocomial. However, in that case, its association cannot be ignored, completely (153). Although studies about the association of GBS and COVID-19 are emerging, there are conflicting data in this field. Some studies in 2021 showed no evidence between GBS and COVID-19 (66,104). The extensive epidemiological studies performed in the United Kingdom found no link between GBS and COVID-19. They reported no enhancement in GBS morbidity during the COVID-19 pandemic, because the GBS morbidity fell 40% to 50% between March, April, and May 2020 compared with the previous 3 years. According to some studies, reducing the transmission of other pathogens that triggered GBS during lockdown can be the reason for this evidence. In addition, scientists could not find the similarity between SARS-CoV-2 and human proteins caused by autoimmune diseases, such as GBS, and postvaccine illness may be due to the chance (66).
The mechanism that SARS-CoV-2 virus can trigger GBS is unknown, but multifactors may be involved in this mechanism, including secondary hypoxia, specific receptor damages, and cytokine damages (abnormal immune response) (119). In other words, some mechanisms have been hypothesized (1). First, the PNS is damaged by viruses, such as SARS-CoV-2, entering the nervous system by blood circulation (35). In this regard, a possible mechanism for the coronavirus attack to the olfactory nerve neuroepithelium is hypothesized. It can also immigrate through retrograde axonal transport from the trigeminal and vagal endings (155).
Second, the neurons are damaged by the accumulation of toxic substrates produced under hypoxic conditions in COVID-19 patients with severe pneumonia (5,125). Third, the presence of ACE2 in the nervous system, muscles, and other tissues causes the affinity of this virus to these sites (26,53). On the other hand, it has been assumed that SARS-CoV-2 could directly invade the nerves through ACE2 receptors and lead to peripheral neuropathy (60).
Fourth, the hypothesis described the immune-associated neuropathy. SARS-CoV-2 is supposed to stimulate the production of inflammatory mediators from immune cells, which may result in immune-related polyneuropathy. COVID-19-induced inflammatory milieu also could trigger molecular mimicry, which has a possible role in GBS similar to other immune-mediated diseases (78).
Collectively, testing for COVID-19 is recommended for patients who present the clinical symptoms of GBS to help early diagnosis and treatment, avoid spreading of the virus, and control the disease (1). It was speculated that there is a link between COVID-19 and GBS (82). Most studies are case series and case reports. Therefore, broad epidemiological studies are required to clear that SARS-CoV-2 is causal or coincidental of GBS during this outbreak. Moreover, the occurrence of GBS after vaccination can be possible in the future that needs attention.
Immunomodulatory Approaches for GBS Therapy
During the last decades, therapeutic approaches have progressed from upper and lower massage, soda of phenyl salicylate and strychnine to PE, IVIG, and complement inhibitors (128,138). Prognosis factors, for instance, Erasmus GBS Respiratory Insufficiency Score (EGRIS) helps choose the best treatment by physicians. GBS patients need to be under monitoring every 2 h, especially if they are suffering from AMAN and are in a progressive state due to the poor prognosis, and subsequently heavier treatments (135,138). Based on some reports, 25% of patients experienced intubation (138).
Most meta-analysis investigations indicated a shorter interval between symptom onset and hospitalization, where the possibility of intubation also seems to occur (43,138). On the other hand, intense muscle weakness or bulbar weakness amplifies intubation possibility. Hospitalized patients should be checked permanently in terms of bulbar dysfunction and possible autonomic disturbances. Once the symptoms occur, they should be moved to the ICU. It is important that intubation is not preferred as far as possible. Besides medical treatments, psychological supports and physical treatments are also essential (7,43,138).
GBS has been known as an acute inflammatory disorder of the PNS, which is mediated by autoimmune mechanisms. Therefore, immunomodulatory therapies are considered the main approaches to alleviate its outcomes (72). So far, researchers have evaluated the effect of various methods, including IVIG, PE, complement inhibitors, corticosteroids, and immune adsorption to regulate immune reactions that occur during GBS in the experimental and clinical trial studies that will be described in the following part of the current article and Table 1 (100). It has to be considered that only IVIG and PE are approved and can be recommended for GBS and others are under experimental and clinical studies. During COVID-19 pandemic, IVIG, PE, or both of them have been used as immunomodulatory treatments for GBS and its variants in patients with SARS-CoV-2 infection. However, the combination therapy of IVIG and PE is not notable than each one (106).
Immunomodulation Approaches for Guillain–Barré Syndrome Therapy
APC, antigen-presenting cells; CSF-F, cerebrospinal fluid filtration; CY, cyclophosphamide; GBS, Guillain–Barré syndrome; IVIG, intravenous immunoglobulin; MM, mycophenolate mofetil; PE, plasma exchange; TNF-α, tumor necrosis factor-alpha; TWP, Tripterygium Wilfordii Hook polyglycoside.
Clinical findings have characterized those autoantibodies against gangliosides, especially GM1, GD1a, GD1b, and GT1b that induce nerve injury in GBS cases in different ways. Furthermore, they contribute to poor prognosis and slow down the recovery process (44,148). IVIG is generally the first safe therapeutic procedure for GBS over the world and its efficacy has been established in various investigations. IVIG can bind to the C1, C3b, C4, C3b, C3a, and C5a and neutralize the activated complement; it can neutralize autoantibodies and adjust the production of proinflammatory cytokines through linking to the Fcγ receptor on its expressive cells. Moreover, it prevents the activation and migration of leukocytes (131,145). Studies reported that the injected IVIG has a half-life of about 3 weeks. The recommended dosage for IVIG is 0.4 g kg−1 day−1 for 5 days within 14 days after onset of the first signs of weakness (67,100). Administration of total IVIG dosage usually is divided into 5 days to decline its side effects such as treatment-related fluctuations, especially in children (127).
The results of one cohort study showed that the safety and efficacy of subcutaneous immunoglobulins are equivalent to IVIG and can be administered at home. In addition, it is cost-effective and can decrease the risk of SARS-CoV-2 exposure in health care. Therefore, it can be used as an alternative choice instead of conventional IVIG, but more evaluation is needed (102). IVIG can be used in different fields such as Hematology, Immunology, Nephrology, Dermatology, and Rheumatology in adult respiratory distress syndrome, heart failure, and Alzheimer's disease (97). However, antibody-dependent enhancement, serum sickness, and interfering with effective antibodies produced against viremia are risk factors of IVIG (24). In COVID-19, this method can be used as a prophylactic way to reduce the risk of infection or for treatment of patients, but more studies are needed to evaluate the efficacy (23,25,61,110).
Another available immunotherapy for GBS is PE approach that could be administered 4 weeks after onset of symptoms, five times 50 mL/kg every day (47). This removal therapy has been characterized as an exchange form of plasmapheresis, which cleans the blood plasma of the patient from antibodies, activated components of complements, and immune mediators by replacing it with a donated plasma (99). Studies have shown that PE therapy in GBS patients contributes to accelerate the improvement ratio after the first 6 months to 1 year and decline complications. For example, the recovery of muscle ability in patients treated with PE was likely to be observed after 1 year (47). PE is widely used for many different disorders, such as GBS, myeloma, thrombotic thrombocytopenia, Goodpasture syndrome, hyperviscosity, and blood and kidney disorders, and it is always reported as a safe treatment option. However, there are some disadvantages such as arrhythmias, paresthesia, arterial blood pressure fall, and increased temperature with cold sensation (97).
Overall, despite the number of disadvantages, IVIG and PE are the most common and safe immunotherapeutic methods for the treatment of GBS. In addition, early application of them, before irreversible axonal damage, can prevent neurological complications. Moreover, IVIG and PE efficacy has been proven in various types of studies (144).
The pathological role of activated complement such, as axon damages and destroying myelin, has been established by massive data. Therefore, pharmacological protocols based on complement inhibition could be helpful in controlling GBS (73). Clinical findings have reported the elevated levels of C3a, C5a, and C5–b9 in serum and cerebrospinal fluid of GBS patients, which indicate the aggravated effect of activated complement during the acute phase of the disease (65,84,94). In this regard, some complement inhibitor agents have been examined. Halstead et al. showed that using APT070, an inhibitor of C3 and C5 convertase, significantly led to decreased neuromuscular junction injury in mice that received anti-GQ1b antibodies (48). Concanavalin A (ConA), is the other complement inhibitor that could have an effect on the presynaptic binding of the anti-GQ1b antibody and disturb it (21).
Willison et al. illustrated in their evaluations that rEV576 is a recombinant protein with inhibition capability of C5 to C5a and C5 cleavage as well as MAC formation. It causes neutralization of harmful anti-GQ1b antibodies that fix the complement on presynaptic Schwann cells (49). Another immunomodulatory medication that exerts its effects through inhibition of complement is a type of humanized monoclonal antibody called eculizumab. It also prevents C5 convertase activity. Therefore, it reduces anti-GQ1b antibody and complement-mediated damage at the neuromuscular junction (50,69). Three agents mentioned above have not been established as a specific treatment for GBS, but could be promising immunotherapy to this neurological disease (72).
According to the clinical trials and meta-analyses studies, administration of corticosteroids could downregulate the proinflammatory function of macrophages, but despite their suitable application for the treatment of autoimmune disease, they have no efficacy for GBS. However, when the prolongation of the disease period may cause acute-onset chronic inflammatory demyelinating polyneuropathy (acute-onset chronic inflammatory demyelinating polyneuropathy), corticosteroids could be suggested (130,133). In a GBS patient who received corticosteroids, the results illustrated that they are not effective in the recovery of patients, and also could significantly delay the recovery (54).
Due to the confirmed role of FcγRs in the pathogenesis of GBS by several clinical studies, they might be considered as a therapeutic target for this disease. The polymorphisms in FcγRs genes and their mediated inflammation play a critical part in developing GBS, especially through activated macrophages (112,133). Several studies have been examined the pathological role of FcRn in the experimental/preclinical model of GBS (85,126). According to these studies, the Abdegs (antibodies that enhance IgG degradation) were suggested as a promising candidate for the treatment of GBS. Abdegs showed a beneficial effect to the improvement of antibody-mediated immune neuropathy such as GBS, through binding to the FcRn with high affinity. Therefore, they cause degradation of IgG type of antiganglioside autoantibodies and hasten clearance of them (72,150,151).
Another group of immune-modulating compounds recommended for the treatment of GBS is INF, which are known as inhibitory glycoproteins. Among this family, IFN-β seems to implicate in ameliorating GBS, as its therapeutic effects have been indicated in multiple sclerosis, chronic inflammatory demyelinating polyneuropathy, and EAN (experimental autoimmune neuritis is an animal model of GBS) due to its immunomodulatory properties such as preventing TNF-α secretion and antigen presentation, modulating macrophage activity, decreasing the production of inflammatory cytokines, and T cell proliferation (29,31).
Cyclophosphamide (CY) is another immunomodulatory agent that is expected to be effective in the treatment of GBS. It is helpful in favor of improving the clinical features of GBS in the treatment of EAN models. Nonetheless, its prolonged administration could lead to infection and some neoplastic disorders in the patients (31,145). One of the immunoregulating components that its effect on GBS was evaluated by Garssen et al. is Mycophenolate mofetil (MM). They indicated in their pilot study that MM has an appropriate potential to be an optional therapy of GBS with more efficacy, and it is safer than CY. However, further clinical studies are needed to be done in this regard (42,75).
Rituximab is the monoclonal antibody against CD20, which contributes to the depletion of targeted B cells, so it modulates the function of the immune system. There is no clinical evidence about its effect on the treatment of GBS, but the results from one case report study have been shown that rituximab administration caused the improvement of muscle strength in the patient who developed GBS after undergoing T cell-depleted hematopoietic stem cell transplantation for myelodysplastic syndrome (8,147).
The root extract of Tripterygium wilfordii Hook F is the Chinese medicine that has attracted a wide range of attention for the treatment of inflammatory and autoimmune disease by its immunomodulatory activity such as inhibition of T cell activation, cyclo-oxygenase, and nitric oxide production. Data from a study, which was carried out by Zhang et al., showed that T. Wilfordii polyglycoside (TWP) can be useful for the treatment of GBS patients, probably through reducing the concentrations of IL-6, soluble IL-6 receptor, soluble IL-2 receptor, and the intrathecal IgG synthesis. Besides, some investigations suggested that TWP might ameliorate EAN (57,145,147,152). Some researchers recommended in their study that targeting Th17 to downregulate the proinflammatory-related genes, such as IL-23 and RORγT, can be considered as one of the other therapeutic options in the treatment of GBS/EAN (144).
Recently, using purinergic signaling modulation like P2X7R antagonists as an adjuvant was reported to have anti-inflammatory effects and can decrease the cytokine storm damages. Due to ATP enhancement in neurodegenerative state, such as GBS, the expression of P2X7R (ATP receptor) increases in glial cells resulting in proinflammatory cytokine release. Therefore, inhibition of P2X7R may be helpful for the treatment of inflammatory response reduction in GBS and COVID-19 infection (111). Table 1 illustrates some candidates and new approaches of immunomodulation therapy for GBS.
Conclusion
GBS is a neural disorder that the different parts of the PNS are targeted by the humoral and cellular immune responses. There are different methods to regulate immune reactions during GBS in experimental and clinical trial studies. Since microbial agents are responsible for this disorder, some studies reported GBS cases during the COVID-19 pandemic. However, there may be an association between SARS-CoV-2 and this neuroimmune disorder, but more studies need to be performed to evaluate the effects of SARS-CoV-2 on the PNS and the therapeutic effects of various methods.
Footnotes
Authors' Contributions
Conception and article design: R.J. Collection of data: S.M., N.S., M.T., M.B., S.B., N.M.Z., A.K., and R.J. Article writing: S.M., N.S., M.T., M.B., S.B., N.M.Z., A.K., and R.J. Important revisions made and confirmed final revision: R.J. All authors reviewed and approved the final version of the article.
Author Confirmation Statement
Meidaninikjeh is a PhD student from Alzahra University (Tehran, Iran); Meidaninikjeh and Dr. Khalili are from the Cancer Biomedical Center (CBC) Research Institute (Tehran, Iran); Sabouni is from Mashhad University of Medical Sciences (Mashhad, Iran); Taheri is from Golestan University of Medical Sciences (Gorgan, Iran); Borjkhani is from the National Institute of Genetic Engineering and Biotechnology (Tehran, Iran); Bengar is from Islamic Azad University – Shahre Ghods Branch (Tehran, Iran); and Dr. Zolbanin and Dr. Jafari are from Urmia University of Medical Sciences (Urmia, Iran), all where education and research are the primary functions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.