
Abstract
The purpose of this research was to investigate the gene expression levels of inflammatory cytokines interferon (IFN)γ, tumor necrosis factor (TNF)α, interleukin (IL)1β, IL2, IL6, IL8, and IL17, and anti-inflammatory cytokines IL4, IL10, IFNα, and IFNβ, as well as relevant key transcription factors (TFs), including GATA3, PU1, NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells), IRF3 (interferon regulatory factor 3), BCL6 (B cell lymphoma 6 protein), FOXP3 (forkhead box P3), RORγt, and T-bet (T-box expressed in T cell) in Iranian patients with moderate and severe coronavirus disease 2019 (COVID-19). Fifty-six patients with COVID-19, and 25 healthy controls (HCs) age and sex matched were investigated. Based on the interim guidance of COVID-19 from the World Health Organization, the patients were classified into 33 moderate and 23 severe patients with COVID-19. The gene expression levels of cytokines and relevant TFs were quantified in peripheral blood mononuclear cells by quantitative real-time polymerase chain reaction (qRT-PCR). The gene expression levels of TFs RoRγ (RAR-related orphan nuclear receptor γ), NF-κB, and T-bet were significantly higher in patients with COVID-19 compared with HCs. Furthermore, the gene expression levels of cytokines, including IL2, IFNγ, IL6, TNFα, IL1β, IL8, and IL17, were significantly higher in patients with COVID-19 than HCs. However, there was a significant increase for IL6, TNFα, and IL17 in severe compared with moderate patients with COVID-19. Finally, The Spearman correlation analysis revealed a significantly positive correlation for IL6 and TNFα, IL6 and IL2, IL6, IFNγ, and IL2 and IFNγ. These data suggest that expression of IL6, TNFα, and IL17 as well as the synergic effect of elevated values of IL2 and IFNγ should be considered in the treatment and management of patients with severe COVID-19.
Introduction
The current pandemic of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has affected all aspects of our daily lives, including lifestyle as well economic, political, and international affairs. Based on the COVID-19 dashboard of the World Health Organization (WHO), as of February 20, 2022, the SARS-CoV-2 had infected more than 420 million people worldwide (confirmed by tests) and resulted in more than 6 million deaths. Despite the start of the vaccination program with different types of vaccines, to date, many new cases of COVID-19 infection with different types of COVID-19 with different variants have been reported worldwide (World Health Organization, 2022). Also, due to the huge demands as well as the conditions of some countries, the implementation of the national immunization program may take more than a few months.
In addition, with several mutations observed in the genome of the virus and the different efficacy of the vaccines, it seems that we will meet new cases of COVID-19 for a longer period of time (Forni and Mantovani, 2021; Mills and Salisbury, 2021; Wouters et al, 2021). Consequently, understanding the pathophysiology of COVID-19 disease is still essential and effective to treat patients with COVID-19.
Numerous studies have shown that one of the most important causes of mortality in patients with COVID-19 is the unrestrained production of inflammatory cytokines due to increased cellular immune responses, also known as cytokine storms (Del Valle et al, 2020; Han et al, 2020; Long et al, 2020). Studies of different countries have assessed the expression levels of some cytokines and reported elevated serum levels of tumor necrosis factor (TNF)α, interleukin (IL)6, IL1β, and interferon (IFN)γ in severe and critical patients with COVID-19 (Del Valle et al, 2020; Han et al, 2020; Long et al, 2020; Meftahi et al, 2020; Parisi and Leosco, 2020). However, few studies investigated the gene expression levels of an almost complete panel of cytokines and their relevant transcriptional factors in peripheral blood mononuclear cells (PBMCs) of patients with COVID-19.
Therefore, the purpose of this research is to investigate the gene expression levels of inflammatory and anti-inflammatory cytokines and relevant transcription factors (TFs) in Iranian patients with moderate and severe COVID-19 to evaluate the discrepancies between them. Also, the possible correlations of them are analyzed to associate with cytokine storms of COVID-19.
Materials and Methods
Selection of patients
In this study, we investigated 56 patients with COVID-19 (mean age: 61.8 ± 18.9 years, range 22-93 years), including 24 female (42.9%) and 32 male (57.1%), compared with 25 healthy individuals age and sex matched (mean age: 61.48 ± 18.7 years, range 22–90 years). The participants were recruited from April 2020 to May 2020 in the infectious department of Rasoul-e-Akram and Firoozabadi Hospitals, which are two referral COVID-19 centers in Tehran, Iran. The COVID-19 diagnosis was based on a real-time polymerase chain reaction (PCR) assay of both RdRp (RNA-dependent RNA polymerase) and N (nucleocapsid) genes of SARS-CoV-2 in nasopharyngeal swab samples (Pishtaz Teb, Tehran, Iran). Patients with diabetes, hypertension, cardiovascular disease, body mass index >25, autoimmune diseases, and a history of other underlying diseases were not included in our study. In addition, all patients were sampled before starting treatment, especially anti-inflammatory and immunosuppressive therapies.
According to the clinical signs of pneumonia and oxygen saturation (measured by pulse oximetry in the room air) from interim guidance on the management of COVID-19 from the WHO patients with COVID-19, patients were classified as moderate (equal or more than 90% oxygen saturation) and severe (oxygen saturation less than 90% with severe respiratory distress). As mentioned, patients with COVID-19 were classified into 33 (58.9%) moderate patients (mean age: 57.9 ± 17.9 years) and 23 (41.1%) severe patients (mean age: 66.9 ± 19.3 years) during the early phase of infection (less than 10 days after symptom onset). We included 25 healthy individuals with negative SARS-CoV-2 real-time polymerase chain reaction and IgG antibody tests as the healthy controls (HCs) group. This study is approved by the Medical Ethics Committee (
PBMC isolation and total RNA extraction
Five milliliters of peripheral blood from each subject were collected in K3-EDTA tubes. Fresh PBMCs were isolated from whole blood by density gradient centrifugation using Ficoll (Sigma Aldrich). To deplete platelets, cold phosphate-buffered saline (pH = 7.4) was added to PBMCs; samples were centrifuged at 200 g for 10 min at 4°C. Total RNA was extracted from ∼2 × 106 PBMCs using 750 μL of QIAzol reagent (Qiagen) following the manufacturer's instructions. Briefly, the cell lysate was mixed with 200 μL of chloroform and centrifuged at 12,000 g for 15 min at 4°C.
The upper, colorless fluid phase was aspirated and mixed with 600 μL of isopropanol and centrifuged at 12,000 g for 10 min at 4°C. The RNA pellets were washed with 1 mL of 70% ethanol, centrifuged at 7,500 g for 6 min at 4°C, then, air dried, and dissolved in nuclease-free distilled water. The concentration and purity of extracted RNA were analyzed by measuring absorbance at 260/280 nm using a NanoDrop spectrophotometer (ND1000 Technologies, Wilmington, DE). The samples were stored at −80°C.
Complementary DNA synthesis and mRNA quantification
Complementary DNAs (cDNAs) were synthesized from the extracted RNAs by Oligo dT and random hexamers using an Easy cDNA synthesis kit (PARSTOUS, Tehran, Iran) based on the manufacturer's protocol. mRNAs were quantified in duplicate reactions using a Rotor-gene Q thermal cycler (Qiagen, Germany). Reactions were carried out in 20 μL total volumes, including 10 μL of SYBR Green PCR Master Mix (Amplicon, Denmark), 0.5 μL of both forward and reverse primer, 1 μL of undiluted cDNA, and 8 μL of nuclease-free water (CinnaGen, Tehran, Iran). The β-actin and GAPDH genes were used as internal controls for normalization. The relative expression levels of cytokines (IFNα, IFNβ, IFNγ, TNFα, IL1β, IL2, IL4, IL6, IL10, and IL17) and TFs (BCL6, FoxP3, IRF3, GATA3, NF-κB, PU.1, Rorγt, and T-bet) were calculated using the 2−ΔΔCt method. The primer pairs, which were used for the quantification of each gene, are shown in Table 1.
The Forward and Reverse of Primer Sequences
BCL6, B cell lymphoma 6 protein; FoxP3, forkhead box P3; IFN, interferon; IL, interleukin; IRF3, interferon regulatory factor 3; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; Rorγt, RAR-related orphan nuclear receptor γ t; T-bet, T-box expressed in T cell; TNFα, tumor necrosis factor alpha.
Statistical analysis
SPSS (version 24) and GraphPad Prism (version 8.01) software were used for the statistical analysis and data presentation in figures, respectively. The D'Agostino-Pearson test was used to analyze the normality of data distribution. Non-normally distributed variables were analyzed using the Mann–Whitney and Kruskal–Wallis test, and normally distributed variables using the T-test and one-way ANOVA (analysis of variance).
For all comparisons, multiple comparisons test with the Bonferroni method was used between the studied groups. The Spearman correlation was used to investigate the possible associations among gene expression levels. The diagnostic accuracies of severe and moderate COVID-19 were analyzed by receiver operating characteristic (ROC) and the area under the curve (AUC). Univariate and multivariate logistic regression were performed to identify predictors associated with severe patients with COVID-19. (Each cytokine showed statistically significant difference from the univariate analysis, and these were next analyzed by multivariate logistic regression by the Enter model.) Results were considered statistically significant at a p-value less than 0.05.
Results
In this study, 56 patients with COVID-19 in the moderate (n = 33, mean age: 57.9 ± 17.9 years) and the severe (n = 23, mean age: 66.9 ± 19.3 years) groups were compared with 25 healthy individuals as the HC group. Demographic and laboratory findings of COVID-19 and HCs were shown in Table 2. Gene expression levels of cytokines and relevant TFs were evaluated in the PBMCs of moderate and severe patients with COVID-19 compared with HCs. The gene expression levels of RoRγ (RAR-related orphan nuclear receptor γ) (Fold Change [FC]: 2.06, p = 0.002), NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) (FC: 2.1, p = 0.003), and T-bet (FC: 1.82, p = 0.02) were significantly higher in patients with COVID-19 compared with HCs.
The Laboratory Finding of Coronavirus Disease 2019 and Healthy Control Groups in This Study
ns, Nonsignificant, * p < 0.05, ** p < 0.01, *** p < 0.001.
ALT, alanine transaminase; AST, aspartate transaminase; COVID-19, coronavirus disease 2019; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; PT, prothrombin time.
However, there was no significant difference between moderate and severe patients with COVID-19. Furthermore, gene expression levels of PU1, Bcl6 (B cell lymphoma 6 protein), and GATA3 did not show a significant difference between patients with COVID-19 and HCs. Although there was no significant difference in the IRF3 (interferon regulatory factor 3) and FOXP3 (forkhead box P3) levels in patients with COVID-19 compared with HCs, there was a significant increment of them in severe patients compared with moderate patients with COVID-19 (Fig. 1).
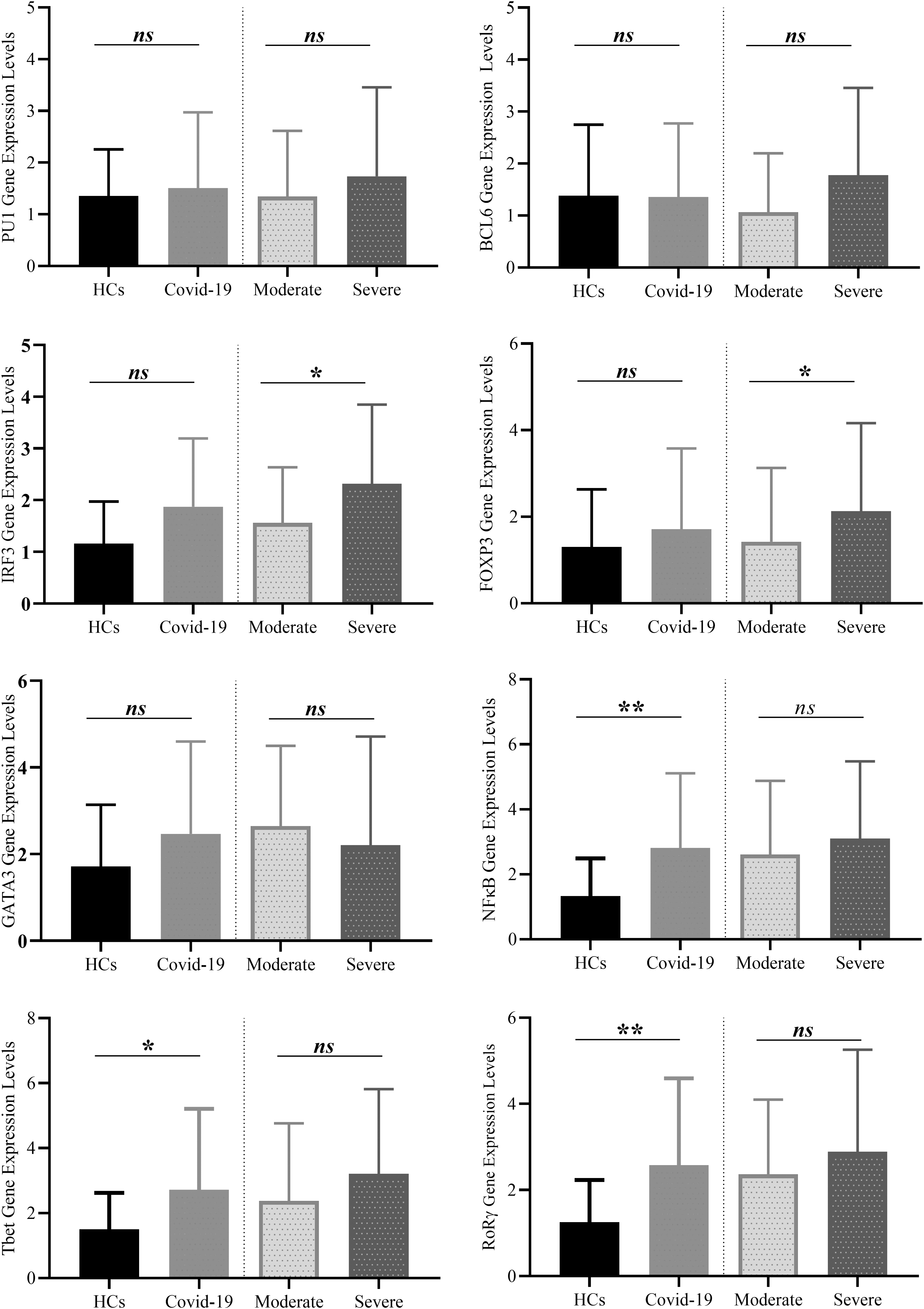
The gene expression levels of TFs in patients and HCs. The levels of RoRγ, NF-κB, and T-bet were significantly higher in the patients with COVID-19 compared with HCs. However, there was no significant difference between moderate and severe patients with COVID-19 for these TFs. The gene expression levels of PU1, Bcl6, and GATA3 did not show a significant difference between patients with COVID-19 and HCs. Although there was no significant difference in the IRF3 and FOXP3 levels in patients with COVID-19 compared HCs, there was a significant increment of them in the severe patients compared with moderate patients with COVID-19. *p < 0.05, **p < 0.01. Bcl6, B cell lymphoma 6 protein; COVID-19, coronavirus disease 2019; FOXP3, forkhead box P3; HC, healthy control; IRF3, interferon regulatory factor 3; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; RoRγ, RAR-related orphan nuclear receptor γ; TF, transcription factor.
The gene expression levels of IL2 (FC: 3.15, p < 0.001), IFNγ (FC: 2.32, p < 0.001), IL6 (FC: 8.53, p < 0.001), TNFα (FC: 2.04, p = 0.018), IL1β (FC: 2.1, p = 0.001), IL8 (FC: 1.96, p = 0.002), IFNα (FC:2.3, p < 0.01), IFNβ (FC:2.0, p < 0.05), and IL17 (formally IL17A) (FC: 1.84, p = 0.04) were significantly higher in patients with COVID-19 than HCs. However, there was significant increase for IL6 (FC: 2.47, p = 0.005), TNFα (FC: 1.88, p = 0.019), and IL17 (FC: 2.04, p = 0.005) in severe compared with moderate patients with COVID-19 (Fig. 2).

The gene expression levels of cytokines in patients and HCs. The gene levels of cytokines, including IL2, IFNγ, IL6, TNFα, IL1β, IL8, and IL17, were significantly higher in patients with COVID-19 than HCs. However, there was significant increase for IL6 (FC: 2.47, p = 0.005), TNFα (FC: 1.88, p = 0.019), and IL17 (FC: 2.04, p = 0.005) in severe compared with moderate patients with COVID-19. *p < 0.05, **p < 0.01, ***p < 0.001. FC, Fold Change; IFN, interferon; IL, interleukin; TNFα, tumor necrosis factor alpha.
ROC curve analysis showed the gene expression levels of IL6 (AUC = 0.75, p = 0.002) and IL17 (AUC = 0.72, p = 0.006) could differentiate moderate from severe patients with COVID-19. However, the other cytokines and TFs did not show significant AUC for severe discrimination of severe patients with COVID-19 (Fig. 3).

The ROC curve analyses. The comparison of cytokines differentiating severe versus (n = 23) moderate (n = 33) patients with COVID-19. The AUCs (95% CI) and p-values of cytokines that significantly increase in the severe group compared with the moderate group of patients with COVID-19 were analyzed. 95% CI, 95% confidence interval; AUC, area under the curve; ROC, receiver operating characteristics.
The Spearman correlation analyses revealed significantly positive correlation between IL6 and TNFα (r = 0.39, p < 0.001), IL6 and IL2 (r = 0.31, p < 0.05), IL6 and IFNγ (r = 0.35, p < 0.01), and IL2 and IFNγ (r = 0.33, p < 0.01). Interestingly, there was a weak positive correlation between IL6 and FOXP3 (r = 0.26, p < 0.05). The gene expression correlations among cytokine and TFs are shown as a heat map in Figure 4. The cytokine and TF levels as predictors for severe COVID-19 were assessed by univariate and multivariate logistic regression. In the univariate analysis, the gene expression levels of IL6, IL17, IL10, and TNFα were significant severe predictors. However, in the multivariate analysis, only IL6 and IL10 were significant severe predictors (Table 3).
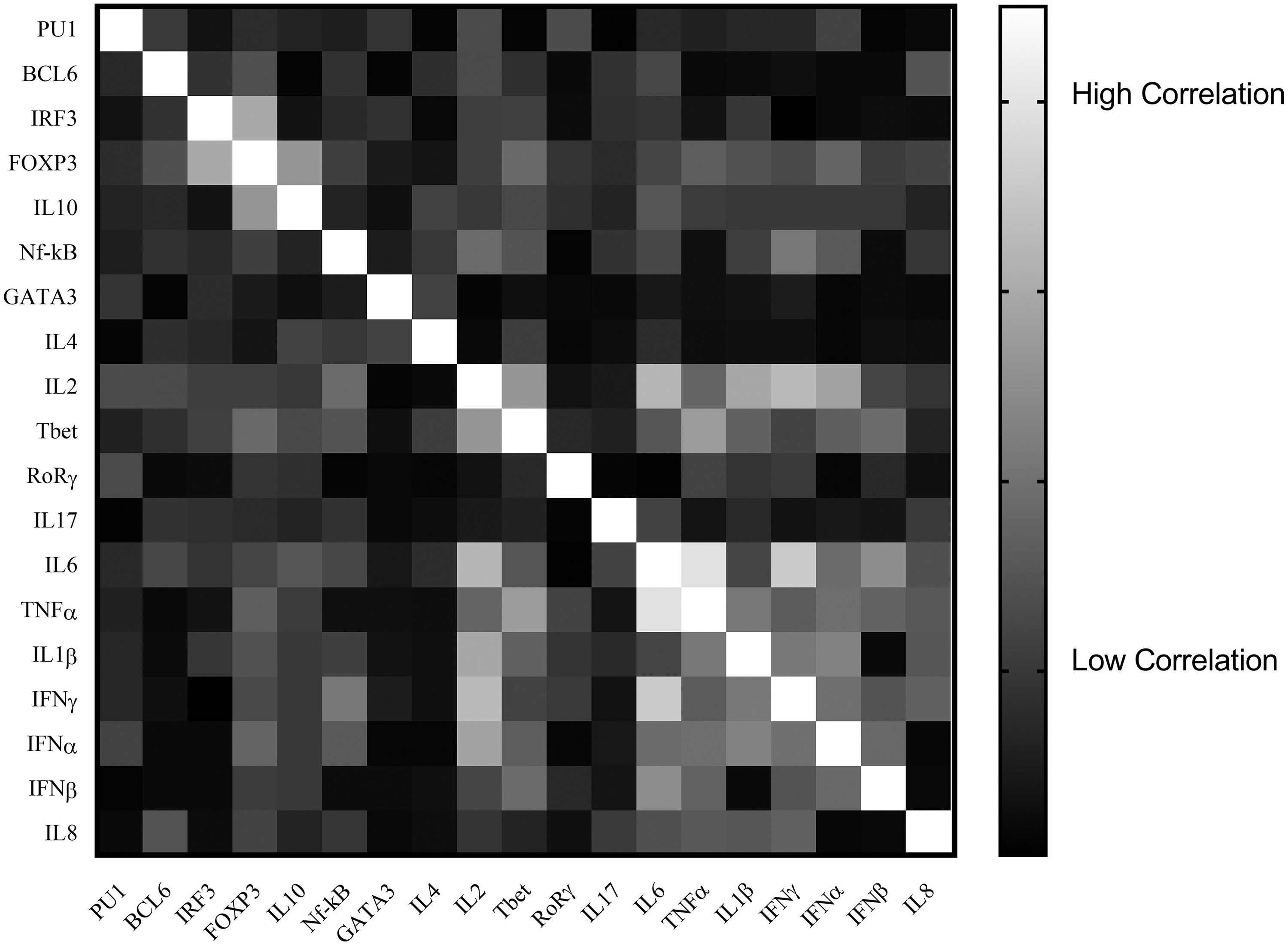
The heat map depicts Spearman correlation analyses between cytokines and TFs. The analyses revealed significantly positive correlation for IL6 and TNFα (r = 0.39, p < 0.001), IL6 and IL2 (r = 0.31, p < 0.05), IL6 and IFNγ (r = 0.35, p < 0.01), and IL2 and IFNγ (r = 0.33, p < 0.01). Interestingly, there was a weak positive correlation for IL6 and FOXP3 (r = 0.26, p < 0.05).
Univariate and Multivariate Logistic Regression Analysis of Gene Expression of Cytokines to Predict Severe from Moderate Patients with Coronavirus Disease 2019
The significance values (< 0.05) are shown in bold.
95% CI, 95% confidence interval.
Discussion
There are numerous reports on the investigation of serum cytokine levels in patients with COVID-19. However, few studies are available on the dysregulation of gene expression of cytokines and their associated TFs in the PBMCs of patients with COVID-19 (Gardinassi et al, 2020; Sadanandam et al, 2020). In this study, a wide range of inflammatory and anti-inflammatory cytokines and their associated TFs were evaluated by quantitative real-time polymerase chain reaction in moderate and severe Iranian patients with COVID-19 compared with the HCs. Besides, their role and correlation with each other in the formation of cytokine storms were investigated.
The results of this study showed that the levels of IFNγ, T-bet (T-box expressed in T cell), and IL2 in patients with COVID-19 were higher than HCs. However, this difference was not observed in the severe compared with moderate patients with COVID-19. Conflicting results have been reported regarding the association between serum level of IL2 and the severity of COVID-19. Tjan et al (2021) showed that IL2 serum levels were higher in asymptomatic and mild patients than moderate and severe patients, while Long et al (2020) showed that serum levels of IL2 were directly correlated with the disease severity. In our study, gene expression levels of IL2 and IFNγ were positively correlated with IL6 and TNF in COVID-19 patients.
Recently, reports emphasized that the increased gene expression of IL2 and IFNγ in lymphocytes could be syngeneic effects for systemic overexpression of IL6 and TNFα, resulting in cytokine storms in severe and critical patients with COVID-19 (Qin et al, 2022; Hu et al, 2021; Kim et al, 2021; Mangalmurti and Hunter, 2020). The most elevation of cytokine levels was observed for IL6 (FC: 2.47) and TNF-α (FC:1.88) in severe COVID-19 patients compared with moderate patients. Furthermore, the IL6 expression levels showed a positive correlation with TNFα, IL2, IFNγ, and FOXP3.
Although the levels of other inflammatory cytokines, including IL1β and IL8, were higher in patients with COVID-19, this increase was not observed in severe patients with COVID-19. Consistent with our results, Del Valle et al (2020) showed the serum levels of TNFα and IL6 were associated with disease severity and other inflammatory parameters. They reported elevated serum levels of TNFα, IL6, and IL8 were the most important cytokines in the production of cytokine storms (Del Valle et al, 2020). However, the results of this study support the overexpression of IL6, TNFα, IL2, and IFNγ in severe COVID-19 conditions.
Although the levels of other inflammatory cytokines, including IL1β and IL8, were higher in patients with COVID-19, this increase was not observed in severe patients with COVID-19. Similar to the pattern of IL8 and IL1β expression levels, the values of IFNα and IFNβ showed an increase in patients with COVID-19 compared with HCs, but this increase was not seen in severe disease conditions. Besides, the expression levels of IFNα and IFNβ did not show a significant correlation with inflammatory cytokines, including IL1β, IL2, IL6, IFNγ, and TNFα.
The gene expression levels of IL10 as an anti-inflammatory cytokine were increased in severe patients compared with moderate patients. The results of multivariate logistic regression showed that the simultaneous increase of IL6 and IL10 was a significant indicator for predicting severe patients versus moderate patients with COVID-19 (odds ratio [OR] = 1.6). Han et al (2020) reported that serum levels of IL6 and IL10 were higher in critical and severe than mild and moderate patients with COVID-19 so that these cytokines could be applied as a biomarker to predict disease severity. However, our results showed no significant correlation between IL10 and inflammatory cytokines, especially TNFα and IL6 levels in patients with severe COVID-19. It seems that in severe COVID-19 patients with elevated levels of IL6 and TNF, the values of IL10 did not increase considerably.
Although an increase in GATA3 and IL4 gene expression was seen in patients with COVID-19, this increase was not significant. Some studies showed an increase in serum levels of IL4 in the patients with COVID-19 compared HCs; this increment was not observed in moderate and severe conditions (Han et al, 2020). The TF NF-κB showed a significant increase in patients with COVID-19 compared with HCs. However, this difference was not seen in moderate and severe patients. In several studies, the NF-κB pathway is mentioned as one of the most important for controlling cytokine storms in critical patients (Kandasamy, 2021; RECOVERY Collaborative Group et al, 2021; Kircheis et al, 2020; Seif et al, 2020; Liu et al, 2017).
Interestingly, the expression levels of IL17 and RoRγ were higher in patients with COVID-19, especially severe ones. However, this increase did not show a significant correlation with the increase of other inflammatory cytokines such as TNFα, IL6, and IL1β. The results of the ROC curve analysis and univariate logistic regression in our study showed that, in addition to IL6 expression, increasing IL17 expression could also predict severe COVID-19 patients compared to moderate ones (AUC = 0.72, OR = 1.33). Rare studies have reported elevated levels of IL17 in severe COVID-19 patients (Bulat et al, 2021; Balestri et al, 2020; Pacha et al, 2020; Ricardo and Lipner, 2020; Wu and Yang, 2020).
Few studies are available on the various levels of IRF3, PU1, and BCL6 TFs in the PBMCs of patients with COVID-19. In vivo and ex vivo studies have shown that strong immune responses of IFN are not induced after exposure to the MERS and the SARS-CoV family. Salman et al showed that, despite the production of IFNα, the IFNβ responses were not strongly generated after exposure to the mentioned viruses, especially SARS-Cov-2, which is related to the incomplete activation of IRF3 (Salman et al, 2021), although the results of our study showed that IRF3 levels increased in severe patients with COVID-1, which did not result in an increase in the expression levels of IFNα and IFNβ.
Recently, several studies have shown that IL15 has increased significantly in people with a critical condition of the disease, who have died. It seems that due to the complex pathophysiology of the disease and the systematic destructive effects of the production of inflammatory different cytokines, supplemental studies are needed to determine the exact reasons for the development of widespread inflammatory responses, especially in patients with severe and critical conditions of COVID-19.
Conclusion
The results indicated that expression of TFs, including RoRγ, NF-κB, and T-bet, and cytokines, including IL2, IL6, IFNγ, IL1β, IL8, IL17, IFNα, and IFNβ, significantly increased in patients with COVID-19 compared with HCs. If the results of this study are confirmed by the evaluation of their protein products, they suggest that should be considered in the treatment and management of patients with COVID-19. Also, the gene expression levels of IL6, TNFα, IL17, IL10, IRF3, and FOXP3 were significantly higher in patients with severe COVID-19. The data suggest that these cytokines and TFs could be used as predictive factors for disease severity in patients with COVID-19.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the staff of Immunology and infectious diseases institute Rasoul-e-Akram and Firoozabadi hospitals.
Authors' Contributions
All authors are from the Iran University of Medical Sciences (Tehran, Iran), where education and research are the primary functions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study has been supported by Immunology Research Center of Iran University of Medical Sciences (Grant No. #9850-17563).