
Abstract
Hantaan orthohantavirus (HTNV) can cause hemorrhagic fever with renal syndrome (HFRS) characterized by acute kidney injury and hemorrhage. Neutrophils are the most abundant innate immune cell and the body's first line of defense against pathogens. Currently, an increasing number of studies have shown that neutrophils may be a mixed blessing in terms of viral infections. However, the role of neutrophils in HFRS patients with HTNV infection has not been fully declared. In this study, we analyzed plasma levels of both myeloperoxidase (MPO) and MPO-DNA in HFRS patients, together with the clinical parameters. Neutrophil-platelet aggregates (NPAs) during the acute and convalescent phases of HFRS were also assessed. The results showed that plasma MPO-DNA levels had no change in different disease phases or severities of HFRS patients. Whereas plasma MPO significantly increased in the acute phase and critical/severe groups of HFRS patients. Furthermore, plasma MPO was positively correlated with inflammatory clinical parameters, such as white blood cell counts, neutrophil counts, and renal injury-related parameters, such as blood urea nitrogen, blood uric acid, and serum creatinine, as well as negatively correlated with and platelet counts. In addition, NPAs increased both in acute and convalescent phase in HFRS patients compared with normal controls. These results suggested that elevated plasma MPO in HFRS patients correlated with disease severity, together with the increases of NPAs in HFRS patients, which may provide new insights into potential role of neutrophils in the pathogenesis of HFRS.
Introduction
Hantaan orthohantavirus (HTNV), an enveloped single-stranded RNA virus, belongs to the class Bunyavirales, order Hantaviridae (HTV), and can cause severe lethal hemorrhagic fever with renal syndrome (HFRS) in humans (Ali et al., 2009). The latest data from the World Health Organization show that ∼200,000 cases of HFRS occur each year worldwide, with a mortality rate ranging from <1% to >10%, and almost 90% of cases occur in China (Bai et al., 2019). People with HFRS are clinically characterized by sudden fever, hemorrhage, thrombocytopenia, and acute renal failure (Jiang et al., 2016). Although both innate and adaptive immune mechanisms contribute to hantavirus-associated disease, including immune complexes, complement activation, B cell response, T cell response, and HTNV-induced cytokine production, have been widely recognized (Hayasaka et al., 2007; Jokinen et al., 1978; Mittler et al., 2019; Muranyi et al., 2005; Penttinen et al., 1981), the pathogenesis of HFRS is far from completely understood.
Neutrophils are important components of the innate immune system that mediate pathogen defense by multiple processes (Liew and Kubes, 2019). Once neutrophils reach the site of infection their primary role is to kill invading microbes by producing reactive oxygen species and releasing antimicrobial proteins, such as myeloperoxidase (MPO) and neutrophil elastase (NE) in a process of degranulation (Odobasic et al., 2016; Pham, 2006). In addition, neutrophils also release neutrophil extracellular traps (NETs), a fibrillary network composed of a double-stranded DNA (dsDNA) backbone and coated with histones and granule molecules, such as MPO, NE, and histone, with the functions of entrapping and killing pathogens (Brinkmann et al., 2004; Yipp and Kubes, 2013); therefore, MPO-DNA is considered to be probably the most specific method for detecting NETosis at present (Metzler et al., 2011; Papayannopoulos et al., 2010).
Moreover, neutrophils interact with platelets and form neutrophil-platelet aggregates (NPAs), which is a noteworthy mechanism of innate immunity that prevents the dissemination of infectious agents (Koupenova et al., 2019). Studies have also shown that in sterile inflammation, platelets induce injury to endothelial cells and initiate neutrophil crowing to the site and are involved in the tissue repair without NET formation (Slaba et al., 2015).
An increasing number of studies have shown that neutrophils may be a mixed blessing in terms of viral infections. A large number of neutrophils were found infiltrating the airways of infants with respiratory syncytial virus infection, and these neutrophils may clear the virus by releasing particles, such as NE, MPO, and gelatinase, but they also lead to neutrophil degranulation, which causes damage to the airway epithelium and mucocilia (Deng et al., 2020). Significantly increasing neutrophils in COVID-19 patients cause an excessive inflammatory response in the body through NETs, exacerbating damage to the nuclear epithelial cells of lung endothelial cells and leading to the development of severe pneumonia (Borges et al., 2020; Zuo et al., 2020).
Laboratory findings during acute stage of HFRS in HTNV-infected patients are anemia, leukocytosis, thrombocytopenia, elevated serum creatinine (Cr), as well as proteinuria and hematuria (Jiang et al., 2016). Studies have also shown that plasma MPO and peripheral blood neutrophil levels are significantly increased in patients infected with Puumala virus (PUUV), and the virus may recruit and activate neutrophils by binding to β2 integrins on neutrophils (Schönrich et al., 2015; Strandin et al., 2018). However, the dynamic changes in MPO and MPO-DNA during HTNV infection and their relationships with clinical markers have not been fully determined.
In this study, plasma MPO-DNA and MPO levels and NPAs in HFRS patients with different severities and phases after HTNV infection were assessed. Furthermore, the correlation between plasma MPO levels and HFRS clinical parameters was analyzed. This analysis might provide new insight of neutrophils in the pathogenesis of HFRS.
Materials and Methods
Patients and sample preparation
We examined MPO-DNA levels in a total of 97 plasma samples from 48 HFRS patients and 9 healthy donors (normal controls [NCs]) from the Second Affiliated Hospital of Air Force Medical University (Xi'an, China) and Xi'an Eighth People's Hospital in 2020. Among them, 79 plasma samples from 45 patients were tested for MPO levels and 31 patients with paired samples of acute and convalescent phases were also tested for MPO tendency. In addition, 19 samples of acute phase and 20 samples of convalescent phase were evaluated for NPAs and 9 patients with paired samples of acute and convalescent phases were analyzed for NPAs tendency. All patients were diagnosed by serological monitoring of Hantaan virus-specific immunoglobulin M and immunoglobulin G. Blood samples were obtained by centrifugation after treatment with the anticoagulant ethylenediamine tetraacetic acid (EDTA) and stored frozen at −80°C before the start of the experiment. The characteristics of all patients are summarized in Table 1.
Characteristics of Hemorrhagic Fever with Renal Syndrome Patients Enrolled in This Study
According to the latest expert consensus on the prevention and treatment of HFRS in China, HFRS patients can be divided into mild, moderate, severe, and critical types according to the severity of the disease as previously described (Jiang et al., 2016). The typical course of HFRS patients can be divided into five phases: febrile, hypotensive, oliguric, diuretic, and convalescent phases (Noh et al., 2019). Based on the classically defined five stages of HFRS, we classified the HFRS patients in this study into acute phase (including febrile, hypotensive, and oliguric phases) and convalescent phase (including diuretic and convalescent phases) (Jonsson et al., 2010; Zhang et al., 2015). Patients with other renal diseases, diabetes, hematological diseases, cardiovascular diseases, autoimmune diseases, viral hepatitis, and other inflammatory diseases were excluded from this study.
This study was approved by the Review Board of the Air Force Military Medical University (KY20173178-1), and all enrolled subjects were informed before blood sample collection.
Quantification of MPO-DNA complexes
MPO-DNA complexes were quantified similarly to what has been previously described, with some modifications (Veras et al., 2020). A precoated anti-human MPO antibody microplate from the Human Myeloperoxidase ELISA Kit (ab119605; Abcam) was used to capture MPO in plasma. Then, Quant-iT PicoGreen dsDNA reagent and kits (P11496; Thermo) were used to quantitatively detect the DNA content in the MPO-DNA complex in the plasma samples according to the instructions with standard curve from 1 to 250 ng/mL.
Enzyme-linked immunosorbent assay for the detection of plasma MPO
Plasma MPO was quantified in the 1:100 diluted samples using the Human Myeloperoxidase ELISA Kit (ab119605; Abcam) according to the instructions with a detection range of 312–20,000 pg/mL.
Determination of NPAs by flow cytometry
The determination of NPAs was performed on whole blood samples from HFRS patients and normal donors. In brief, 1 mL of venous blood coagulated by EDTA was stained with 5 μL of anti-human CD41-PE (MA1-19648; Invitrogen) for 15 min at room temperature. At the end of the incubation, 2 mL FACS lysing solution (349202; Becton Dickinson) diluted 1:10 in distilled water was added and incubated for 10 min at room temperature. Matched isotype controls were used as negative controls. The neutrophils were gated based on their forwards and side scatter characteristics. The data were analyzed using 10,000 cells and were computed and analyzed using FlowJo 7.6.1 software (Oregon).
Clinical data collection and analysis
The values of clinical parameters, including white blood cell (WBC) counts, neutrophil counts, platelet (PLT) counts, blood urea nitrogen (BUN) level, blood uric acid (UA) level, and Cr level, were recorded on the same day with plasma collection for MPO detection during each patient's hospitalization. Correlation analysis was performed using clinical parameters and MPO levels obtained in samples from different disease courses of the same patient. The clinical parameters of all patients participating in the trial are shown in Table 2.
Clinical Indicators of Hemorrhagic Fever with Renal Syndrome Patients Enrolled in Correlation Analysis between Myeloperoxidase and Clinical Parameters
Values represent medians with ranges (minimum and maximum values).
Statistical analysis
The statistical analysis was performed in GraphPad Prism 6 software. The Kruskal–Wallis test was used for plasma MPO-DNA and MPO comparisons between different groups. One-way analysis of variance was used for NPAs comparisons between different groups. Continuous variables are presented as the median and its range (minimum and maximum). Correlation analysis between plasma MPO levels and clinical parameters was performed using the Spearman correlation test. p < 0.05 were considered statistically significant.
Results
Plasma MPO-DNA levels in HFRS patients
To determine whether NETs formation involved in HFRS pathogenesis, we measured the circulating NETs, in the form of MPO-DNA complexes, and the comparison of MPO-DNA levels in different disease severities and phases with that in NCs were analyzed. The results showed that there was no significant difference of plasma MPO-DNA levels in critical/severe groups, moderate/mild groups of HFRS patients and NCs (p > 0.05; Fig. 1A). Furthermore, there was also no significant difference of plasma MPO-DNA levels among acute phase, convalescent phases of HFRS patients and normal subjects (p > 0.05; Fig. 1B). These results suggested that NETs formation was not responsible for the neutrophil pathogenesis in HFRS.
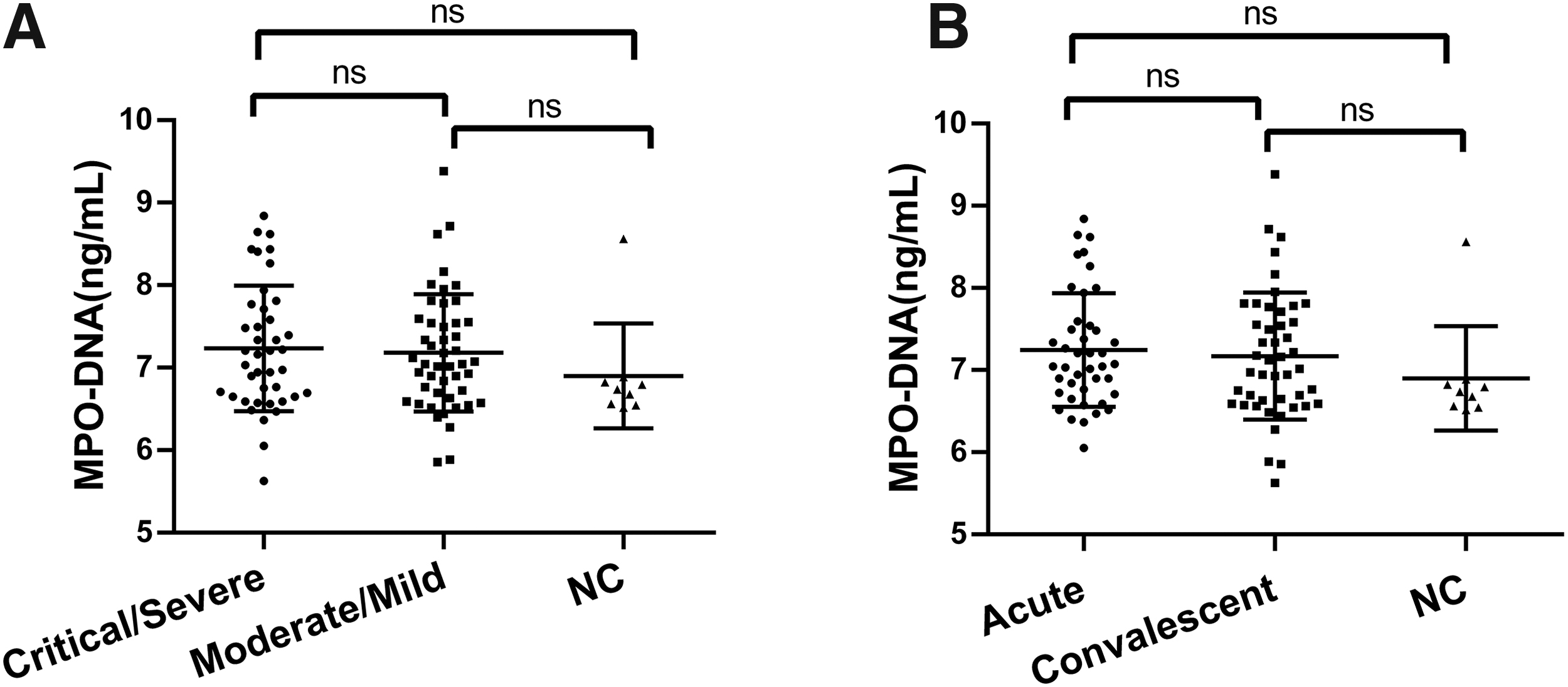
Dynamic changes in plasma MPO-DNA levels in HFRS patients.
Elevated plasma MPO in HFRS patients
Next, we questioned whether plasma MPO levels were related to the severities and courses of the disease. We found that plasma levels of MPO from HFRS patients in the critical/severe group were higher than the moderate/mild group [443.95 (111.00–867.30) ng/mL vs. 320.40 (14.60–757.9.90) ng/mL, p = 0.0384] and much higher than the NCs [443.95 (111.00–867.30) ng/mL vs. 103.60 (63.40–185.50) ng/mL, p = 0.0002]. The plasma MPO levels in the moderate/mild group were also higher than the NCs [320.40 (14.60–757.9.90) ng/mL vs. 103.60 (63.40–185.50) ng/mL, p = 0.0320] (Fig. 2A).

Dynamic changes in plasma MPO levels in HFRS patients.
The plasma MPO level in HFRS patients during the acute phase was significantly higher than that in NCs [461.15 (188.40–867.30) ng/mL vs. 103.60 (63.40–185.50) ng/mL, p < 0.0001] and convalescent phase [197.20 (14.60–673.90) ng/mL, p < 0.0001]; however, plasma MPO level in convalescent phase of HFRS patients were not significantly different from that in NCs (p > 0.05; Fig. 2B). In addition, MPO in paired plasma samples in acute phase and convalescent phase from 31 patients showed the declining tendency except for 2 patients with opposite tendency or no obvious change (Fig. 2C).
Correlation between plasma MPO levels and inflammatory parameters in HFRS patients
To determine the increase of plasma MPO levels was related to the inflammatory parameters of patients, we assessed the relationship between WBC counts, neutrophil counts, PLT counts, and MPO levels from samples drawn on the same day. The results showed that plasma MPO levels were significantly positively correlated with WBC counts (r = 0.5250, p < 0.0001; Fig. 3A) and neutrophil counts (r = 0.5103, p < 0.0001; Fig. 3B) and negatively correlated with PLT counts (r = −0.4598, p < 0.0001; Fig. 3C) in HFRS patients.

Correlation between plasma MPO levels and inflammatory parameters in HFRS patients. The correlations between plasma MPO levels and WBC counts
Correlation between plasma MPO levels and renal function parameters in HFRS patients
Then we analyzed the relationship between plasma MPO levels and the renal function parameters of HFRS patients. The results showed that plasma MPO levels positively correlated with BUN levels (r = 0.3945, p = 0.0015; Fig. 4A), UA levels (r = 0.2443, p = 0.0415; Fig. 4B), and Cr levels (r = 0.4047, p = 0.0005; Fig. 4C).
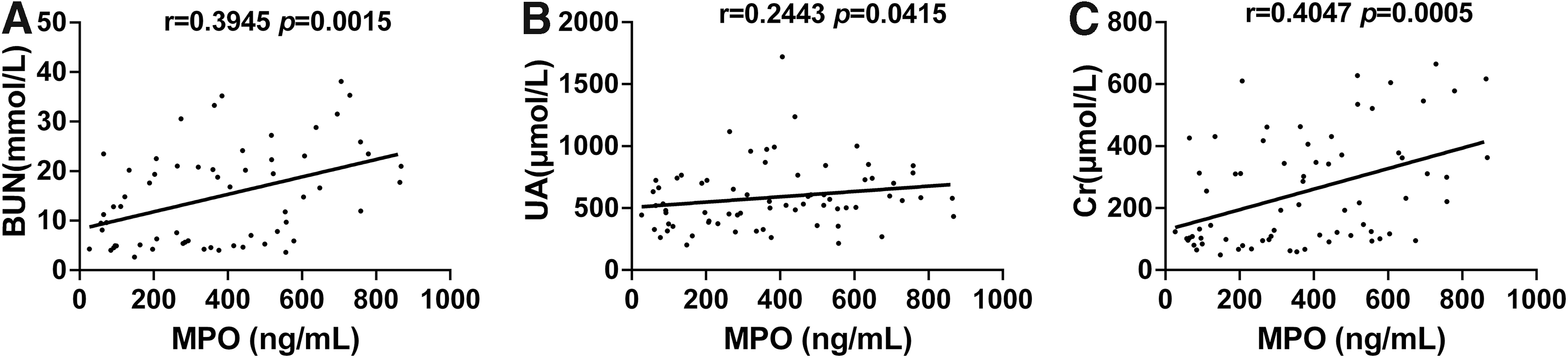
Correlation between plasma MPO levels and renal function parameters in HFRS patients. The correlations between plasma MPO levels and BUN levels
Increased levels of NPAs in both acute and convalescent phase of HFRS
To further assess the level of NPAs in HFRS patients, the percentage expression of CD41 on neutrophils were analyzed (Fig. 5A). Significant increased levels of NPAs were identified in acute phase of HFRS compared with NC (p < 0.01; Fig. 5B). Moreover, an even much higher increases of NPAs in the convalescent phase occurred in most cases compared with acute phase and NCs (p < 0.0001 for both; Fig. 5B). In addition, HFRS patients with paired samples of acute and convalescent phase showed a tendency of an increasing percentage of NPAs in the convalescent phase compared with that in the acute phase (Fig. 5C). These results indicated the importance of NPAs formation for HFRS after HTNV infection.
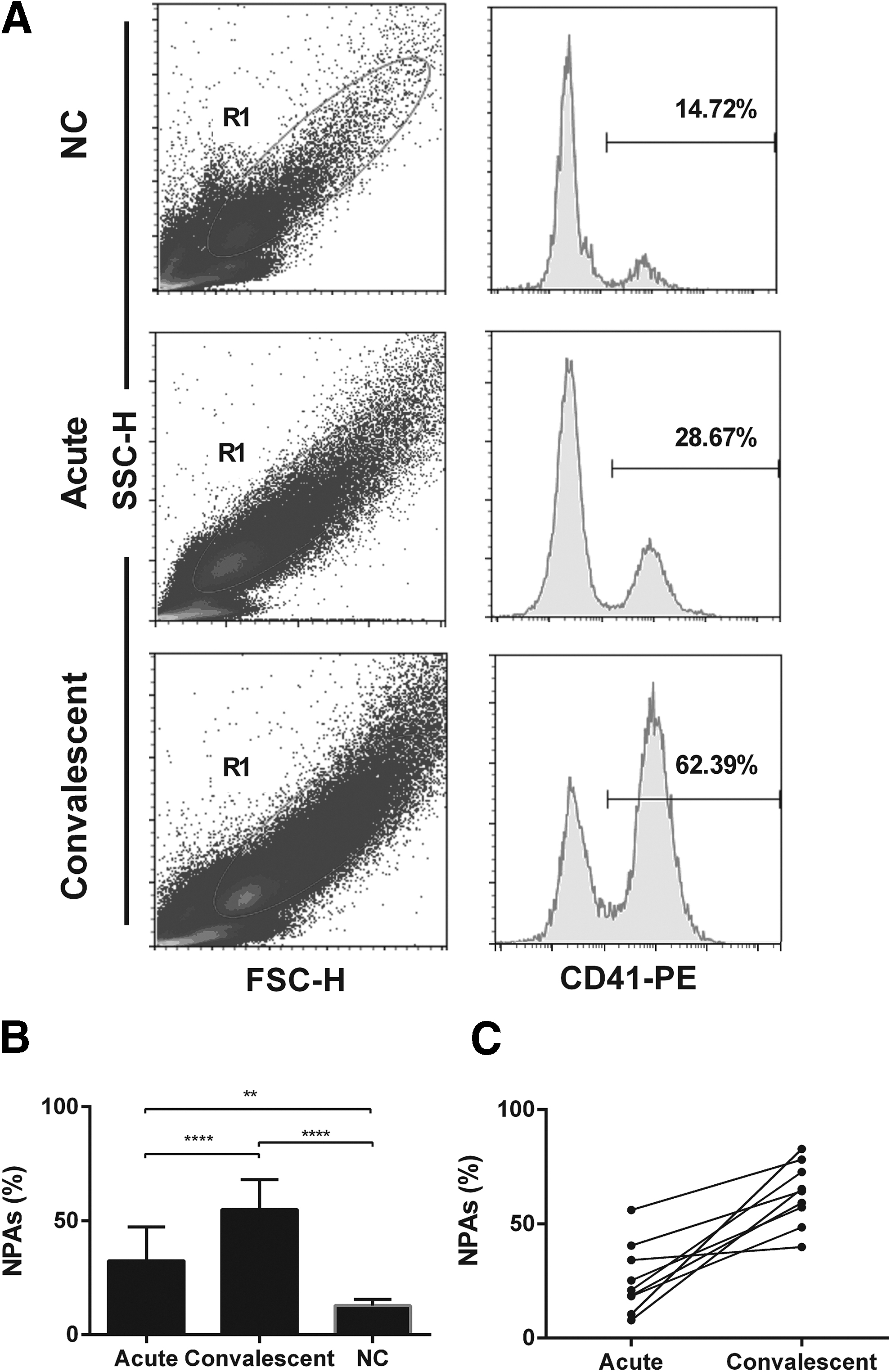
NPAs increased both in acute and convalescent phase of HFRS.
Discussion
HFRS is characterized by vascular leakage, thrombocytopenia, and acute kidney injury, which is immune-mediated, and inflammation imparts tissue damage and pathogenesis. More recently, the contribution of neutrophils to HTV infectious diseases has been observed, including neutrophil-derived factors and interaction between neutrophils and other cells (Schönrich et al., 2015). In this study, we found that the plasma MPO levels elevated in acute phase and critical/severe groups of HFRS patients correlated with disease severity. However, MPO-DNA levels had no relationship with the severity and duration of the disease, which suggests that neutrophils play an important role in the pathological response after HTNV infection mainly through MPO release but do not form NETs. In addition, NPAs increased both in acute and convalescent phases in HFRS patients when compared with NCs, which also implies that immune regulation of neutrophils in HFRS not only occurred in the early stage of the disease but also in the recovery phases.
MPO is an active substance released after neutrophils are activated to carry out oxidative killing of pathogens and body tissues. Previous studies have confirmed that MPO causes endothelial dysfunction through multiple pathways. MPO produces derived oxides such as hypochlorous acid (HOCL), hypothiocyanous acid, and hypobromous acid through halogenation cycles in vivo (Nussbaum et al., 2013; Vanhamme et al., 2018), in which HOCL can not only oxidize endothelial nitric oxide synthase and reduce the bioavailability of nitric oxide but also oxidize laminin and damage the basement membrane or induce vascular endothelial cell apoptosis; MPO itself can also cause endothelial cell damage through a variety of pathways, such as inducing endothelial glycocalyx collapse and promoting the recruitment and activation of neutrophils, or activating calpain, resulting in increased vascular cell adhesion molecule expression, thereby promoting leukocyte adhesion, the inflammatory response, and other ways to damage endothelial function (Etwebi et al., 2018; Manchanda et al., 2018).
In addition, elevated serum UA in HFRS patients is usually thought to result from renal injury, but it has also been shown that MPO is enzymatically involved in the process of oxidation of xanthine by endothelial xanthine oxidase to accumulate UA (Hage et al., 2020; Stamp et al., 2014). Our findings showed that plasma MPO was positively correlated with not only inflammatory parameters but also serum UA levels, BUN levels, and Cr levels in HFRS patients, suggesting that MPO can reflect the severity of HFRS to a certain extent, and whether MPO is involved in HFRS vascular endothelial cell inflammation and kidney injury needs further functional study.
In addition to its role in release into the blood through neutrophil degranulation, MPO is also present in NETs formed after neutrophils undergo apoptosis through the NETosis pathway (Papayannopoulos et al., 2010). MPO is not only an important component of NETs but also an essential condition for NET formation, and MPO-DNA is, therefore, also considered to be probably the most specific method for detecting NETosis at present (Masuda et al., 2016; Vorobjeva and Chernyak, 2020). In vitro studies have shown that hantaviruses can activate neutrophils through β2 integrin signaling resulting in NETosis (Raftery et al., 2014).
In addition, activated endothelial cells recruit neutrophils and the interactions through β2 integrins also result in NETosis during PUUV infection (Strandin et al., 2018). Our findings show that there was no difference in MPO-DNA between groups of different severities and disease phases, indicating that NETs might not be the main pathway involved in neutrophil responses in patients with HTNV infection. These results are consistent with previous studies showing that, when presented with microbes, neutrophils may respond in different ways, with some neutrophils consuming MPO through phagocytosis or degranulation, whereas others forming NETs (Papayannopoulos et al., 2010).
NPAs are a fundamental mechanism linking hemostasis and inflammatory processes of the innate immune system (Soehnlein, 2018). Studies have shown that formation of NPAs can be observed in virus infectious disease, such as HIV infection (Nkambule et al., 2015), human influenza infection (Koupenova et al., 2019), and COVID-19 (Manne et al., 2020), leading to mutual activation of both platelets and neutrophils along with cytokine release, NETs formation, and facilitate these cells gathering together at site of inflammation. In this study, the percentage of NPAs upregulated in the acute phase and increased even much higher in the convalescent phase.
More importantly, no NETs formed during acute and convalescent phase of HFRS. Studies have shown that, in a model of heat-induced liver injury, platelets immediately attach to the endothelium adjacent to the site of injury, which is required for subsequent neutrophil influx, and these neutrophils assist in the wound-healing response without the formation of NETs (Slaba et al., 2015). However, these repairs are based on the adhesion of NPAs with the endothelium, not in the circulation. The function of NPAs upregulated in acute and convalescent phase in HFRS needs to be explored in the future studies.
Conclusions
In conclusion, elevated plasma MPO in HFRS patients correlated with disease severity, together with the increases of NPAs both in acute and convalescent phase of HFRS, which may provide new insights into potential role of neutrophils in the pathogenesis of HFRS.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was supported by the National Natural Science Foundation of China (Grant Nos. 81771705 and 81871239).