
Abstract
Middle East respiratory syndrome coronavirus (MERS-CoV) is associated with significant morbidity and mortality. This study was performed to assess the proinflammatory cytokines profile among MERS-CoV patients. A total of 46 MERS-CoV–infected patients (27 symptomatic and 19 asymptomatic) were assessed and compared with 52 normal healthy controls for plasma levels of interleukin (IL)-1β, tumor necrosis factor (TNF)-α, IL-17, IL-7, IL-6, interferon (IFN)-α, and IL-15 using a customized luminex kit. Whereas asymptomatic MERS-CoV patients and controls were no different; the mean plasma levels among MERS-CoV symptomatic patients were significantly higher than the normal controls: IL-1β (16.89 ± 1.23 vs. 12.80 ± 0.59 pg/mL; p < 0.001), TNF-α (14.04 ± 0.93 vs. 10.35 ± 0.29 pg/mL; p < 0.0001), IL-17 (14.3 ± 0.89 vs. 11.47 ± 0.61 pg/mL; p < 0.001), IL-7 (21.56 ± 1.00 vs. 16.31 ± 0.30 pg/mL; p < 0.0001), IL-6 (156.5 ± 37.90 vs. 18.60 ± 1.59 pg/mL; p < 0.0001), and IFN-α (68.73 ± 13.06 vs. 23.57 ± 1.05 pg/mL; p < 0.0001). The mean plasma levels of IL-7 (24.81 ± 1.63 vs. 19.79 ± 0.94 pg/mL; p < 0.01), IL-6 (312.7 ± 94.67 vs. 101.2 ± 25.67 pg/mL; p < 0.01), and IFN-α (89.00 ± 18.97 vs. 51.05 ± 8.68 pg/mL; p < 0.05) were significantly elevated among MERS-CoV symptomatic patients with fatal outcome compared with MERS-CoV symptomatic patients who survived. Only IL-7 was found to have a higher risk ratio of mortality (4.76, 95% confidence interval: 1.5–14.94; p < 0.01). No differences were observed in IL-15 levels among the groups. Significantly elevated proinflammatory cytokines among symptomatic MERS-CoV–infected patients may contribute to manifestations of cytokine storm frequently observed among critically ill MERS-CoV patients and IL-7 may serve as a marker for disease activity.
Introduction
The Middle East respiratory syndrome coronavirus (MERS-CoV) belongs to a group of beta-coronaviruses. It emerged in Saudi Arabia in 2012 (Zaki et al., 2012) and remains a global public health concern. Since the emergence of MERS-CoV World Health Organization has reported 2,591 cases including 894 deaths globally by May 2022. Majority of cases have been reported from Saudi Arabia where multiple nosocomial outbreaks caused significant morbidity and mortality (Alenazi et al., 2017; Amer et al., 2018; Assiri et al., 2013; Balkhy et al., 2016; Barry et al., 2020; Drosten et al., 2015; Fagbo et al., 2015). MERS-CoV is a zoonotic infection that originated in bats with dromedary camels as intermediate reservoir (Dudas et al., 2018; Mackay and Arden, 2015).
This virus preferentially infects the lower respiratory airways and may cause intense respiratory dysfunction with substantial mortality particularly among patients with comorbidities such as chronic lung, heart, and kidney diseases, diabetes, and hypertension (Garbati et al., 2016). The clinical presentation of MERS-CoV infection is variable, ranging from asymptomatic or mild disease to critical illness resulting in acute respiratory distress syndrome (ARDS), cytokine storm, and multiorgan failure. The mechanisms involved in disease pathogenesis are still not fully understood (Widagdo et al., 2019).
Innate and adaptive immune responses play an important role in the pathogenesis of MERS-CoV (Akdis et al., 2011). Among numerous immunological responses evoked against MERS-CoV infection, proinflammatory cytokines and chemokines are considered to be the key factors influencing the outcomes (Akdis et al., 2011). Proinflammatory cytokines are low molecular weight proteins induced by several factors such as infection, immune-activated T cells, toxins, ischemia, and trauma. These cytokines regulate activation, growth, differentiation, and migration of the immune cells to the site of infection (Dinarello, 2000; Turner et al., 2014). The key proinflammatory cytokines include interleukin (IL)-1, IL-6, tumor necrosis factor (TNF)-α, IL-33, interferon (IFN)-α, IL-12, IL-17, IL-18, and IL-8 (Dinarello, 2000). These cytokines are produced predominantly by activated macrophages and mesenchymal cells such as fibroblasts, and epithelial and endothelial cells.
Induction of these cytokines result in upregulation of inflammatory reactions and production of acute phase proteins that induce fever, inflammation, tissue destruction, and, in a few instances, shock and death (Dinarello, 2000). The outcome of inflammatory response is usually determined by the balance between proinflammatory and anti-inflammatory cytokines. In addition, IL-1 and TNF-α induce endothelial adhesion molecules, which are crucial for the adhesion of leukocytes to the endothelial surface before extravascular migration into the tissues (Dinarello, 2000). Moreover, proinflammatory cytokines such as IL-1, IL-6, and TNF-α are involved in the pathogenesis and propagation of respiratory viral infections (Clementi et al., 2021; Vazquez et al., 2019; Zhou et al., 2014). To better understand the role of proinflammatory cytokines in MERS-CoV infection, we assessed the blood levels of proinflammatory cytokines among symptomatic and asymptomatic patients infected with MERS-CoV.
Materials and Methods
Study population
This cross-sectional study was performed to assess the levels of proinflammatory cytokines among MERS-CoV patients between January 2018 and September 2019. Details of the patients included in the study groups are described in Table 1. A total of 46 MERS-CoV–infected patients (22 men and 24 women) with the mean age 50.9 ± 17.7 years were included in the study. Among the MERS-CoV–infected group, 19 patients were asymptomatic, whereas 27 patients had symptoms and among them 8 patients died. The most common symptoms among the symptomatic patients were fever in 19 (41.3%) patients followed by cough in 10 (21.7%). The most frequent comorbidity was diabetes mellitus in 8 (17.4%) followed by hypertension in 4 (8.7%) patients (Table 1). Blood samples were collected during the acute phase of the infection, within 24 h of laboratory confirmation of MERS-CoV infection.
Demographic and Clinical Details of Middle East Respiratory Syndrome Coronavirus–Positive Patients
SOB, shortness of breathing; DM, diabetes mellitus; HTN, hypertension, HF, heart failure; CAD, coronary artery disease.
None of the patients was receiving any antiviral or immunosuppressive therapy at the time of collection of blood samples. In addition, a group of 52 randomly selected normal healthy individuals (mean age 38.1 ± 13.7 years) was also included in the study as a control group. All the normal controls tested negative for human immunodeficiency virus, hepatitis viruses B and C, and human T lymphocytic leukemia virus. This study was approved by the College of Medicine Institutional Review Board (IRB), project # E15-1625, and all patients signed an informed consent.
Measurement of proinflammatory cytokines and chemokines
The plasma levels of IL-1β, IL-6, TNF-α, IFN-α, IL-7, IL-15, and IL-17A among patients and controls were measured by luminex customized proinflammatory human cytokine magnetic plex panel (Novex Life Technologies) in accordance with the manufacturer's instructions. In brief, the standard human cytokines one and two were reconstituted by adding the assay diluent (500 μL) to the lyophilized cytokine standard and incubated at room temperature for 15 min. The top standards were prepared by transferring 300 μL of each standard into a sterile tube and this was followed by preparation of 1:3 serial dilutions. Then, 25 μL of antibody beads solution was dispensed into each well of 96-well microtiter plate and incubated for 1 min on magnet. The plate was washed twice with 200 μL of washing solution and 50 μL of incubation buffer was added to all wells.
Subsequently, 50 μL of assay diluent with 50 μL of plasma samples were added to the samples wells. One hundred microliters of each standard was added to the wells. The plate was then covered and incubated at 4°C on a shaker in dark overnight. After the incubation the plate was washed twice with 200 μL of washing solution, and 100 μL of biotinylated detector antibody was added and incubated for 1 h on a shaker in dark. The plate was then washed twice with 200 μL of washing solution and 100 μL of streptavidin–R-Phycoerythrin (RPE) solution was added and incubated for 30 min on a shaker in the dark.
Finally, the plate was washed three times with 200 μL of washing solution and resuspended in 150 μL of washing solution and was shaken for 3 min before being read by luminex MAGPIX system. Interpretation of the results was performed using xPONENT software and the concentrations of cytokines were expressed in pg/mL. The analytical sensitivities for IL-1β, IFN-α, IL-7 and IL-15 were <5 pg/mL; IL-6 and TNF-α were <0.5 pg/mL; and IL-17A was <1 pg/mL.
Diagnosis of MERS-CoV infection
MERS-CoV RNA extraction and detection was performed as described previously (Alhetheel et al., 2017). In brief, total nucleic acid was extracted from 300 μL of each specimen in viral transport medium using Nucleic Acid Isolation Kit I and MagNA Pure Compact system (Roche Applied Science) and eluted with a final volume of 50 μL. A 10 μL of the extracted RNA was reverse transcribed into cDNA using random primer. The cDNA was amplified for the detection of MERS-CoV genes UpE and Orf1A using specific primers and probes of the Altona kit (Humburg, Germany) and Rotergene instrument (Qiagen, Santa Clarita, CA). The diagnosis of MERS-CoV infection was confirmed by the detection of both UpE and Orf1a genes.
Statistical analysis
Data were statistically analyzed using GraphPad Prism 5 software. The statistical analysis between all groups was performed using one-way analysis of variance. Statistical analysis between two groups was performed using nonpaired t-test. The risk ratio for mortality was determined using Fisher exact probability test. A two-tailed p ≤ 0.05 was considered statistically significant.
Results
Comparative analysis of data between MERS-CoV–infected patients and the normal healthy controls revealed increased levels of proinflammatory cytokines among symptomatic patients with MERS-CoV infection. The mean plasma levels of IL-1β (16.89 ± 1.23 vs. 12.80 ± 0.59 pg/mL; p < 0.001), TNF-α (14.04 ± 0.93 vs. 10.35 ± 0.29 pg/mL; p < 0.0001), IL-17 (14.33 ± 0.89 vs. 11.47 ± 0.61 pg/mL; p < 0.001), IL-7 (21.56 ± 1.00 vs. 16.31 ± 0.30 pg/mL; p < 0.0001), IL-6 (156.5 ± 37.90 vs. 18.60 ± 1.59 pg/mL; p < 0.0001), and IFN-α (68.73 ± 13.06 vs. 23.57 ± 1.05 pg/mL; p < 0.0001) among MERS-CoV–infected patients were significantly higher than the normal controls (Fig. 1A–F).
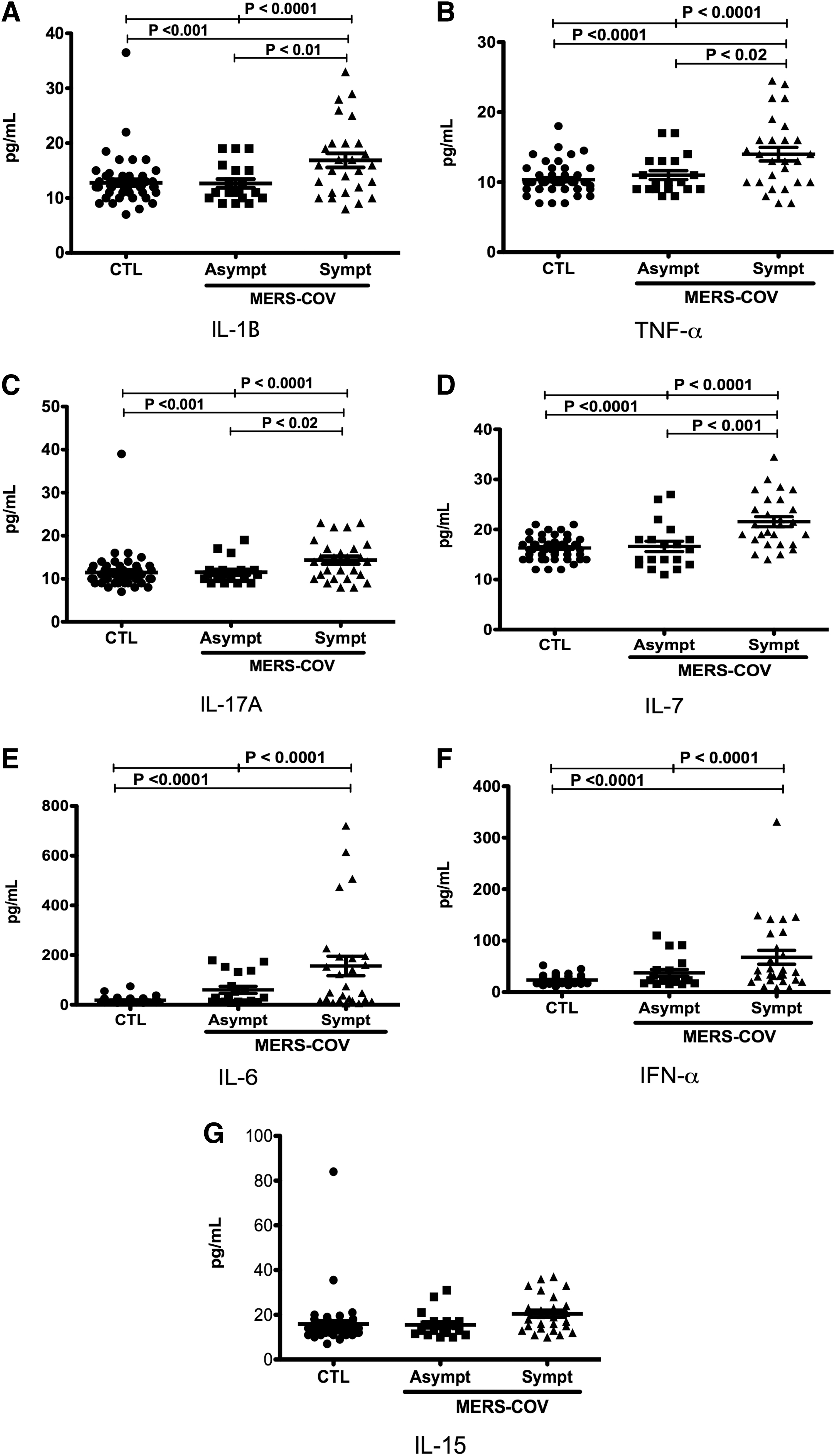
Human proinflammatory cytokines levels in patient study groups. Plasma of symptomatic (n = 27) and asymptomatic (n = 19) MERS-CoV patients along with healthy controls (CTL) (n = 52) were collected and cytokines were analyzed using luminex customized proinflammatory cytokine magnetic plex panel and luminex MAGPIX system. The mean levels of IL-1β
Similarly, the mean plasma levels of IL-1β (16.89 ± 1.23 vs. 12.66 ± 0.80 pg/mL; p < 0.01), TNF-α (14.04 ± 0.93 vs. 11.00 ± 0.63 pg/mL; p < 0.02), IL-17 (14.33 ± 0.89 vs. 11.53 ± 0.65 pg/mL; p < 0.02), and IL-7 (21.56 ± 1.00 vs. 16.63 ± 1.041 pg/mL; p < 0.001) in symptomatic MERS-CoV patients were significantly higher than the asymptomatic MERS-CoV patients (Fig. 1A, D). No statistically significant differences were observed between symptomatic MERS-CoV patients and asymptomatic MERS-CoV patients for mean plasma levels of IL-6 (156.0 ± 39.38 vs. 60.08 ± 14.18 pg/mL; p = 0.051) and IFN-α (67.61 ± 13.51 vs. 37.24 ± 6.64 pg/mL; p = 0.08) (Fig. 1E, F).
In addition, no statistically significant differences were observed between symptomatic MERS-CoV patients, asymptomatic MERS-CoV patients, and normal controls for mean plasma levels of IL-15 (20.46 ± 1.54 pg/mL vs. 15.47 ± 1.31 pg/mL vs. 15.82 ± 1.45 pg/mL), respectively (Fig. 1G). The mean plasma levels of IL-7 (24.81 ± 1.63 vs. 19.79 ± 0.94 pg/mL; p < 0.01), IL-6 (312.7 ± 94.67 vs. 101.2 ± 25.67 pg/mL; p < 0.01), and IFN-α (89.00 ± 18.97 vs. 51.05 ± 8.68 pg/mL; p < 0.05) were significantly elevated among MERS-CoV symptomatic patients with fatal outcome compared with MERS-CoV symptomatic patients who survived (Fig. 2D–F).

Human proinflammatory cytokines levels in survived and died Symptomatic MERS-CoV patients. Plasma of symptomatic MERS-CoV patients survived (n = 19) and symptomatic died (n = 8) were collected and cytokines were analyzed using luminex customized proinflammatory cytokine magnetic plex panel and luminex MAGPIX system. The mean levels of IL-1β
No statistically significant differences were observed between symptomatic MERS-CoV with fatal outcome and survived patients for the levels of IL-1β (19.50 ± 2.78 vs. 16.00 ± 1.09 pg/mL), TNF-α (15.56 ± 1.86 vs. 13.74 ± 0.88 pg/mL), IL-17 (15.88 ± 1.79 vs. 14.11 ± 0.86 pg/mL), and IL-15 (23.88 ± 2.67 vs. 19.84 ± 1.66 pg/mL) (Fig. 2A–C, G). IL-7 was the only cytokine found to have a higher risk ratio of mortality (4.76, 95% confidence interval: 1.5–14.94; p < 0.01) (Table 2). No difference in cytokine levels was observed between asymptomatic MERS-CoV patients and normal controls.
The Risk Ratio of Mortality for All Cytokines Tested
Statistically significant.
IFN, interferon; IL, interleukin; TNF, tumor necrosis factor.
Discussion
Proinflammatory cytokine levels were increased in the symptomatic MERS-CoV–infected patients. In concordance with these findings it has been shown previously that cytokines such as IL-1β, IFN-α, TNF-α, and IL-17 were significantly elevated in MERS-CoV–infected patients (Alosaimi et al., 2020; Scheuplein et al., 2015). Clinical features such as fever, cough, dyspnea, fatigue, and pneumonia among coronavirus disease 2019 (COVID-19), severe acute respiratory syndrome coronavirus (SARS-CoV), and MERS-CoV patients have been attributed to increased production of inflammatory mediators along with virus-induced immunopathology that propagates acute lung injury inducing ARDS (Channappanavar and Perlman, 2017; D'Elia et al., 2013). It has been clearly demonstrated in SARS and MERS animal models that the delayed type I IFN response induces hyperinflammation by promoting pulmonary infiltration of neutrophils and macrophages, the main sources of proinflammatory cytokines that play a critical role in inducting ARDS (Jamilloux et al., 2020).
Although IFN response is considered to be protective in SARS-CoV and MERS-CoV infections, the type I IFN-mediated antiviral activity is inhibited in both infections (Kindler et al., 2016; Shokri et al., 2019), resulting in enhancement of disease severity in both conditions (Channappanavar and Perlman, 2017; Prompetchara et al., 2020). MERS-CoV–infected human plasmacytoid dendritic cells (DCs), on the contrary, have been shown to produce large amounts of types I and III IFNs, particularly IFN-α (Scheuplein et al., 2015), which is consistent with the findings of this study. It has recently been reported that both Th1 and Th2 immune responses are downregulated in MERS-CoV infection that have been attributed to the upsurge of proinflammatory cytokines such as IL-1α, IL-1β, and IL-8 (Alosaimi et al., 2020). Collectively these observations indicate that the data for cytokine profile in MERS-CoV remain inconclusive.
Serum levels of proinflammatory cytokines such as IFN, TNF-α, IL-6, and IL-17 among symptomatic patients with MERS-CoV infection were elevated in this study. In vitro studies of alveolar epithelial cell infection with MERS-CoV have clearly demonstrated increased production of IFN-γ and other proinflammatory cytokines including IL-1β, IL-6, and IL-8 (Lau et al., 2013). The main sources of these cytokines are monocytes and neutrophils and the levels of proinflammatory cytokine exhibit a positive correlation with the cell counts of monocytes and neutrophils (Kim et al., 2016). Moreover, serum levels of IL-6, IL-8, and IFN-α among severely ill patient with MERS-CoV have been reported to be higher than patients with mild MERS-CoV infection (Min et al., 2016). Similar findings were also observed in this study where symptomatic MERS-CoV patients were harboring higher concentrations of proinflammatory cytokines in their blood compared with asymptomatic patients with MERS-CoV infection or healthy normal controls.
Elevation of plasma levels of IL-17A was also observed in this study among symptomatic MERS-CoV patients, which was in agreement with previous findings of both in vivo (Faure et al., 2014) and in vitro studies (Josset et al., 2013). This cytokine induces recruitment of monocytes and neutrophils at the site of inflammation and plays a critical role in airway remodeling during pulmonary infection or allergic inflammation by enhancing the production of proinflammatory cytokines and chemokines (Lee et al., 2016). This was evident in a study reporting markedly increased levels of IL-17 among MERS-CoV patients along with elevated levels of a number of other proinflammatory cytokines including of IFN-γ, TNF-α, and IL-15. A prominent proinflammatory Th1 and Th17 response was clearly seen in patients with MERS-CoV infection, with markedly increased concentrations and IL-17 compared with controls (Mahallawi et al., 2018). These observations suggest that IL-17 is not only an important component of MER-CoV–associated cytokine storm, but it also contributes to the enhancement of its severity.
Among the symptomatic patients with MERS-CoV infection fatal outcome was observed in a group of patients with significantly higher blood levels of IL-7 compared with symptomatic patients who survived. It has recently been reported that COVID-19–infected patients in the intensive care unit (ICU) had significantly higher levels of IL-7 compared with non-ICU patients and normal controls (Huang et al., 2020). Similarly, elevated blood levels of IL-7 among mild, moderate, and severely ill patients with COVID-19 infection were found to be significantly higher compared with normal controls (Chi et al., 2020). Moreover, same study reported significantly higher levels of IL-7 in severely ill patients compared with mild and moderately ill groups of patients with COVID-19 infection suggesting the use of IL-7 blood levels as a possible marker of disease severity in COVID-19 infection. In addition, it has been observed that male patients have a higher risk of hospitalization and death compared with female patients (Peckham et al., 2020) and the available evidence confirms that male patients harbor significantly higher levels of IL-7 compared with female COVID-19 patients (Chi et al., 2020). It is therefore conceivable that elevated levels of IL-7 observed in this study could possibly reflect similar role of IL-7 in MERS-CoV infection.
Production of proinflammatory cytokines following MERS-CoV infection is critical for host defense. Expression of proinflammatory cytokines, including IL-6, IL-8, IFN-γ, or IP-10, has been shown to correlate with the severity of disease and mortality (Huang et al., 2005). The source of elevated blood levels of proinflammatory cytokines in MERS-CoV infection is believed to be the alveolar macrophages triggering the cytokine storm and inflicting damage to the neighboring lung tissues (Nicholls et al., 2003; Zhou et al., 2014). Elevated levels of IL-6 and TNF-α are the indicators of severe respiratory viral infection and it is possible that elevated blood levels of IFN-γ may cause severe MERS disease (Jiang et al., 2005). IFN response in mild cases of MERS-CoV infection is low or absent compared with severely ill patients (Kim et al., 2016). Elevated blood levels of IFN-γ in severely ill patients suggest the critical role of this cytokine. In vitro infection of human leukemia monocytic cell line (THP-1) cells, macrophages, and DCs derived from human peripheral blood monocytes by MERS-CoV triggers production of proinflammatory cytokines and chemokines and form a positive feedback response, eventually leading to a cytokine storm (Tynell et al., 2016; Zhou et al., 2014). These observations indicate that viral load appears to be critical for induction of cytokine storm and the associated morbidity and mortality of MERS-CoV.
Conclusion
Proinflammatory cytokine levels were increased in symptomatic MERS-CoV–infected patients. These observations indicate that clinical presentation of MERS-CoV–infected patients may have a correlation with the blood concentrations of proinflammatory cytokines and IL-7 may serve as a marker for disease activity. Data describing cytokine profile of MERS-CoV patients are inconsistent, which could be owing to variations in disease severity, presence of comorbidities, and differing age of the patients. Further investigation during different phases of the disease and the associated comorbidities may provide a better insight into the pathogenesis of MERS-CoV infection.
Footnotes
Acknowledgments
The authors thank King Khalid University Hospital and Prince Mohammed Bin Abdulaziz Hospital for the help in providing patients samples.
Authors' Contributions
A.A. and A.A.: designed the study, conceived the idea, performed experiments, data analysis, and prepared the article draft; Z.S., A.S., H.A., and M.B.: contributed to software data analysis, writing, reviewing and editing the article; M.N., M.B., M.A., A.A., S.A., and Z.M.: contributed to data collection, data analysis, writing, reviewing, and editing the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The research project was funded by the King Abdulaziz City for Science and Technology (research Grant No. 1–02).