
Abstract
Chronic hepatitis C is a major health concern with high morbidity and mortality rates. The introduction of direct acting antivirals (DAAs) as a first-line treatment for hepatitis C virus (HCV) has significantly enhanced HCV eradication. However, DAA therapy is facing rising concerns regarding long-term safety, viral resistance, and reinfection. HCV is associated with different immune alteration mechanisms that can evade immunity and establish persistent infection. One of these suggested mechanisms is the accumulation of myeloid-derived suppressor cells (MDSCs), which is known to accumulate in chronic inflammatory conditions. Moreover, the role of DAA in restoring immunity after successful viral eradication is still unclear and needs further investigations. Thus, we aimed to investigate the role of MDSCs in chronic HCV Egyptian patients and its response to DAA in treated compared with untreated patients. Fifty untreated chronic hepatitis C (CHC) patients, 50 DAA-treated CHC patients, and 30 healthy individuals were recruited. We used flow cytometer analysis to measure MDSCs frequency and enzyme-linked immunosorbent assay analysis to evaluate the serum level of interferon (IFN)-γ. We found a significant elevation in MDSC% among the untreated group (34.5 ± 12.4%) compared with the DAA-treated group (18.3 ± 6.7%), while the control group had a mean of (3.8 ± 1.6%). IFN-γ concentration was higher in treated patients compared with untreated. We also found a significant negative correlation (rs −0.662) (p < 0.001) between MDSC% and IFN-γ concentration among treated HCV patients. Our results revealed important evidence of MDSCs accumulation in CHC patients and partial retrieval of the immune system regulatory function after DAA therapy.
Introduction
Chronic hepatitis C virus (HCV) infection estimates are ∼70 million people worldwide as estimated by the World Health Organization (WHO), causing ∼400,000 deaths every year and ∼3–4 million new infections each year (Wo Dore et al, 2020). Around 30% of these deaths are linked to long-term HCV-related outcomes; cirrhosis and hepatocellular carcinoma (HCC) (WHO, 2021). Egypt is reported to be one of the most HCV-infected areas worldwide with a viremic prevalence of 6.3% compared with the global prevalence of 1% (Blach et al, 2017). The predominant genotype of HCV in chronic hepatitis C (CHC) patients in Egypt has been identified as genotype 4 (Messina et al, 2015).
HCV is a chronic infection that mediates several alterations in both innate and adaptive immunity to evade host immunity and promote virus persistence (Park and Rehermann, 2014). One of these alterations is the accumulation of immune suppressive cells (myeloid-derived suppressor cells [MDSCs]), which in turn induce further immune suppression and augment persistence of the infection (Telatin et al, 2019). Moreover, ongoing research suggests that MDSCs can mediate viral immune evasion parallel to that of tumor evasion mechanisms. Furthermore, recent studies suggest a potential role of MDSCs not only in chronic nature of HCV disease but also in HCV-induced HCC (Bowers et al, 2014; Norris et al, 2013; Wang et al, 2018; Wang et al, 2016).
MDSCs are myeloid cells that are activated in pathological instances due to aberrant myelopoiesis such as cancer, inflammatory and infectious diseases; they are relatively immature and involved in immunological regulation of many pathological conditions (Gabrilovich, 2017). They have some characteristics that distinguish them from monocytes and neutrophils such as potent suppressive activity, a distinct gene expression profile, and biochemical characteristics (Solito et al, 2019) with monocytic and granulocytic features that can negatively regulate T-cell function (Talmadge and Gabrilovich, 2013).
Human MDSCs express a variety of myeloid cell markers, such as CD11b+ and CD33+, but they usually lack HLA-DR and lineage-specific antigens, such as CD3, CD19, and CD57 (Damuzzo et al, 2015). MDSC expansion has been identified as an important pathophysiological principle in cancer and chronic inflammatory conditions (de Coaña et al, 2017).
The introduction of oral direct acting antiviral (DAA) therapy, which constitutes a highly effective and tolerable, short-duration treatment modality, gave momentum to HCV elimination targets (Yehia et al, 2014). Although they have reached 90–100% cure rate regardless of HCV genotype, DAAs do not prevent HCV reinfection (Wijaya et al, 2021). Moreover, CHC is still associated with many challenges; a great percentage of patients with CHC are from low- and middle-income countries with large population and financial limitation to expensive therapies with DAAs that are the most efficient in the treatment of chronic HCV infection (Leblebicioglu et al, 2018).
Furthermore, 85% of HCV cases are asymptomatic with a delayed diagnosis, which ends by complications development such as liver cirrhosis and HCC (Lapointe-Shaw et al, 2021). Currently, we are facing a new era with the use of DAA agents. However, the exact immunological effects of DAA therapy in CHC patients are not completely understood; it is unclear whether effective DAAs role in inhibiting HCV replication has a prominent effect on restoration of immune activity and surveillance capacity in HCV-cured patients, which raise the demand for further investigations (Li et al, 2019).
We aimed to unravel the role of MDSCs (CD33+ HLA-DR– CD11b+) in chronic HCV infection and its response to DAA therapy. Moreover, another aim of this study is to evaluate the serum level of interferon (IFN)-γ in those patients as a clue to the antiviral immunity developed against the CHC infection. Further knowledge needed to elucidate a potential mechanism for enhancing HCV treatment and augmenting its desired effects, and this may open the way for alternative treatment modality for CHC patients and help preventing the reinfection already observed in DAA-treated individuals.
Materials and Methods
Subjects: This study was conducted on 130 individuals aged ≥18 years, recruited from the outpatient hepatology clinic of The Medical Research Institute (MRI, Alexandria, Egypt) from October 2020 to December 2020, and classified as follows: 50 treatment-naïve CHC patients (diagnosed by positive HCV Ab test and viral PCR), 50 DAA-treated CHC patients using sofosbuvir 400 mg/day (Gratisovir® or Soflanork® or Heterosofir®), and Daclatasvir 60 mg/day (Daktavira® or Daclavirocyrl®) without ribavirin therapy fulfilling the inclusion criteria based on the protocol provided by the National Committee for Control of Viral Hepatitis (NCCHC) in Egypt.
The treated group had sustained viral response of 24 weeks after treatment completion (SVR24). We excluded patients with any of the following conditions: Child C cirrhotic patients, platelet count <50,000/μL, HCC, extrahepatic malignancy, pregnancy, inadequately controlled diabetes mellitus (HbA1c >8%), coinfection with HBV or HIV. The control group consisted of 30 healthy volunteered individuals (verified by negative HCV Ab test and normal liver function tests).
All patients were asked to freely volunteer to the study, and informed written consents were gathered before their inclusion in the study, according to the ethical guidelines of the MRI, Alexandria University.
MDSC% measurement by flowcytometric analysis
MDSC frequency was investigated using 100 μL of anticoagulated (EDTA-coated vacutainers) whole blood. Samples were stained with monoclonal antibodies, including fluorescein isothiocyanate mouse antihuman CD33 (BD Bioscience Pharmingen™, San Diego; Clone HIM3-4), phycoerythrin mouse antihuman CD11b/Mac-1 (BD Bioscience Pharmingen™; Clone ICRF44), and PerCP Anti-HLA-DR (L243; BD Biosciences, San Jose, CA). Samples were incubated in the dark at room temperature (20°C—25°C) for 15 min, and then RBCs were lysed using 2 mL of diluted lysing solution (BD Biosciences) for 10 min.
Finally, samples were washed twice using phosphate buffered saline (0.0067 M) and were ready to be analyzed using BD FACS Calibur™ flow cytometer system. The gating strategy for MDSCs frequency investigations was set (CD33+, CD11b+, and HLA-DR-/low).
IFN-γ concentration measurement using enzyme-linked immunosorbent assay analysis
Plasma samples were collected in dry clean Eppendorf tubes and preserved at −20°C until use. Interferon gamma level was then measured according to the instructions of the enzyme-linked immunosorbent assay kit manufacturer (BT Lab/cat E0105HU; Bioassay Technology Laboratory, Shanghai, China).
Statistical analysis of the data
Data were fed to the computer and analyzed using IBM SPSS software package version 20.0. (Armonk, NY: IBM Corp). Categorical data were represented as numbers and percentages. Chi-square test was applied to investigate the association between the categorical variables. For continuous data, they were tested for normality by the Shapiro-Wilk test. Quantitative data were expressed as range (minimum and maximum), mean, standard deviation, and median. For normally distributed quantitative variables, Student's t-test was used to compare two groups while one-way analysis of variance (ANOVA) test was used for comparing the three studied groups.
On the contrary, for not normally distributed quantitative variables the Mann–Whitney test was used to compare two groups, while the Kruskal–Wallis test was used to compare three groups, followed by post hoc test (Dunn's for multiple comparisons test) for pairwise comparison and the Spearman coefficient to correlate between not normally distributed quantitative variables. The significance of the obtained results was estimated at the 5% level.
Results
Demographic and laboratory data
Patients' age ranged from 18 to 68 years, and there was no significant difference in age or sex across the three study groups. Patients' demographic data and laboratory assessments are summarized in Table 1.
Comparison Between the Three Studied Groups According to Demographic Data and Laboratory Investigations
p: p-value for comparison between the studied groups.
Statistically significant at p ≤ 0.05.
ALT, alanine transaminase; AST, aspartate transaminase; INR, international normalized ratio; Max., maximum; Min., minimum; SCR, serum creatinine; SD, standard deviation; WBCs, white blood cells.
Assessment of MDSC's frequency
We observed a significant decrease in MDSC frequency among treated group compared with untreated, p 1 < 0.001. We also recognized that the treated group had higher MDSC frequency than healthy controls, p 3 < 0.001, as shown in Table 2 and Figure 1. We further investigated the correlation between MDSC% and laboratory data in Table 3. A significant positive correlation was found between alanine transaminase, aspartate transaminase, and MDSC% in both treated and untreated groups.
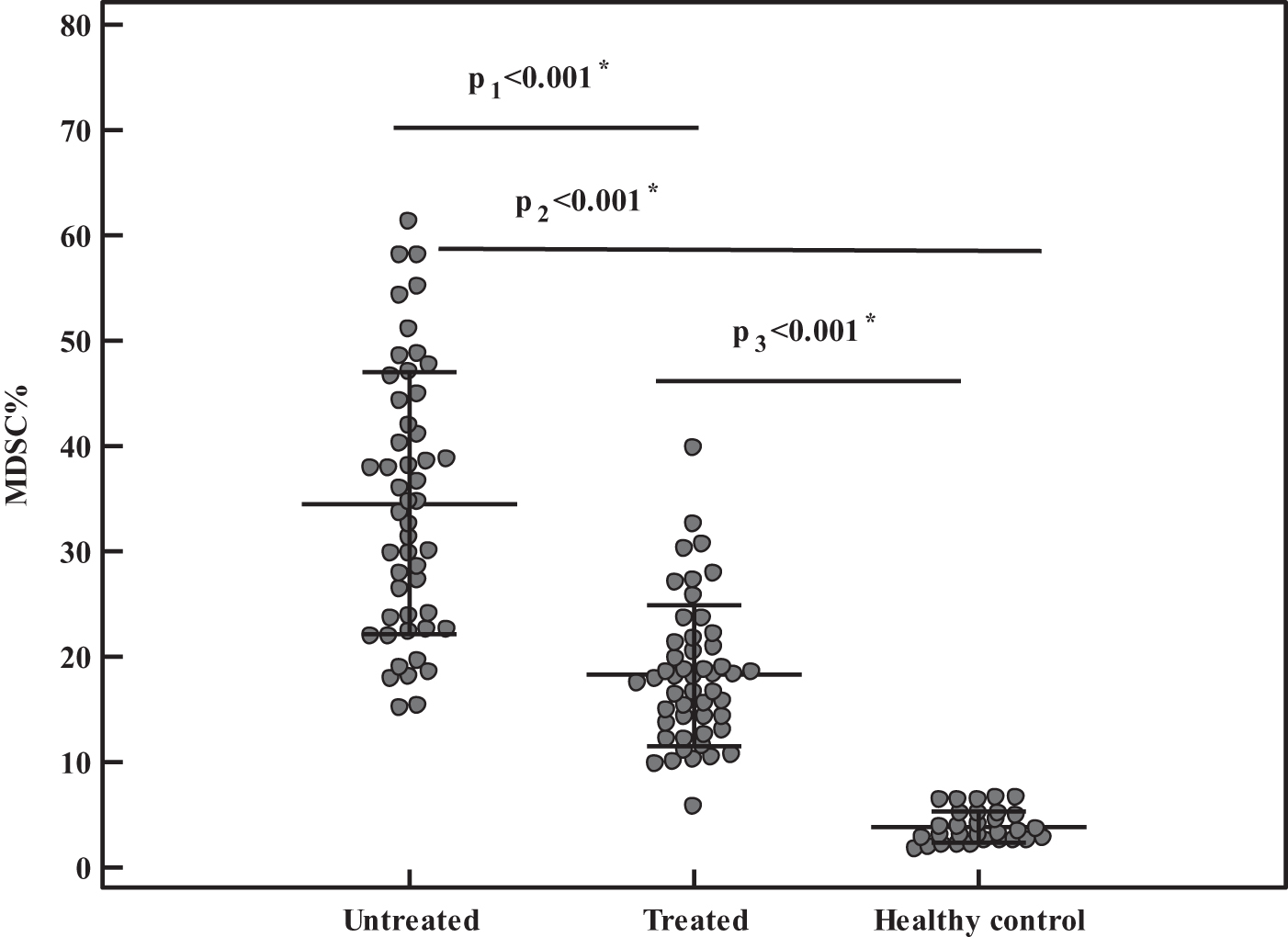
Comparison between the three studied groups according to MDSC. *Statistically significant at p ≤ 0.05. MDSC, myeloid-derived suppressor cell.
Comparison Between the Three Studied Groups According to Myeloid-Derived Suppressor Cell %
p: p-value for comparison between the studied groups.
p 1: p-value for comparison between untreated and treated.
p 2: p-value for comparison between untreated and healthy control.
p 3: p-value for comparison between treated and healthy control.
Statistically significant at p ≤ 0.05.
Medians with common letters are not significant (i.e., medians with different letters are significant).
MDSC, myeloid-derived suppressor cell.
Correlation Between Myeloid-Derived Suppressor Cell % and Laboratory Data in Each Group
Statistically significant at p ≤ 0.0.
rs , Spearman's coefficient.
Assessment of IFN-γ concentration
Comparison of IFN-γ concentration between the different study groups is summarized in Table 4. We found that HCV-treated patients had significantly higher IFN-γ concentration than untreated patients, p 1 < 0.001. On the contrary, healthy controls had lower IFN-γ concentration than both treated and untreated groups represented in Figure 2.
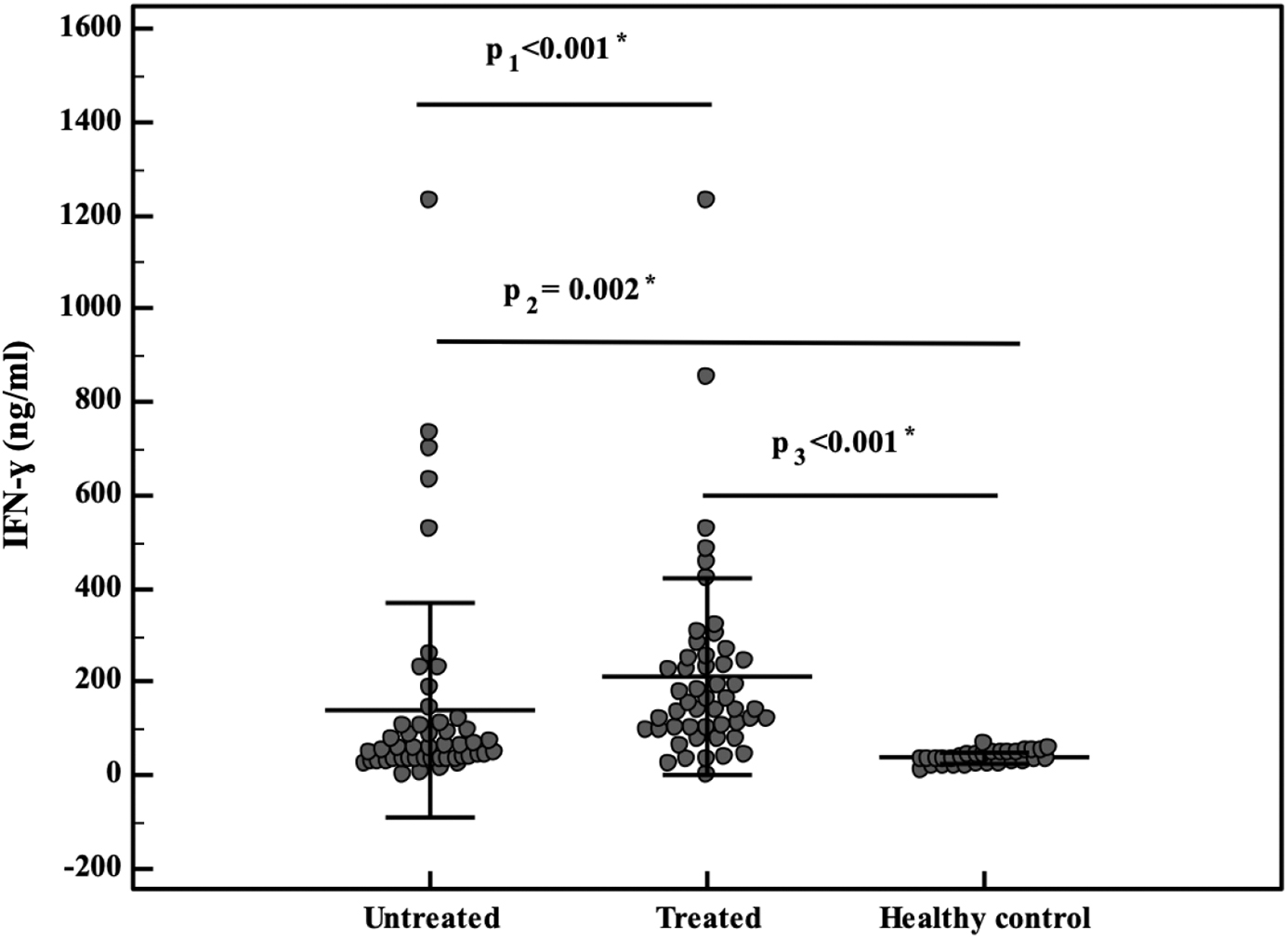
Comparison between the three studied groups according to IFN-γ concentration. *Statistically significant at p ≤ 0.05. IFN-γ, interferon γ.
Comparison Between the Three Studied Groups According to Interferon-γ Concentration
p: p-value for comparison between the studied groups.
p 1: p-value for comparison between untreated and treated.
p 2: p-value for comparison between untreated and healthy control.
p 3: p-value for comparison between treated and healthy control.
Statistically significant at p ≤ 0.05.
Medians with common letters are not significant (i.e., medians with different letters are significant).
IFN-γ, interferon γ.
Correlation between MDSC% and IFN-γ concentration
Correlation between MDSC frequency and IFN-γ concentration in the different study groups is summarized in Table 5. Data from the table show significant negative correlation between MDSC frequency and IFN-γ concentration among group 2 of treated HCV patients (p < 0.001*) represented in Figure 3.
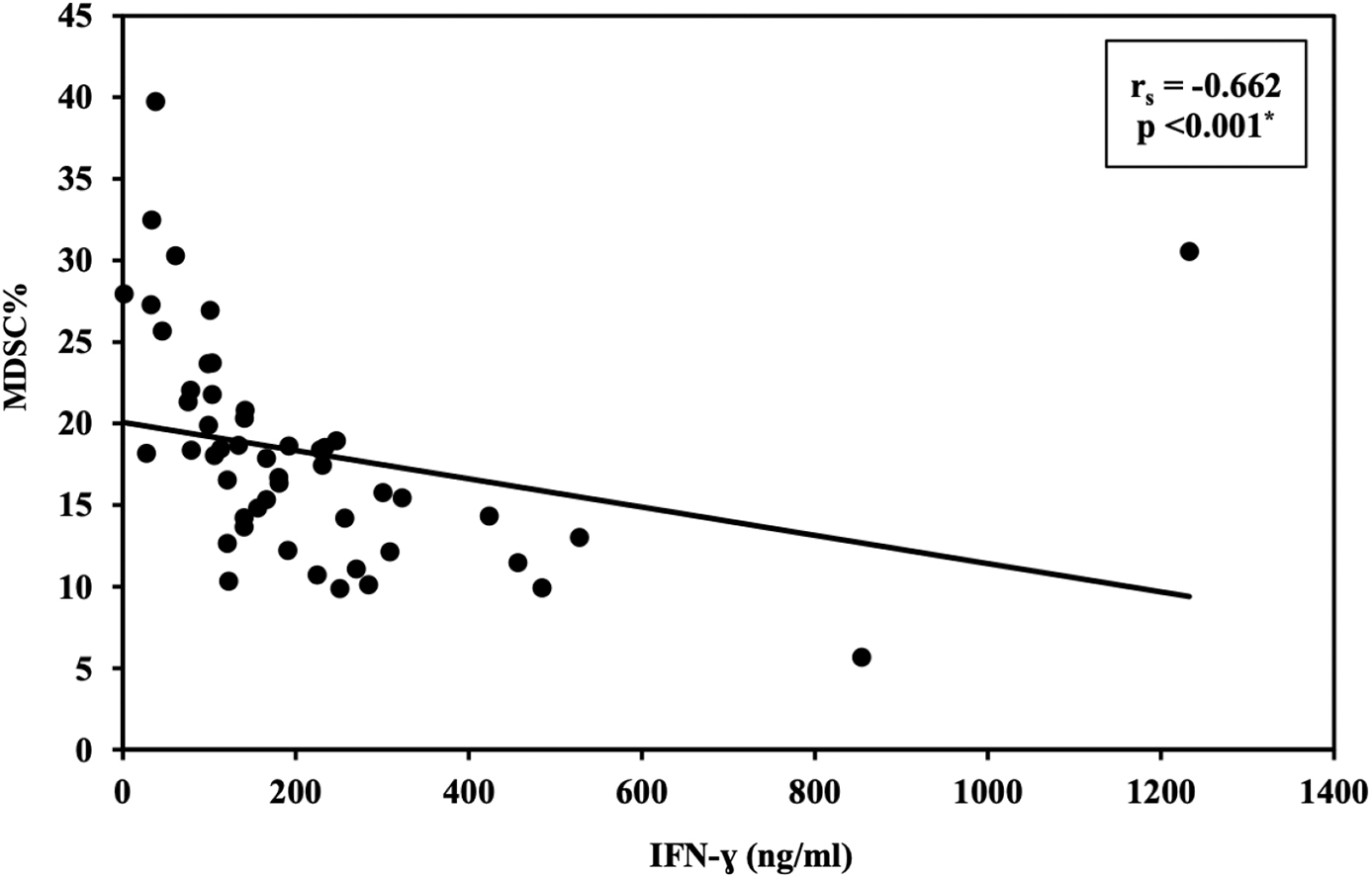
Correlation between MDSC% and IFN-γ concentration in the treated group. *Statistically significant at p ≤ 0.05.
Correlation Between Myeloid-Derived Suppressor Cell % and Interferon-γ Concentration in Each Group
Statistically significant at p ≤ 0.05.
Discussion
CHC infection is associated with different mechanisms that interfere with pathogen recognition and cytokine production, such as reduced population of peripheral blood dendritic cells, impaired production of inflammatory cytokines, and enhanced production of the immunosuppressive cytokines such as interleukin (IL-10) (Crosignani et al, 2016; Sachdeva et al, 2015). The use of DAA therapy is reported to cause a noticeable reduction in inflammatory biomarkers in plasma and liver. However, this reported reduction may not reach the normal levels of such markers, which may be attributed to multiple factors related to the virus itself; its genotype, viral load, and/or host factors, such as age and immune response (Baskic et al, 2017; Carlin et al, 2015; Tarragô et al, 2014).
Accumulating evidence indicated that HCV infection may trigger generation of monocytic myeloid-derived suppressor cells (M-MDSCs) (Pang et al, 2016; Zhai et al, 2017) through induction of monocytes differentiation into M-MDSC (Pang et al, 2016). Increased MDSC frequency was reported to be positively correlated with HCV viral load and decreased CD8 T-cell function (Tacke et al, 2012; Zeng et al, 2014) and also antigen-specific immunosuppression of CD8 T cells by M-MDSC (Zhai et al, 2017). The HCV induction of M-MDSC is thought to be mediated through TLR2/PI3K/AKT/signal transducer and activator of transcription 3 (STAT3) signaling pathway, which induces CD4+Foxp3+ regulatory T cells and inhibits autologous CD4+ T cell activation (Zhai et al, 2017).
Although MDSCs may contribute to immunological balance after infection through controlling excessive inflammatory response arising from such conditions, their expansion may favor pathogen persistence and limit viral elimination, and thus lead to persistent infection (Dai et al, 2015). To investigate the role of MDSCs, we measured the percentage of MDSC population in untreated CHC group, DAAs treated CHC group, and a control group of healthy individuals. Our results revealed a significant increase in MDSC frequency in the untreated chronic HCV patients when compared with the healthy control group.
Moreover, there is a significant decrease in MDSC frequency in the treated CHC patients when compared with the untreated ones. However, the decrease detected in the treated CHC group did not reach the levels noticed in the healthy group. This suggests a proposed role of MDSC in the immune dysregulation reported in chronic HCV infection, and a relation between the viral eradication and sustained viral response attained by DAAs and the partial restoration of MDSC frequency to near-normal levels.
Significant MDSC expansion in chronic HCV infection is thought to be mediated through HCV exosomes. These exosomes-mediated MDSC expansion is directed through viral particles shedding from infected hepatocytes into patients' plasma (Wang et al, 2018). It is reported that MDSC expansion observed in multiple disease models can suppress host immune responses through a significant inhibition in T-cell functions by promoting T reg induction (Ren et al, 2016). MDSC can also cause significant increase in plasma levels of a variety of immunosuppressive mediators, such as arginase 1 (Arg1), inducible nitric oxide synthase, STAT3, and reactive oxygen species (ROS) (Hong et al, 2018; Morceau et al, 2013; van Bragt et al, 2014; Zhang et al, 2019).
The study carried out by Ren and his colleagues to identify the role of MDSCs in regulating T cell function and differentiation in chronic HCV infection revealed a significant increase in the number of MDSCs in comparison with healthy individuals, although the overall number of myeloid cells expressing the surface markers CD33+ and CD11b+ was significantly lower than the number in the healthy ones (Ren et al, 2016). These findings go in agreement with our findings regarding the increase of number of MDSCs in chronic HCV infection in comparison with healthy ones.
Moreover, an experiment done by Tackle and his research team for studying the MDSCs function in chronic HCV infection and its mechanism of action revealed that chronic HCV infection promotes CD33+ MDSC, which suppress the T cell response through ROS, which in turn leads to the persistence and chronicity of HCV infection (Tacke et al, 2012). Another in vitro experiment showed a significant increase of MDSCs in the peripheral blood of untreated CHC patients compared with healthy donors through Arg1 induction and subsequent L-arginine depletion (Cai et al, 2013).
A work done by Pang and his collaborators showed that HCV core protein and polyinosinic:polycytidylic acid (poly I:C) usage as a simulated HCV infection has led to induced differentiation of peripheral blood mononuclear cells (PBMCs) into monocytic-MDSCs. Also, this work revealed an underlying mechanism associated with PI3K signaling pathway (Pang et al, 2016). This again adds up to the agreement with our results that indicate MDSC expansion is present and promoted by HCV infection.
Furthermore, a conclusion reached by another research group led by Zeng states that an increased frequency of MDSCs is present in untreated chronic HCV patients with a positive correlation between that frequency and HCV RNA load and a downregulation of TCR ζ expression on CD8+ T cells, which is inversely correlated with MDSCs frequency in such patients (Zeng et al, 2014).
In addition, in accordance with our results, Hetta and his colleagues reported that the frequency of peripheral MDSCs in Egyptian chronic HCV patients who have developed HCC was significantly increased in comparison with a healthy control group recruited for the study in a model designed for illustrating the role of MDSCs in development of HCV-related HCC in Egyptian patients (Hetta et al, 2019).
Furthermore, Thakuri and his associates pointed out that MDSC promotion and differentiation are affected by HCV infection as they observed a significant increase of MDSC frequency in PBMCs in individuals with chronic HCV infection. They also investigated the role of mRNA expression of runt-related transcription factor-1 (RUNX1) overlapping RNA (RUNXOR) and its target gene RUNX1 to identify the mechanism underlying MDSC expansion, and they concluded that they are overexpressed and consequently can be used as biomarkers for MDSC expansion in chronic HCV infection (Thakuri et al, 2020).
Regarding the decrease in MDSCs frequency upon DAAs treatment in comparison with the untreated CHC patients revealed by our study, a partial retrieval of the immune system regulatory function and reversal of the global dysregulation already reported in case of chronic HCV infection were indicated. The research work pertaining to the effect of DAAs on MDSC population is somewhat lacking, and the knowledge is still piling up to attain needed data to ensure MDSCs as a potential therapeutic target in the treatment of chronic HCV infection.
There is another rising question about the HCC frequency related to chronic HCV infection, and whether this is due to the use of DAAs itself or the already immune dysregulation caused by HCV persistence. Tumino and his colleagues in a small cohort study of 18 HIV/HCV coinfected patients investigated the effect of DAAs on the immune cells related to immune suppression named T regulatory (T reg) cells and MDSCs, and they ended up with interesting results revealing persistence of a high frequency of T reg cells and failure of DAAs to get the MDSCs to the normal levels despite the improved sustained virologic response rates in patients with chronic HCV infection attained by DAAs (Tumino et al, 2017).
Interestingly, Langhans in a letter to The Journal of Hepatology commended the results retrieved by Tumino and his team, and emphasized that the work done by Tumino is a continuation of his work that was done earlier in which he reported the persistence of T reg cells in chronic HCV patients receiving a full DAA treatment protocol and a sustained viral response with HCV eradication (Langhans and Spengler, 2017).
On the contrary, in agreement with the results concluded from this study, Telatin and his collaborators in rather a larger study enrolling 168 patients chronically infected with HCV concluded that the percentages of M-MDSCs are significantly higher when compared with the healthy controls, but in a longitudinal study performed on 11 treated patients in which the percentages of M-MDSCs were evaluated over a time period of 12 and 24 months, they noticed a decrease in the percentages of M-MDSCs in comparable levels with healthy controls (Telatin et al, 2019).
Moreover, a decrease in the frequency of MDSCs and M-MDSCs in chronic HCV-infected patients to a normal level upon DAA treatment on a 24-week period, which is comparable with healthy controls, was reported in a study carried out on 32 chronic HCV patients with an additive observation that the increase in MDSC percentages was accompanied by an increase in CD8+ T cell and NK cell levels (Li et al, 2019), which also goes in accordance with our findings.
Concerning IFN-γ levels, we assessed the levels among the three groups enrolled in this study, which revealed a statistically significant difference (p < 0.001*) between study groups. The treated CHC group showed significantly higher IFN-γ levels compared with untreated group, which may represent a clue to the partial restoration of NK cells activity after DAA treatment. Moreover, there was a significant negative correlation between MDSC frequency and IFN-γ concentration among the group of treated HCV patients (p < 0.001*).
In a research study carried out on chronic HCV genotype 4-infected Egyptian patients by Nabeel et al, serum IFN-γ and IL-10 levels were assessed, and it was revealed that successful DAA-mediated viral eradication induced significant changes in IFN-γ and IL-10 levels (Nabeel et al, 2022), which was in agreement with our results.
To the best of our knowledge, in addition to the shortage of knowledge on the role of MDSCs in chronic HCV and its response to DAAs, there is no published study on that role in the Egyptian patients and the prevailing HCV genotype 4, which is of great importance to elucidate because of the burden the HCV creates on the economic and health status of Egypt, and the National adoption of mass treatment program, which has an impact on the chronic HCV-infected patients. Moreover, the HCC development, which is a major and life-threatening complication of chronic HCV infection, can be related to MDSC accumulation and the immune dysregulation caused by such accumulation, which may play a role in the persistent inflammatory state in liver tissue that is thought to play a role in HCC development.
In conclusion, future studies applied as longitudinal prospective cohort on large number of patients with follow-up before and after DAA treatment would be a valuable addition to the already available knowledge to further reveal the clinical significance of elevated MDSC frequency in CHC patients and open the way to future MDSC targeting as a promising therapeutic potential through immune modulation in chronic HCV cases.
Footnotes
Authors' Contributions
B.A. contributed to review and editing (equal); writing—review and editing (equal); writing—original draft (equal); methodology (supporting). M.A. assisted with conceptualization (supporting); methodology (supporting). A.K.A., W.E., and H.M. provided methodology (supporting). B.E. contributed to conceptualization (lead); writing—original draft (lead); review and editing (equal); formal analysis (lead); writing—review and editing (equal); and methodology (lead).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.