
Abstract
Monocytes in hepatitis C virus (HCV) infection play a critical role in chronic liver inflammation and fibrosis. We studied circulating monocytes and monocyte receptors in patients with HCV infection who were naive to treatment and those who received direct acting antiviral therapy and achieved sustained virological response. CD64+ CCR2+ (M1-like) and CD206+ CD163+ CX3CR1+ (M2-like) monocyte numbers and receptor expression were evaluated by flow cytometry. Higher expression of the monocyte chemokine receptor CCR2 predicted the severity of liver fibrosis, independent of successful treatment and viral clearance (R 2 = 0.235, p = 0.002), whereas monocyte CX3CR1 expression was lower in both treated and untreated patients compared with controls (p = 0.011). The expression of the scavenger receptor CD163 was lower in patients with successful treatment (p = 0.005), supporting its role as a marker of treatment response. CD64+ CCR2+ (M1-like) and CD206+ CD163+ CX3CR1+ (M2-like) monocyte numbers were not altered with fibrosis progression or treatment response. Our findings reflect the diverse functions of monocytes in liver inflammation, fibrosis, and therapy. However, HCV clearance did not lead to complete monocyte reconstitution. Targeting monocytes and their chemokine receptors bears therapeutic potential to reduce liver fibrosis and improve disease outcome.
Introduction
Infection of the liver by hepatitis C virus (HCV) causes chronic inflammatory damage and death of the parenchymal cells. This results in progressive replacement by extracellular matrix (ECM) proteins, in a process of hepatic fibrosis. Ultimately cirrhosis ensues and liver transplantation becomes lifesaving (Pellicoro et al., 2014). HCV infection was an exceedingly challenging problem until effective direct acting antiviral (DAA) agents were developed. Despite the excellent results with sofosbuvir-based DAA therapy in viral clearance, patients with bridging fibrosis and cirrhosis are still at risk of developing liver-related complications and mortality, even after achieving a sustained virological response (Nahon and Ganne-Carrié, 2019).
When the liver is chronically inflamed, circulating monocytes infiltrate the liver in increased numbers and differentiate into macrophages (Italiani and Boraschi, 2014). Monocytes express the chemokine receptors, CCR2 and CX3CR1, implicated in the pathogenesis of liver fibrosis (Tacke and Zimmermann, 2014). CCR2 and its ligand; monocyte-chemoattractant protein 1 (MCP-1/CCL2) were found to be upregulated in the fibrotic liver, with an accumulation of inflammation-polarized monocyte-derived macrophages that activate hepatic stellate cells, the source of ECM proteins (Karlmark et al., 2009; Zimmermann et al., 2010). CX3CR1, the chemokine receptor for fractalkine (CX3CL1), represents an anti-inflammatory differentiation signal, as macrophages polarized to anti-inflammatory activation in the liver are derived from monocytes expressing CX3CR1 (Ancuta et al., 2003).
Some authors have identified CX3CR1 gene as a susceptibility gene for hepatic fibrosis in HCV infection, whereas others have associated the upregulation of CX3CR1 and fractalkine with chronic liver damage (Efsen et al., 2002; Wasmuth et al., 2008). The monocyte macrophage lineage cells also express a variety of scavenger receptors, including the haptoglobin–hemoglobin scavenger receptor (CD163) and the mannose receptor (CD206) (Porcheray et al., 2005). Upon anti-inflammatory activation, both receptors were found to be released in soluble form in substantial levels, which correlated with liver fibrosis in patients with chronic hepatitis C (Kazankov et al., 2014; Saha et al., 2019).
Heterogeneity among monocytes, the circulating precursors of liver macrophages, is well recognized. Monocytes and macrophages are highly plastic cells, with a remarkable ability to change their physiology and phenotype in response to external signals (Porcheray et al., 2005). Macrophages have been described according to the differential expression of the chemokine receptors CCR2 and CX3CR1 secondary to proinflammatory or anti-inflammatory activation into M1 or M2, respectively (Mantovani et al., 2004). M1 macrophages preferentially express the high-affinity IgG Fcγ receptor I (CD64), whereas the scavenger (CD163) and mannose (CD206) receptors are highly expressed by M2 macrophages (Hristodorov et al., 2015).
Since some features of the receptor repertoire are conserved between circulating monocytes and tissue macrophages (Martinez et al., 2013), thus we used M1 and M2 markers as a method of characterizing monocyte subpopulations before they differentiate into macrophages. Cells that express M1 phenotype markers (CD64 and CCR2) and M2 phenotype markers (CD206, CD163, and CX3CR1) were used to identify the cells with an M1 or M2 profile (Fadini et al., 2014) to understand the diverse and sometimes contrasting functions of monocytes and macrophages in HCV-induced liver inflammation, fibrosis, and direct antiviral therapy.
Materials and Methods
Patients
A total of 43 patients with HCV infection consecutively participated in this prospective study. All patients were recruited from the Cairo University Center for Hepatic Fibrosis. The study included 23 antiviral treatment-naive patients and 20 patients who had cured HCV infection after DAA therapy. Patients were treated with sofosbuvir (nucleotide analog NS5B polymerase inhibitor) and daclatasvir (NS5A inhibitor) for a 12-week regimen if the liver fibrosis grade was F0–F3 and a 24-week regimen if the liver fibrosis grade was F4 (European Association for The Study of The Liver, 2018).
Patients were defined to have achieved sustained virological response (SVR) if HCV RNA was undetectable, 12 or 24 weeks after treatment completion. Exclusion criteria included ascites, coinfection with other hepatitis viruses or human immunodeficiency virus, and other liver diseases. Ten age- and sex-matched (6 men and 4 women; median age, 45 years), healthy individuals provided control samples. The study was approved by the departmental ethical committee in Cairo University. An informed written consent was obtained from all study participants.
Assessment of liver fibrosis
Liver fibrosis evaluation was performed using transient elastography with FibroScan. The measurements expressed in kiloPascals (kPa) were regarded as the liver stiffness measurement for each participant. The score was converted to the METAVIR staging system (F0–F4) (Castéra et al., 2005). Liver fibrosis was also assessed by validated noninvasive methods on serum biomarkers. Platelet counts, liver-associated enzymes including aspartate and alanine aminotransferases (AST and ALT) were obtained and noninvasive estimators of fibrosis were determined, including the AST to Platelet Ratio Index (APRI) (Wai et al., 2003) and the Fibrosis-4 (FIB-4) Index (Sterling et al., 2006). APRI was calculated using the following equation: 100 × [AST (U/L)/upper limit of normal AST values (U/L)]/[Platelet (109/L)] and Fib-4 was calculated using the following equation: [age × AST (U/L)]/[Platelet (109/L) × √ALT (U/L)].
Flow cytometry
Whole blood samples were collected in EDTA tubes from each patient and control. Each sample was analyzed for complete blood counts. For the identification and quantification of monocyte phenotypes, we performed flow cytometry. M1-like phenotype was characterized using fluorescein isothiocyanate (FITC)-conjugated anti-CD64 (BD Biosciences) and phycoerythrin (PE)-conjugated anti-CCR2 (Miltenyi Biotec) antibodies. In a separate tube, M2-like phenotype was identified by FITC-conjugated anti-CD206, allophycocyanin (APC)-conjugated anti-CX3CR1, with or without PE-conjugated anti-CD163 antibodies (Miltenyi Biotec). Washed blood samples were immunostained for 10 min at 4°C by using the appropriate antibodies followed by erythrocyte lysis.
All samples were analyzed using a Becton Dickinson FACSCanto and the BD FACS Diva analysis software, evaluating a total of 5 × 104 cells. Monocytes were first gated in a forward/sideward scatter dot-plot according to their size and granularity (Fig. 1). Monocytes expressing CD64 and CCR2 characterized an M1-like phenotype. Monocytes showing M2-like phenotype were defined based on the co-expression of CD206 and CD163 followed by gating for CX3CR1 expression within the double positive population or by the co-expression of CD206 and CX3CR1 only. For each of the gated positive population, we determined the mean fluorescence intensity for the respective monocyte markers. Unstained control tubes were performed to assist with gating.

Monocytes were first gated in a forward scatter/sideward scatter (FSC/SSC) dot-plot according to their size and granularity
Statistical analyses
Differences between groups were assessed applying Kruskal–Wallis and Mann–Whitney U for nonparametric tests and one-way analysis of variance and Student's t-test for parametric tests. Bivariate Spearman's rank-correlation was used to measure the relationship between two variables. A p-value <0.05 was considered as statistically significant. Using liver stiffness measurement as a quadratic-transformed dependent variable, regression analysis was performed for each independent variable while controlling for patient treatment status (treated or untreated). Data were analyzed using IBM SPSS Statistics version 20. The results were graphically represented using Graph Pad Prism version 5.
Results
Treatment-naive HCV-infected individuals and patients treated with DAA therapy and achieving viral clearance were evaluated (Table 1). Patients with HCV infection showed variable severity of liver fibrosis. Thirty-nine percent of patients who had not received anti-HCV treatment and 55% of SVR achieving patients had significant liver fibrosis or cirrhosis (METAVIR stage F2–F4). Higher values of liver stiffness measurements by FibroScan were associated with increasing Fib-4 scores (R = 0.512, p = 0.001), increasing AST/ALT ratio (R = 0.481, p = 0.001), but not with increasing APRI scores (R = 0.267, p = 0.087) (Data not shown). The aminotransferase enzyme levels were significantly decreased in patients with an SVR than treatment-naive patients.
Clinical and Laboratory Characteristics of Hepatitis C Virus Patients
Data are presented as median and 25th–75th percentiles or number (%).
Significant p < 0.05.
ALT, alanine aminotransferase; APRI, aspartate aminotransferase to platelet ratio index; AST, aspartate aminotransferase; CAP, controlled attenuation parameter; FIB-4, Fibrosis-4; HCV, hepatitis C virus; kPa, kilopascals; N/A, not applicable; SVR, sustained virological response.
Monocyte M1-like and M2-like phenotypes in treatment-naive HCV patients and patients achieving SVR
The monocyte phenotypes were evaluated in healthy controls, in treatment-naive patients and patients achieving SVR with DAA therapy. The absolute numbers of monocyte subpopulations were estimated from the flow cytometric frequencies and the total leukocyte counts from the hematology analyzer. The total monocyte numbers were comparable in both treatment-naive and SVR patients compared with controls (p = 0.069) (Fig. 2). When the absolute numbers of CD64+ CCR2+ (M1-like) and CD206+ CX3CR1+ (±CD163+) (M2-like) phenotypes were analyzed, there were no considerable alterations in treatment-naive patients and patients achieving SVR compared with controls. The frequency of the M2-like phenotype was small relative to the M1-like phenotype in patients and controls.
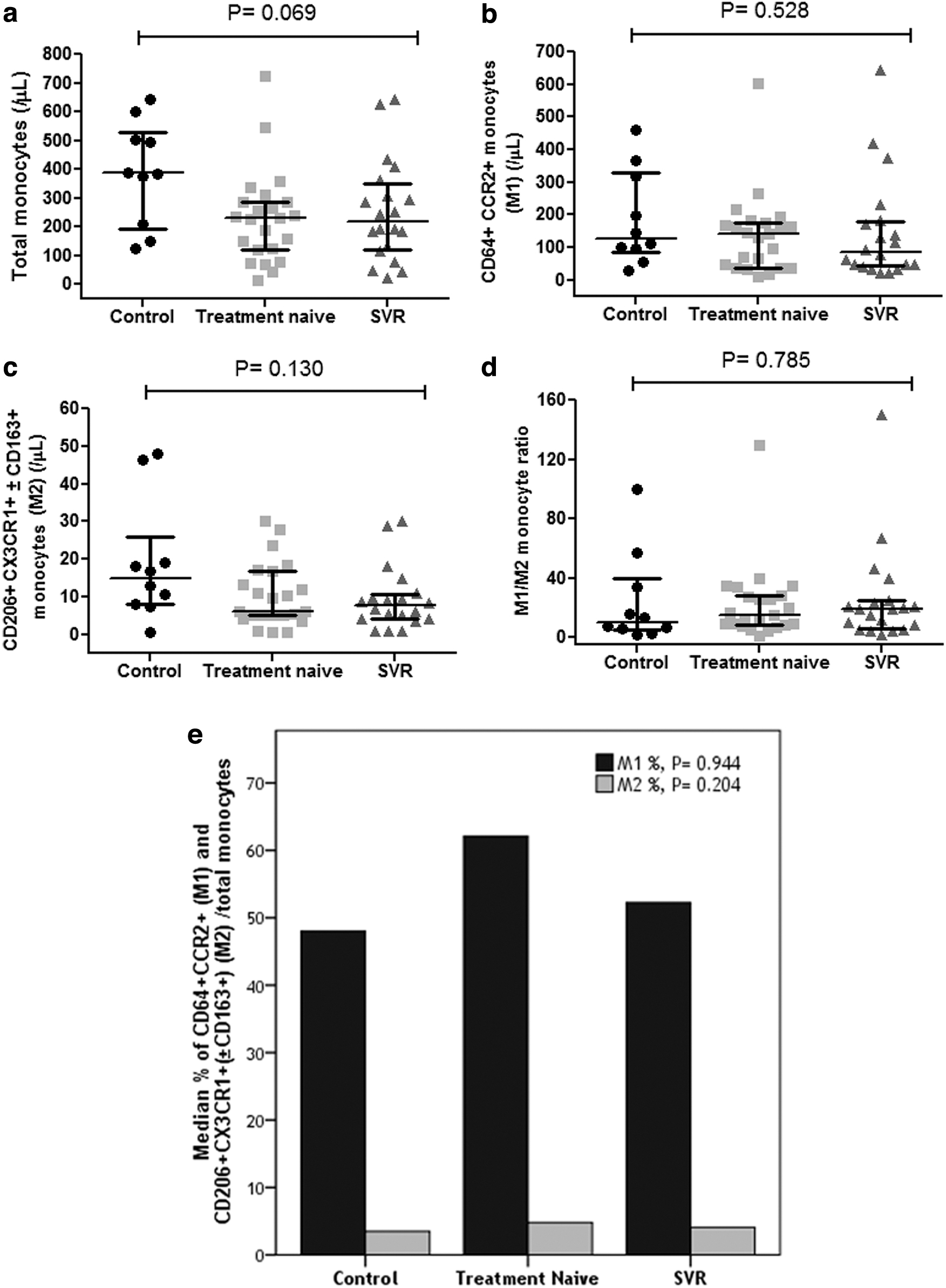
The total monocyte numbers were comparable in both treatment-naive and SVR patients compared with controls
Surface receptor expression of monocytes in treatment-naive HCV patients and patients achieving SVR
We examined the expression of the surface receptors related to the M1-like phenotype; CCR2 and IgG FcγRI (CD64) and those related to the M2-like phenotype; CX3CR1, mannose (CD206) and scavenger (CD163) receptors (Fig. 3). For each cell, the mean fluorescence intensities of each staining were measured and analyzed. Treatment-naive and SVR achieving patients displayed no difference in the expression of the receptors related to the M1-like phenotype compared with controls. By contrast, differences in expression of receptors related to the M2-like phenotype were identified. Lower expression of CX3CR1 was detected in both treatment-naive and SVR achieving patients compared with controls (p = 0.011). The only difference in the expression of monocyte receptors between treatment-naive and SVR achieving patients was observed for CD163. Lower expression was observed in patients achieving SVR compared with treatment-naive patients (p = 0.005).
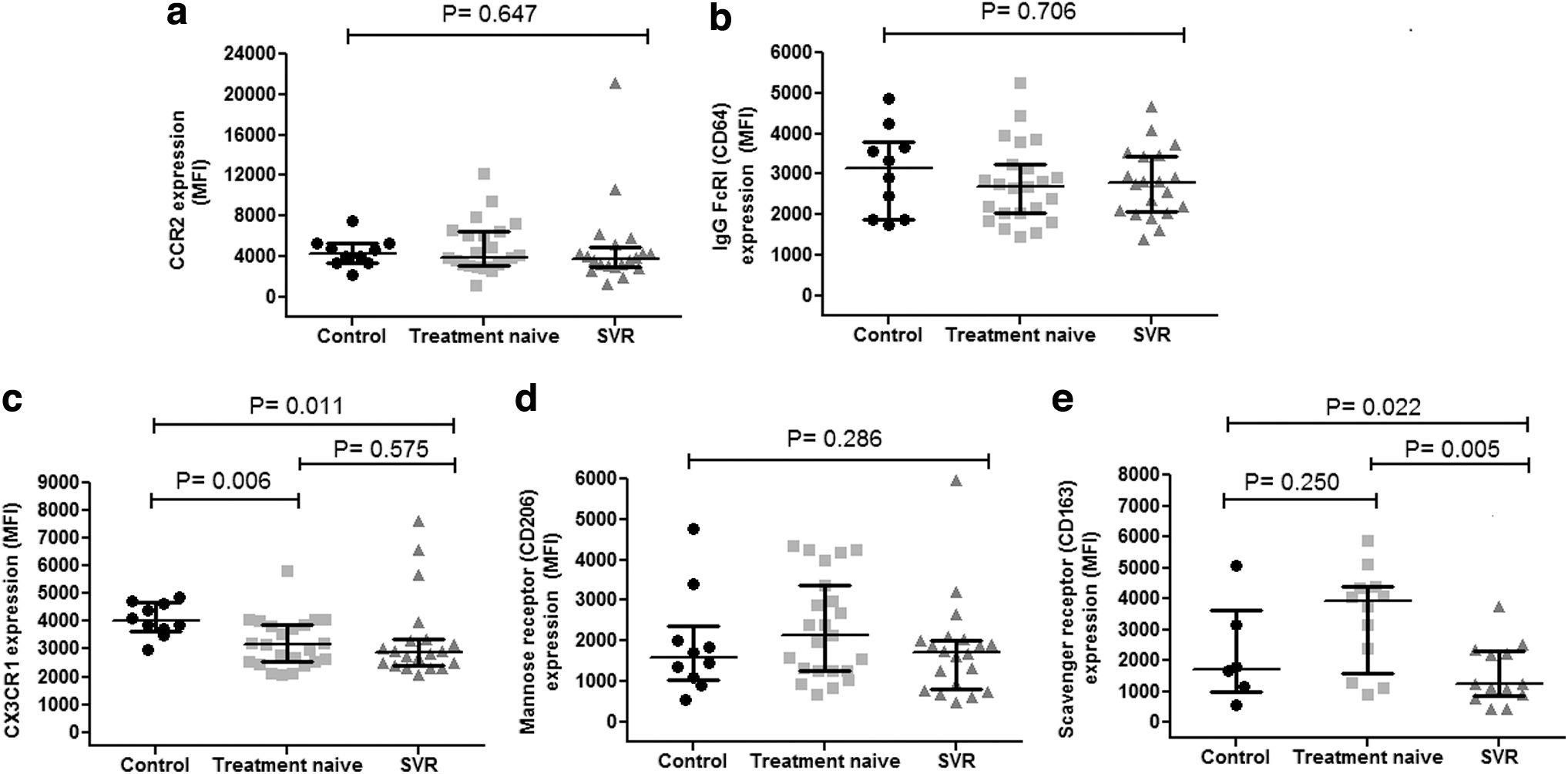
The expression of the surface receptors related to the M1-like phenotype;
When studying monocyte receptor expression, the only significant correlation in normal controls was a strong correlation between IgG FcγRI (CD64) and the mannose receptor (CD206) (R = 0.794, p = 0.006). This positive correlation was further observed in treatment-naive patients (R = 0.430, p = 0.041), but not in treated SVR achieving patients (R = −0.038, p = 0.875) (Data not shown). In treatment-naive patients, the expression of the chemokine receptors, CCR2 and CX3CR1 correlated weakly (R = 0.417, p = 0.048), whereas in SVR achieving patients the expression of CD206 and CD163 correlated moderately (R = 0.588, p = 0.035) (Data not shown).
Monocyte CCR2 expression predicts progression of severity of liver fibrosis
We explored the relationship between the severity of liver fibrosis in all HCV patients (n = 43) and monocyte subpopulations and surface receptor expression. Increasing CCR2 expression significantly predicted the severity of liver fibrosis, estimated by the liver stiffness measurement using transient elastography, in kPa, independent of successful treatment by DAA and viral clearance (Table 2). On the contrary, when examined for the prediction of liver fibrosis severity, the expression of IgG FcγRI (CD64), CX3CR1, mannose (CD206), and scavenger (CD163) receptors, did not show a detectable effect. Similarly, the numbers of M1-like and M2-like subpopulations were not associated with an increasing degree of fibrosis.
Association of Monocyte Phenotypes and Surface Receptors with Liver Stiffness Measurements While Controlled for Patient Treatment
Significant p < 0.05.
MFI, mean fluorescence intensity.
Correlation between monocyte subpopulations and receptors with biochemical liver parameters
When assessed for correlation with the degree of liver injury measured as serum ALT levels, the expression of CD163 correlated significantly with higher ALT enzyme levels (R = 0.530, p = 0.006) and lower AST/ALT ratios (R = −0.456, p = 0.022) (Table 3). The expression of the mannose receptor (CD206) did not follow a similar pattern of correlation with ALT levels and AST/ALT ratio. The albumin concentration, a marker of the synthetic function of the liver correlated inversely with M1-like CD64+ CCR2+ monocytes (R = −0.371, p = 0.014). The expression of monocyte receptors did not show an association with decreasing serum albumin concentration or decreasing platelet count, an indicator of advanced disease. We found no correlation between M1- or M2-like cells or receptors with the HCV viral load in treatment-naive patients.
Correlation Between Monocyte Subpopulations and Surface Receptors with Biochemical Liver Markers
Significant p < 0.05.
Discussion
Monocytes circulate constantly to and from the healthy liver but populate the liver in massive numbers in the setting of chronic inflammation. One central feature of chronic liver inflammation is the polarization of monocytes and macrophages (Tacke and Zimmermann, 2014). We characterized blood monocyte subpopulations and surface receptors before they differentiate into liver macrophages in patients with HCV liver disease and in treated patients achieving SVR after DAA therapy. We found that increasing expression of CCR2 predicted the severity of liver fibrosis estimated by the liver stiffness measurement. This was independent of successful treatment and viral clearance.
Although the numbers of CCR2 and CD64 expressing monocytes were not altered, increasing CCR2 expression with fibrosis progression suggested a potential role for CCR2 in liver fibrosis. Experimental evidence has shown that when the liver is injured, CCR2 critically controls monocyte entry into the liver, primarily by promoting the mobilization of monocytes from the bone marrow into the circulation (Karlmark et al., 2009). In chronic liver damage, intrahepatic CCR2 expressing monocytes develop preferentially into inducible nitric oxide synthase producing M1 macrophages that can activate hepatic stellate cells in a TGF-β-dependent mechanism to transdifferentiate into myofibroblasts that secrete fibrillar collagens I and III and α-smooth muscle actin, resulting in fibrosis (Karlmark et al., 2009).
M1 macrophages in the liver release proinflammatory cytokines such as interleukin (IL)-1β, tumor necrosis factor-alpha (TNF-α), and IL-6 that cause further hepatocyte inflammation and apoptosis. Cytokines, especially IL-1, reduce albumin RNA expression and synthesis in the liver during inflammation (Moshage et al., 1987). We observed that CD64+ CCR2+ M1-like cells correlated negatively with serum albumin levels, and because albumin is a marker of the synthetic function of the liver, this suggests that CD64+ CCR2+ cells have prognostic importance.
In contrast to CCR2, the expression of monocyte CX3CR1 was not associated with liver fibrosis severity. Although the numbers of CX3CR1 expressing cells (M2-like cells) were unaltered, lower expression of CX3CR1 was detected in both naive to treatment and SVR achieving patients compared with controls. Of importance, an opposing regulation of CX3CR1 and its ligand has been described in patients with fibrosis and cirrhosis (Karlmark et al., 2010). As the ligand for CX3CR1, fractalkine (CX3CL1) is induced upon liver injury in hepatocytes and hepatic stellate cells, this may explain the reduced expression of CX3CR1 by monocytes. Experimental data have revealed that monocyte-derived macrophages deficient in CX3CR1 undergo increased cell death, because the primary functions of CX3CR1 in the injured liver promote the survival of infiltrating monocytes by activating antiapoptotic bcl-2 expression (Karlmark et al., 2010).
Increased cell death provides a profound signal for the infiltration of monocytes that develop into M1 macrophages. By this means, the inflammatory response is perpetuated resulting in enhanced liver fibrosis. It was also observed that downregulating CX3CR1 in monocytes, upregulates CCR2 expression through p38 MAP kinase signaling (Montague et al., 2018). Our data show that in the setting of downregulated CX3CR1 in HCV, increasing CCR2 expression in monocytes was predictive of the severity of fibrosis. In our patients, reduced CX3CR1 expression by monocytes developing into hepatic macrophages may result in unrestricted inflammation and fibrosis progression within the injured liver.
Fibrosis is an abnormal wound healing response to chronic inflammation, leading to scarring of the liver. It is important to note that liver fibrosis is not one directional, but regression from fibrosis could be observed in patients undergoing successful treatment of their underlying disease (Campana and Iredale, 2017). If the chronic damage to the liver terminates, the inflammatory pathways become deactivated, whereas regenerative pathways of macrophages dominate (Tacke and Trautwein, 2015). Viral clearance is one measure to stimulate regression of liver fibrosis. With the development of DAAs, programs for screening and diagnosis of HCV patients were established (Soliman et al., 2019).
DAAs have dramatically changed the course of chronic hepatitis C. Sofosbuvir in combination with other DAAs provide high SVR rates for chronic HCV patients, including those with advanced liver disease (Laursen et al., 2020). In our patients, it seems evident that successful antiviral therapy has valuable effects on liver-related parameters. However, our results indicate that HCV clearance does not lead to complete immunological reconstitution. We found that CX3CR1 was reduced in both treated and untreated patients, whereas CCR2 was associated with liver fibrosis independent of treatment. Thus, a combination of anti-inflammatory and antifibrotic therapies in addition to etiology-specific treatment will be most effective.
The reprogramming of monocyte-derived macrophage subpopulations toward orchestrating regenerative rather than inflammatory response is a promising approach. CCR2 expression by monocyte-derived macrophages represents a target for the treatment of liver fibrosis. Treatment with the dual CCR2/CCR5 inhibitor, cenicriviroc, has proven effective in reducing liver fibrosis in experimental models and patients with fibrosis (Sherman et al., 2019). Because of the functional significance of CX3CR1 expression for the regulation of liver inflammation and fibrosis, pharmacological augmentation of this pathway may represent another potential antifibrotic strategy for patients with chronic liver inflammation (Esfen et al., 2002).
When monocyte receptors were assessed for correlation with the degree of liver injury by serum ALT levels, the expression of the scavenger receptor CD163 correlated significantly with increasing enzyme levels and decreasing AST/ALT ratio. In line with its role as a marker of ongoing inflammation, monocyte CD163 levels were lower in patients with successful sofosbuvir-based DAA therapy. This was the only difference observed between treatment-naive patients and patients with successful therapy, confirming CD163 as a reliable biomarker of response.
It is important to note that this was irrespective of disease severity as 55% of SVR achieving patients and 39% of patients who had not received treatment had significant liver fibrosis or cirrhosis. It was reported that the soluble form of CD163 dynamically declined with successful therapy irrespective of treatment regimen and the decline was not an effect of the specific antiviral treatment but related to HCV clearance (Laursen et al., 2018a). After oral DAA-therapy, the decline was rapid and sustained after treatment ending, signifying macrophage deactivation upon HCV clearance.
Similar to soluble CD163, soluble CD206 has gained interest for its potential as a biomarker of antiviral treatment (Laursen et al., 2018b). We found that monocytic CD206 was not different between treated and untreated patients, despite that CD206 correlated moderately with CD163 in SVR achieving patients. CD206 did not follow a similar pattern to CD163, correlating with increasing ALT levels and decreasing AST/ALT ratio. Differences in expression and regulatory mechanisms for CD163 and CD206 receptors may explain the dissimilarities in their prognostic utility. CD163 and CD206 display mutually exclusive induction patterns. IL-4 upregulates CD206 expression and suppresses that of CD163, whereas IL-10 induces the overexpression of CD163 and excludes other activation pathways of macrophages (Procheray et al., 2005). Low IL-10 levels were found to be associated with SVR (Yoneda et al., 2011), in line with reduced monocyte CD163 expression in viral response to HCV treatment.
Conclusion
Successful antiviral therapy has valuable effects on liver-related parameters. However, we found that CX3CR1 was reduced in both treated and untreated patients, whereas CCR2 was associated with liver fibrosis independent of treatment. Targeting monocytes and monocyte-derived macrophages driving fibrosis progression holds promising opportunities for therapy, even after viral clearance. Future studies will determine when and where the reprogramming of monocyte-derived macrophages may be incorporated to treat patients with chronic liver disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Cairo University Center for Hepatic fibrosis (CUCHF) was funded by the Egyptian Science and Technology Development Fund (STDF; ID 5274, Ethical approval N-53-2014).