
Abstract
FcγR is expressed by many immune cells and plays an important role in the immune response to hepatitis B virus (HBV) infection. CD32 belongs to the FcγR family. This study aimed to observe changes in CD32 expression by CD4+ T and CD8+ T lymphocytes in chronic HBV infection patients and evaluate the clinical utility of CD4+ T and CD8+ T CD32 expression to assess the severity of liver injury in chronic HBV-infected patients. A total of 68 chronic HBV patients and 40 healthy individuals were recruited, and the median fluorescence intensity (MFI) of CD32 expression on CD4+ T, CD8+ T lymphocytes was measured using flow cytometry and the CD4+ T, CD8+ T CD32 index was calculated. The reactivity of the healthy individual lymphocytes to mixed patients' plasma containing HBV was observed. Finally, the correlation between CD4+ T, CD8+ T lymphocytes CD32 MFI and liver function indicator levels was analyzed. The CD4+ T, CD8+ T CD32 MFI and index were significantly elevated in HBV patient groups than in normal control group (p < 0.001, for all). Furthermore, the CD32 MFI of healthy persons' CD4+ T and CD8+ T lymphocytes were remarkably increased when stimulated with mixed patients' plasma containing high HBV copies (p < 0.001; P < 0.001). More importantly, in HBV patients, there was a significant positive correlation between CD4+ T, CD8+ T CD32 MFI and the level of serum aspartate aminotransferase (p < 0.05, p < 0.05). In conclusion, the increased expression of CD32 on CD4+ T and CD8+ T lymphocytes might be potential promising biomarkers for the severity of liver function impairment in chronic HBV patients.
Introduction
Hepatitis B is a global public health concern caused by the hepatitis B virus (HBV), which infects >240 million people worldwide and causes >700,000 deaths per year (Tang et al., 2018). China has a high prevalence of HBV infection. Although the incidence of acute hepatitis B decreased from 2013 to 2020, the incidence of chronic hepatitis B has increased annually in China (Miao et al., 2021). Since patients with chronic hepatitis B are more likely to develop HBV-related cirrhosis, liver failure, and hepatocellular carcinoma (Croagh and Lubel, 2014; Yuen et al., 2018), it is important to clarify the precise mechanism that determines the disease outcomes, especially the mechanism of the host antivirus immune response. Multiple studies have reported that the impairment of cellular immunity is believed to be a key contributing factor (Guidotti et al., 2015; Li et al., 2014); therefore, the identification of immunological markers associated with the clinical outcomes is important to improve the clinical management of hepatitis B.
It has been well established that receptors for the Fc portion of IgG (FcγRs) have been the focus of extensive research due to their key role linking innate and humoral immunity. CD32 belongs to human FcγRII family, is a low-affinity Fc receptor of immunoglobulin IgG, which is commonly expressed on the surface of monocytes, macrophages, and eosinophils (Anania et al., 2019), as well as natural killer (NK) cells, B lymphocytes (Bruhns and Teillaud, 2016; Van Den Herik-Oudijk et al., 1994), and activated T lymphocytes (Engelhardt et al., 1995; Holgado et al., 2018). Several studies have reported that FcγRs, including CD32, play an important role in the healthy immune response to infectious disease, inflammation, autoimmunity, and cancer (Junqueira et al., 2022; Qi et al., 2019; Vogelpoel et al., 2015).
In 2018, it was demonstrated that CD32 expression was a marker of CD4+ T cell activation in human immunodeficiency virus (HIV)+ individuals and raised questions regarding the immune resting status of CD32+ cells harboring HIV-1 proviruses (Badia et al., 2018). In this study, we investigated the changes in the characteristics of CD32 expression on CD4+ T and CD8+ T lymphocytes in patients with chronic HBV infection. Furthermore, we observed the reactivity of healthy individuals' CD4+ T and CD8+ T lymphocytes to mixed patients' plasma containing HBV. Finally, we evaluated the clinical utility of CD4+ T and CD8+ T CD32 expression to assess the degree of liver function impairment in chronic HBV-infected patients.
Materials and Methods
Subjects
A total of 68 patients with chronic HBV infection were recruited at the Second People's Hospital of Hefei from January to December 2021. The diagnosis was based on clinical and laboratory findings according to the Guideline of Prevention and Treatment for Chronic Hepatitis B (2015 version) (Hou et al., 2017). None of the patients with HBV infection had received antiviral treatment within 6 months before this study's enrollment and divided into liver function normal (HBV-LFN) group and liver function abnormal (HBV-LFAN) group according to HBsAg, HBeAg, serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), and HBV DNA levels.
Acute hepatitis B and infection with other hepatitis virus or HIV, drug-induced liver injury, autoimmune hepatitis, alcoholic hepatitis, and cirrhosis was excluded. A total of 40 healthy individuals, who came for physical checkups with normal results were recruited as the normal control group. The characteristics of the subjects in the three groups are summarized in Table 1. The study protocol was approved by the ethics committee of the Second People's Hospital of Hefei.
Clinical Features of the Subjects in the Three Groups [Median (Interquartile Range)]
Kruskal–Wallis test with Dunnett's post hoc tests were used to compare the differences between groups.
p < 0.001, ** p < 0.01, compared with NC group; △△△ P < 0.001, compared with HBV-LFN group.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBIL, direct bilirubin; HBV-LFAN, HBV patients with liver function abnormal; HBV-LFN, HBV patients with liver function normal; NC, normal control; ND, not determined; TBIL, total bilirubin.
Clinical parameter analysis
Every subject in our study took routine laboratory tests, including serum biochemical indices of liver function, HBV serological markers, blood routine tests, and serum HBV DNA. Liver function biochemical indices, including ALT, AST, total bilirubin (TBIL), and direct bilirubin (DBIL), were measured using an automatic biochemical analyzer (AU5800; Beckman Coulter). Normalized serum concentrations of ALT, AST, TBIL, and DBIL were 7–40 U/L, 13–35 U/L, 2–20.4 μmol/L, and 0–6.8 μmol/L. The HBV serological markers, including HBsAg, HBsAb, HBeAg, anti-HBe, and anti-HBc, were determined using an automatic chemiluminescence immune analyzer (LiCA500, Beijing Chemclin). The absolute number of lymphocytes was detected using an automated blood cell analyzer (BC6900; Mindray). The serum HBV DNA loads were determined by real-time polymerase chain reaction (PCR) using CFX96 quantitative PCR instrument (Bio-Rad) with a low detection limit of 15 IU/mL.
Mixed plasma preparation
The plasma samples of 20 healthy individuals were collected and mixed as allogeneic plasma. The plasma samples of 20 chronic HBV infections (HBsAg+, HBV DNA 15–500 IU/mL) were collected and mixed as low virus copies plasma, 20 plasma samples of HBV patients (HBsAg+, HBV DNA >108 IU/mL) were as high virus copies plasma, respectively. Plasma with hemolysis, hyperlipidemia, and high bilirubin were excluded.
PBMCs isolation, stimulation, and incubation
Peripheral blood mononuclear cells (PBMCs) were isolated from 2 mL ethylenediaminetetraacetic acid (EDTA) anticoagulant combined with the peripheral blood samples of healthy individuals through density gradient centrifugation using Ficoll-Paque (TBD Science, Tianjing, China). The samples were resuspended in RPMI 1640 and the cell concentration was adjusted to 1 × 106/mL. The cells were stimulated with 10% auto plasma, mixed allogeneic plasma, mixed low virus copies, and high virus copies plasma, respectively. Finally, the PBMCs were incubated at 37°C 5% CO2 for 24 h, and the cells were collected for flow cytometric analysis.
Flow cytometric analysis
EDTA anticoagulant peripheral blood samples (50 μL) of the subjects or cultured PBMCs (100 μL) were stained with anti-CD3-PerCP (Biolegend), anti-CD8-FITC (Biolegend), anti-CD4-APC (Biolegend), and anti-CD32 PE (Biolegend) for 20 min at room temperature in the dark. Red blood cells in the peripheral whole blood samples were lysed with 1 mL lysis solution (BD Biosciences) for 10 min at room temperature in the dark. After lysing the red blood cells, the cell suspension was centrifuged for 5 min at 1,500 rpm. Finally, the cell pellets were washed with cold phosphate buffer saline and subjected to flow cytometry. Cultured PBMCs were detected directly after staining and washing. Acquisitions were performed using CellQuest Software by FACS Calibur (BD Bioscience), and data were analyzed using FlowJo Software. The expression of CD32 on CD4+ T and CD8+ T lymphocytes was presented as the median fluorescence intensity (MFI).
Calculation of the CD32 index and lymphocyte absolute numbers
Several articles have reported the neutrophil CD64 index calculation method (Huang et al., 2022; Liu et al., 2020). In reference to the neutrophil CD64 index calculation method, the CD32 index was calculated using the following formulas: neutrophil CD32 index = (neutrophil CD32 MFI/lymphocyte CD32 MFI)/(monocyte CD32 MFI/neutrophil CD32 MFI). Th cell CD32 index = (CD4+ T CD32 MFI/lymphocyte CD32 MFI)/(monocyte CD32 MFI/CD4+ T CD32 MFI). CD8+ T cell CD32 index = (CD8+ T CD32 MFI/lymphocyte CD32 MFI)/(monocyte CD32 MFI/CD8+ T CD32 MFI). The absolute numbers of T, CD4+ T, and CD8+ T cells were calculated using the following formula: lymphocyte absolute numbers × the proportions of T, CD4+ T, and CD8+ T cells.
Statistical analysis
The statistical analyses were performed using GraphPad Prism 5.0 software. Since the data were not normally distributed, they were presented as median and interquartile range. Kruskal–Wallis test with Dunnett's post hoc tests were used to compare the differences between groups. The association between the serum liver function indicators and CD32 MFI of CD4+ T, CD8+ T lymphocytes were assessed with a Spearman correlation. Values of p < 0.05 were considered to be statistically significant.
Results
Clinical characteristics of the subjects in each of the three groups
In our study, we recruited 68 chronic HBV-infected patients and 40 normal individuals. A total of 47 HBV infection patients with normal levels of ALT, AST, and HBV DNA and 21 patients with abnormal ALT, AST, and HBV DNA levels were employed as the HBV-LFN group and HBV-LFAN group, respectively. A total of 40 healthy individuals with normal checkup results were recruited as the NC group. The clinical characteristics of the subjects from HBV-LFN, HBV-LFAN, and NC groups are summarized in Table 1.
The CD4+ T and CD8+ T lymphocyte CD32 MFI and index were significantly increased in HBV-LFN and HBV-LFAN patients compared with NC
The CD32 MFI of circulating CD4+ T and CD8+ T lymphocytes was detected and the CD32 index of CD4+ T, CD8+ T and neutrophils was calculated. Representative flow cytometric results are shown in Figure 1. The CD32 MFI of CD4+ T and CD8+ T lymphocytes in HBV-LFN and HBV-LFAN patients were significantly increased than those in NC (Fig. 1A, B). The CD32 index of CD4+ T and CD8+ T lymphocytes in HBV-LFN and HBV-LFAN patients was remarkably higher when compared with the NC group (Fig. 1C). However, there was no significant difference in the neutrophil CD32 index among the three groups (Fig. 1C).
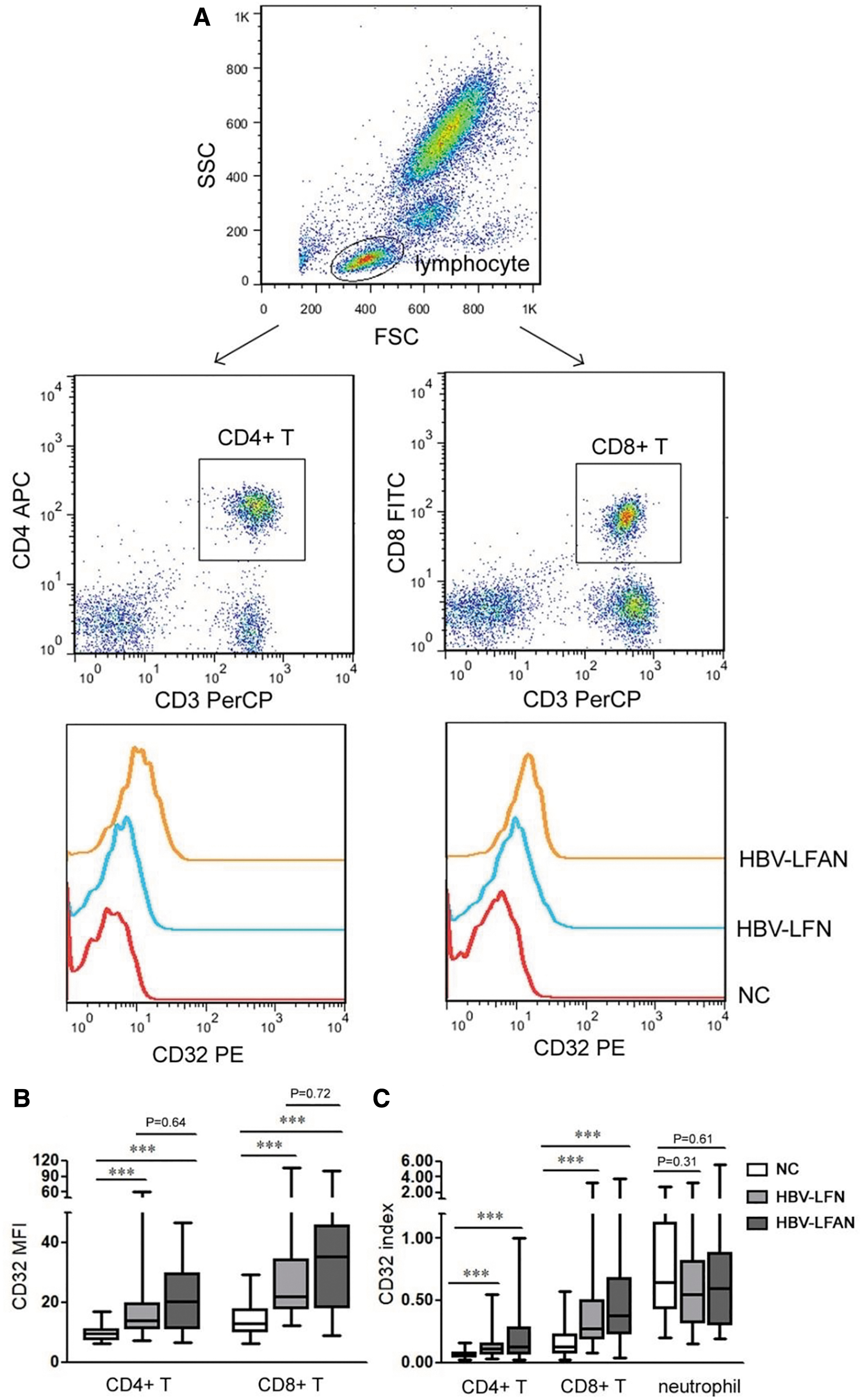
Detection and comparison of CD32 expression in the circulating CD4+ T, CD8+ T cells between chronic HBV patients and NC individuals.
CD32 MFI of CD4+ T and CD8+ T lymphocytes in the normal individual's PBMCs were significantly increased when stimulated with mixed HBV patients' plasma of high virus copies
To further observe the reactivity of CD4+ T and CD8+ T lymphocytes to HBV, PBMCs were isolated from normal individuals' peripheral blood, stimulated with auto plasma, mixed allogeneic plasma, and mixed HBV patients' plasma of low virus copies and high virus copies, respectively. The CD32 MFI of CD4+ T and CD8+ T lymphocytes was detected after an incubation for 24 h. Representative flow cytometric results are shown in Figure 2. The CD32 MFI of CD4+ T and CD8+ T lymphocytes stimulated with mixed HBV patients' plasma of high virus copies were significantly increased compared with those stimulated with auto plasma. The CD32 MFI of CD4+ T and CD8+ T lymphocytes stimulated with mixed allogeneic plasma and mixed HBV patients' plasma of low virus copies were higher than those stimulated with auto plasma, but was not significantly different (Fig. 2).

Detection and comparison of the CD32 MFI in CD4+ T and CD8+ T lymphocytes in normal individuals' PBMCs (n = 6) stimulated with auto plasma, mixed allogeneic plasma, mixed HBV patients' plasma of low virus copies and high virus copies, respectively (Kruskal–Wallis test with Dunnett's post hoc tests were used to compare the differences between groups. Median with IQR was presented, ***p < 0.001). PBMCs, peripheral blood mononuclear cells.
Correlation between CD32 MFI of CD4+ T, CD8+ T lymphocytes and levels of serum liver function indicators in HBV patients
To evaluate the correlation between CD32 MFI of CD4+ T, CD8+ T lymphocytes and liver function indicator levels in HBV patients, a Spearman correlation analysis was carried out. The results showed that there was a significant positive correlation between CD32 MFI of CD4+ T, CD8+ T lymphocytes and serum AST level (Fig. 3). However, remarkable correlation relationships were not identified between the CD32 MFI of CD4+ T, CD8+ T lymphocytes and level of ALT, TBIL, or DBIL (Fig. 3).

Correlation plots between the CD32 MFI of CD4+ T, CD8+ T cells and levels of ALT, AST, TBIL, and DBIL (Spearman correlation test was used for data analysis. *p < 0.05). ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBIL, direct bilirubin; TBIL, total bilirubin.
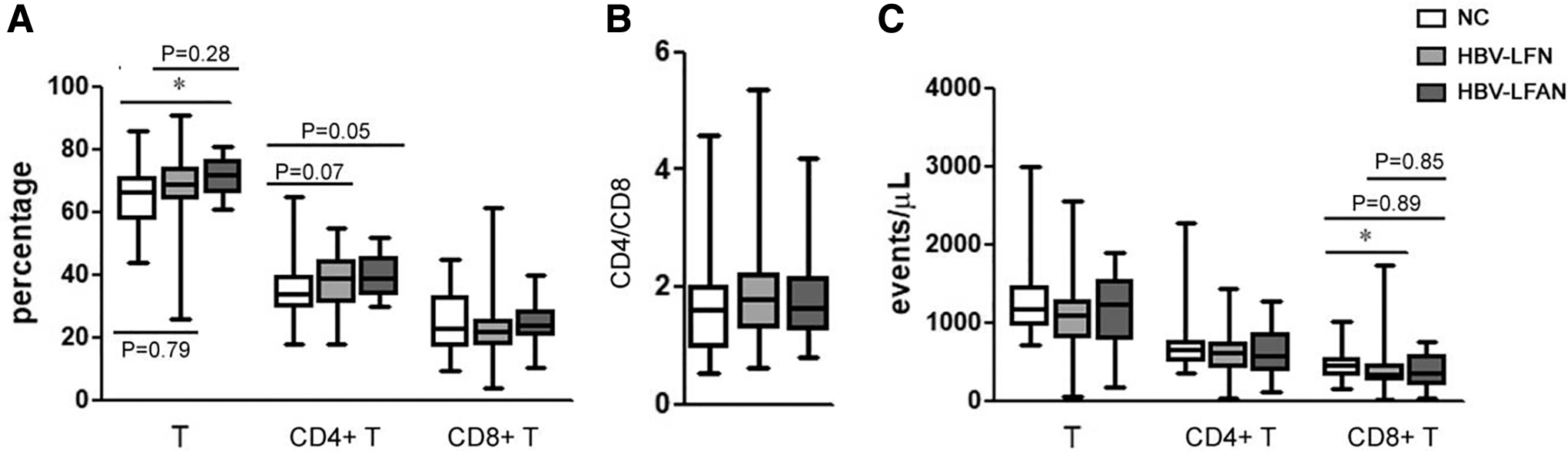
Relative and absolute numbers of T lymphocyte subsets alter the features in the peripheral blood of patients with HBV-LFN and HBV-LFAN groups
We analyzed the relative and absolute number of T lymphocyte subsets in the peripheral blood of the subjects in each of the three groups. The results are listed in Figure 4. The percentage of T lymphocytes in HBV-LFAN patients was significantly higher than those in the NC group, but had no significant difference on the absolute number. The absolute number of CD8+ T lymphocytes in HBV-LFN patients was significantly lower than those in the NC group, but had no significant change on the percentage. In addition, there were no significant differences in CD4+ T lymphocytes and the ratio of CD4+ T and CD8+ T among three groups.
Relative
Discussion
It has been well established that the host immune response plays a vital role in hepatitis B pathogenesis and clinical outcomes. Multiple immune cells, including T lymphocytes, are important in the immune regulation of HBV infection. Focusing on the activation states of immune cells, especially T lymphocytes, may provide new evidence and strategies for determining the immune status of HBV infectors, monitoring disease progression, and predicting the efficacy of antiviral treatment (Li et al., 2014). In this study, the level of CD32 expression in circulating CD4+ T and CD8+ T cells was assessed in chronic HBV infection patients. Our results showed that CD32 expression in circulating CD4+ T and CD8+ T cells was upregulated in both chronic HBV infection patients with normal liver function and abnormal liver function.
Moreover, the CD32 index of CD4+ T and CD8+ T lymphocytes in the patients with chronic HBV infection was remarkably higher when compared with the normal controls. It has been reported that CD32 expression was associated with cell activation (Badia et al., 2018; Huot et al., 2021; Virdi et al., 2020). Our results indicated that the circulating CD4+ T and CD8+ T cells in patients with chronic HBV infection were likely high activated lymphocytes. Similar to our results, Holgado et al. found that activation of CD4+ T cells promoted a marked increase in the expression of CD32 (Holgado et al., 2018).
FcγRs are widely expressed in immune cells and mediate a large array of effectors and immunomodulatory mechanisms that influence both innate and adaptive responses (Bournazos et al., 2014). The expression and function of FcγRs in innate immune cells and B cell have been clearly defined, but it is generally assumed that T cells do not express FcγRs (Nimmerjahn and Ravetch, 2008; Takai 2002). Whether CD32 expression in T cells or not remains controversial. In this study, we found not only that T cells express CD32, but also that CD32 expression levels of CD4+ T and CD8+ T were marked increased when stimulated the healthy individuals' lymphocytes with mixed patients' plasma containing high HBV copies. Our observations indicating that T cells express CD32 are in agreement with those reports (Holgado et al., 2018; Martin et al., 2018).
Previous studies revealed that HBV infection could induce dysfunction in the innate and adaptive immune responses that engage various immune cells (Cho and Cheong, 2021), and these immune cells could release various cytokines and chemokines (Coelho et al., 2005; Dunn et al., 2007; Liu et al., 2016). Moreover, Holgado et al. reported that immune complexes could promote CD4+ T cell activation (Holgado et al., 2018). Thus, we hypothesize that the mixed patients' plasma containing high HBV copies might through certain cytokines, chemokines or immune complexes to activate CD4+ T and CD8+ T cells; however, the precise mechanism requires further study.
It is well known that HBV replicates in hepatocytes but is noncytopathic, liver damage is thought to be immune mediated. For instance, NK cells may contribute to liver inflammation by TNF-related apoptosis-inducing ligand (TRAIL)-mediated death of hepatocytes (Dunn et al., 2007). CD8+ T cells could inhibit viral replication and mediate liver damage through a range of mechanisms, including the release of cytolytic granules (granzyme and perform) for the lysis of infected cells, induction of target cell apoptosis through cross-linking of cell-surface death receptors (FAS-FASL, TRAIL-TRAILR), and secretion of effector molecules (interferon-γ and tumor necrosis factor-α) (Bertoletti and Ferrari, 2012). CD4+ T cells are not likely to mediate direct liver damage during HBV infection, but these cells may help to induce and maintain HBV-specific cytotoxic T lymphocytes (Iannacone and Guidotti, 2022).
AS we all know that cell activation is usually prerequisite to play to the functions. In our study, we found that not only the circulating CD4+ T and CD8+ T cells in chronic HBV infection patients were high activated lymphocytes, but also the level of CD4+ T and CD8+ T CD32 expression was positively correlated with serum AST levels in HBV patients. These findings suggest that CD32 upregulation in CD4+ T, CD8+ T cells might represent a potential promising biomarker for assessing the severity of liver injury in chronic HBV patients.
Our study has two limitations. First, the sample size was small. Second, the precise mechanism that mixed HBV patients' plasma containing high HBV copies could activate resting lymphocytes required further study. In addition, further research is needed to confirm our findings to determine whether the level of CD32 expression in circulating CD4+ T and CD8+ T cells or CD32 index of CD4+ T and CD8+ T lymphocytes could be used as a routine laboratory test to evaluate liver damage in patients infected with HBV.
Footnotes
Authors' Contributions
C.-y.Y. conceived of the study, performed the flow cytometric analysis, writing, and revising of the article; Z.-x.C. supervised and took the leadership responsibility for the research activity planning and execution, supervised, and revised the final article; Z.-s.H. and R.-l.Y. performed the hematological and the laboratory work for the patients; J.J. took part in the laboratory work and data analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from Health Commission of Hefei City Scientific Research Project (Hwk2020yb004). Doctor Projects of the Second People's Hospital of Hefei (2020bszx02).