
Abstract
According to current knowledge, the etiopathogenesis of multiple sclerosis (MS) is complex, involving genetic background as well as several environmental factors that result in dysimmunity in the central nervous system (CNS). MS is an immune-mediated, inflammatory neurological disease affecting the CNS. As part of its attack on the axons of the CNS, MS witnesses varying degrees of myelin and axonal loss. A total of about 20 disease-modifying therapies (DMTs) are available today that, both in clinical trials and in real-world studies, reduce disease activity, such as relapses, magnetic resonance imaging lesions, and disability accumulation. Currently, the world is facing an outbreak of the new coronavirus disease 2019 (COVID-19), which originated in Wuhan, Hubei Province, China, in December 2019 and spread rapidly around the globe. Viral infections play an important role in triggering and maintaining neuroinflammation through direct and indirect mechanisms. There is an old association between MS and viral infections. In the context of MS-related chronic inflammatory damage within the CNS, there has been concern regarding COVID-19 worsening neurological damage. A high rate of disability and increased susceptibility to infection have made MS patients particularly vulnerable. In addition, DMTs have been a concern during the pandemic since many DMTs have immunosuppressive properties. In this article, we discuss the impact of DMTs on COVID-19 risks and the effect of DMTs on COVID-19 vaccination efficacy and outcome in MS patients.
Introduction
Multiple sclerosis (MS) is an immune-mediated neurodegenerative disease of the central nervous system (CNS), which typically affects young individuals 20–40 years of age and is more prevalent in females (Jafarinia et al., 2020d). MS incidence and prevalence are on the rise throughout the world, and it has been estimated that nearly 2.8 million people are living with MS worldwide (Walton et al., 2020). The disease is mainly characterized by two pathological hallmarks: demyelination and neurodegeneration (Jafarinia et al., 2020b). MS is an immune-mediated disease, and through the course of the disease, autoreactive T lymphocytes cross the blood–brain barrier (BBB) and encounter CNS antigens presented by dendritic cells (Jafarinia et al., 2020c). Activated macrophages and T cells can directly attack components of the CNS and cause neuroinflammation, demyelination, gliotic scarring, and axonal loss (Comi et al., 2021; Lazibat et al., 2018).
However, in recent years, there has been a conceptual shift in perceiving the immune-mediated pathology of MS, and it has been proven that B cells also have a key role in disease pathogenesis (Jafarinia et al., 2020a). B lymphocytes can influence the disease through a variety of mechanisms, including the formation of ectopic lymphoid follicles within the CNS, antigen presentation, cytokine production, antibody production, and maturation into antibody-producing plasma cells (Comi et al., 2021; Lehmann-Horn et al., 2017).
The underlying cause of MS is still unclear, but it is believed that it is a multifactorial disease and a combination of environmental, genetic, and epigenetic factors may trigger it (Jafarinia et al., 2020b). There is compelling evidence in support of the fact that viruses such as Epstein–Barr virus (EBV) may play a role in MS pathogenesis. Indeed, viral agents can trigger or accelerate autoreactive immune responses in MS patients through several mechanisms, including bystander activation, molecular mimicry, and viral support for autoreactive cell survival. This issue gains more importance during the coronavirus disease 2019 (COVID-19) global pandemic (Marcucci and Obeidat, 2020; Marrodan et al., 2019). It has been hypothesized that Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) (a strain of coronavirus that causes COVID-19) can induce and exacerbate MS mainly through permeabilizing the BBB by inducing the secretion of proinflammatory signals and providing activation signals for autoreactive lymphocytes (Amruta et al., 2021).
In this article, we discuss the impact of disease-modifying therapies (DMTs) on COVID-19 risks and the effect of DMTs on COVID-19 vaccination efficacy and outcome in MS patients.
SARS-CoV-2
COVID-19 has put a huge burden on the health care system. SARS-CoV-2 was first isolated and identified in Wuhan City, Hubei Province, China, on December 2019 (Zhang et al., 2020). By March 2022, as a rapidly spreading infection, the virus had infected nearly 477 million cases and caused about six million deaths (Jamali et al., 2022). SARS-CoV-2 is a single-stranded RNA virus. Ligation of the virus S protein with its receptor, angiotensin-converting enzyme 2 (ACE2), on type 2 pneumocytes in the human lung facilitates virus entry into lung cells. Then the virus replicates in lung cells and viral components are released (Fattahi et al., 2022; Khalifehzadeh-Esfahani et al., 2022). Virus interaction with lung dendritic cells through pattern recognition receptors and Toll-like receptors triggers local inflammatory responses and promotes the secretion of inflammatory cytokines, such as interleukin-1β (IL-1β), IL-6, transforming growth factor-β1, tumor necrosis factor-α (TNF-α), and chemokines, which can contribute to the recruitment of circulating leukocytes (Laham et al., 2004).
In severe forms of COVID-19, the inflammatory cascade can lead to a cytokine storm, which is the key factor in the development of acute respiratory distress syndrome (ARDS) and extrapulmonary organ failure (Darif et al., 2021).
SARS-CoV-2 is not confined to the respiratory system. In addition to human airway epithelia, lung parenchyma ACE2 is expressed in a variety of tissues, including vascular endothelia, kidney cells, and small intestinal cells (Gheware et al., 2022). Body-wide perspective analysis of ACE2 expression at both the messenger RNA (mRNA) and protein levels has revealed little or no expression of ACE2 in the human brain. While SARS-CoV-2 has neuroinvasive potential and has been isolated from the CNS tissue of MS patients (Yachou et al., 2020). This implies the presence of a potential alternative mechanism for host entry by the virus. However, the exact basis of CNS involvement in COVID-19 has yet to be determined.
Impact of COVID-19 on Severity, Mortality, and Outcome of MS
The impact of SARS-CoV-2 infection on the clinical manifestations of MS patients was not clear at the onset of the pandemic. However, the rapid spread of the virus throughout the globe highlights the urgent need for reliable information about the susceptibility to severe COVID-19 disease in MS patients. Furthermore, the immunomodulatory effect of DMTs in MS patients presents another challenge in SARS-CoV-2-infected MS patients (Smith et al., 2022).
In a study by Bsteh et al. (2021), they enrolled 126 MS patients with COVID-19, of whom 86.5% had a mild course, 9.5% had a severe course, and 3.2% died from COVID-19, and a priori risk significantly predicted the severity and mortality of COVID-19. They also demonstrated that, after controlling for other known risk factors, the COVID-19 outcome was not associated with DMTs or immunosuppressive DMTs (Bsteh et al., 2021). In another study, Sepúlveda et al. (2021) enrolled 407 MS patients in their study, with 84% having relapsing–remitting MS and 74.7% taking DMTs. Their results showed that in 5 patients (1.2%), COVID-19 was confirmed, and in 46 (11.3%), it was suspected.
They also demonstrated that the cumulative incidence of confirmed COVID-19 cases was similar to that of the general population but was almost twofold higher when all cases were considered. Six people (11.7%) were admitted to the hospital; five made a full recovery, and one died. Patients who were hospitalized were frequently male, had diabetes, and had progressive MS, and DMTs were not linked to either the likelihood of infection or the outcome (Sepúlveda et al., 2021).
In a systematic review by Barzegar et al. (2021), the factors associated with COVID-19 susceptibility and outcomes among MS patients were reviewed. This study showed that a history of contact with an infected person is the most important risk factor for COVID-19 susceptibility. Younger age, a relapsing course, and anti-CD20 agents are additional factors that may be linked to infection. Increasing age, more severe MS, anti-CD20 therapy, past corticosteroid usage, and certain comorbidities (obesity and coronary artery disease) may all be independently related to worse infection outcomes, according to the evidence. Male sex is probably a risk factor for more severe diseases. It was noted that being black or African American could be risky (Barzegar et al., 2021).
Impact of DMTs on COVID-19
MS patients are vulnerable to particular infections due to the immunosuppressive and immunomodulatory medications that they require (Luna et al., 2020). Therefore, during the COVID-19 pandemic, many MS patients faced the challenging question of continuing or interrupting their medication. Although some immunosuppressive therapies can increase the risk of severe infections in MS patients, on the other hand, these medications may alleviate the robustness of the immune response and limit the proinflammatory conditions and cytokine storm in MS patients (Yano et al., 2019). Indeed, the COVID-19 clinical course, severity, and outcome in MS cases will be greatly affected by the type of MS therapy and its mechanisms of action in a beneficial or harmful way (Simpson-Yap et al., 2021). There are nine classes of Food and Drug Administration-approved therapies for MS, which will be discussed further in this section.
Natalizumab
Natalizumab is a humanized monoclonal antibody against the cell adhesion molecule α4-integrin. It binds to α4β1-integrin and blocks its interaction with vascular cell adhesion protein-1, thus inhibiting lymphocyte entry to the CNS and preventing acute demyelinating relapses (Li et al., 2018). Regarding the fact that Natalizumab limits immune trafficking in the CNS, it may impair the viral clearance process in the brain during SARS-CoV-2 infection and result in encephalitis. Natalizumab also interferes with the homing of lymphocytes into the CNS, reducing immune surveillance against viral infections (Aguirre et al., 2020; Díaz-Díaz et al., 2021; Marchetti and Engelhardt, 2020). On the other hand, Natalizumab can have a protective role by blocking virus entry to the cells since integrin may act as an alternative receptor for SARS-CoV-2. To date, two cases of COVID-19 in patients with MS treated with Natalizumab have been reported; both cases had a benign clinical course and complete recovery (Chisari et al., 2021).
Interferon-β
Interferon-β (IFN-β) is an immunomodulating and antiviral agent that suppresses inflammation primarily by increasing the expression of anti-inflammatory cytokines while decreasing the expression of proinflammatory cytokines (Noronha et al., 1993). It induces IL-10 secretion and downregulates major histocompatibility complex (MHC) class II expression in antigen-presenting cells (APCs). IFN-β also inhibits viral replication. Furthermore, IFN-β inhibits inflammatory cell trafficking across the BBB and promotes neuronal survival and repair by increasing nerve growth factor production. Another way IFN-β exerts antiviral immunity is by increasing the number of CD56bright natural killer (NK) cells in the peripheral blood. NK cells secrete anti-inflammatory mediators and may have the potential to curb neural inflammation. IFN-β reduces lung vascular permeability through CD79 expression (Cosentino et al., 2005; Dhib-Jalbut and Marks, 2010). In vitro observations by Clement et al. (2020) revealed that IFN-β-1a was highly effective in inhibiting both infectious virus particles and viral RNA SARS-CoV-2 replication in Vero E6 cells.
Furthermore, several studies show that IFN-β-1a administration in MS patients with SARS-CoV-2 infection is not associated with the severity or adverse outcomes of the infection when compared with MS cases who do not take DMTs (Moghadasi and Anjidani, 2021). IFN-β-1a may be safe to use in ARDS as well. Several studies also show that the length of hospitalization, mortality, intensive care unit admission, and intubation rate were significantly lower among COVID-19 patients taking IFN β-1a (Rahmani et al., 2020; Sharifian-Dorche et al., 2021; Sosa et al., 2021).
As previously mentioned in the “SARS-CoV-2” section, virus (such as SARS-CoV-2) interaction with lung dendritic cells triggers local inflammatory responses and promotes Th17 cells after interaction with the virus. Then Th17 cells secrete IL-17, which causes the activation of monocytes, macrophages, and neutrophils. These cells produce a massive amount of inflammatory cytokines, such as IL-6, IL-1β, TNF-α, and IFN-γ, resulting in a cytokine storm (Darif et al., 2021; Martonik et al., 2021). It has been proposed that IFN-β inhibits virus replication by reducing the production of inflammatory cytokines (Dorgham et al., 2021) (Fig. 1).
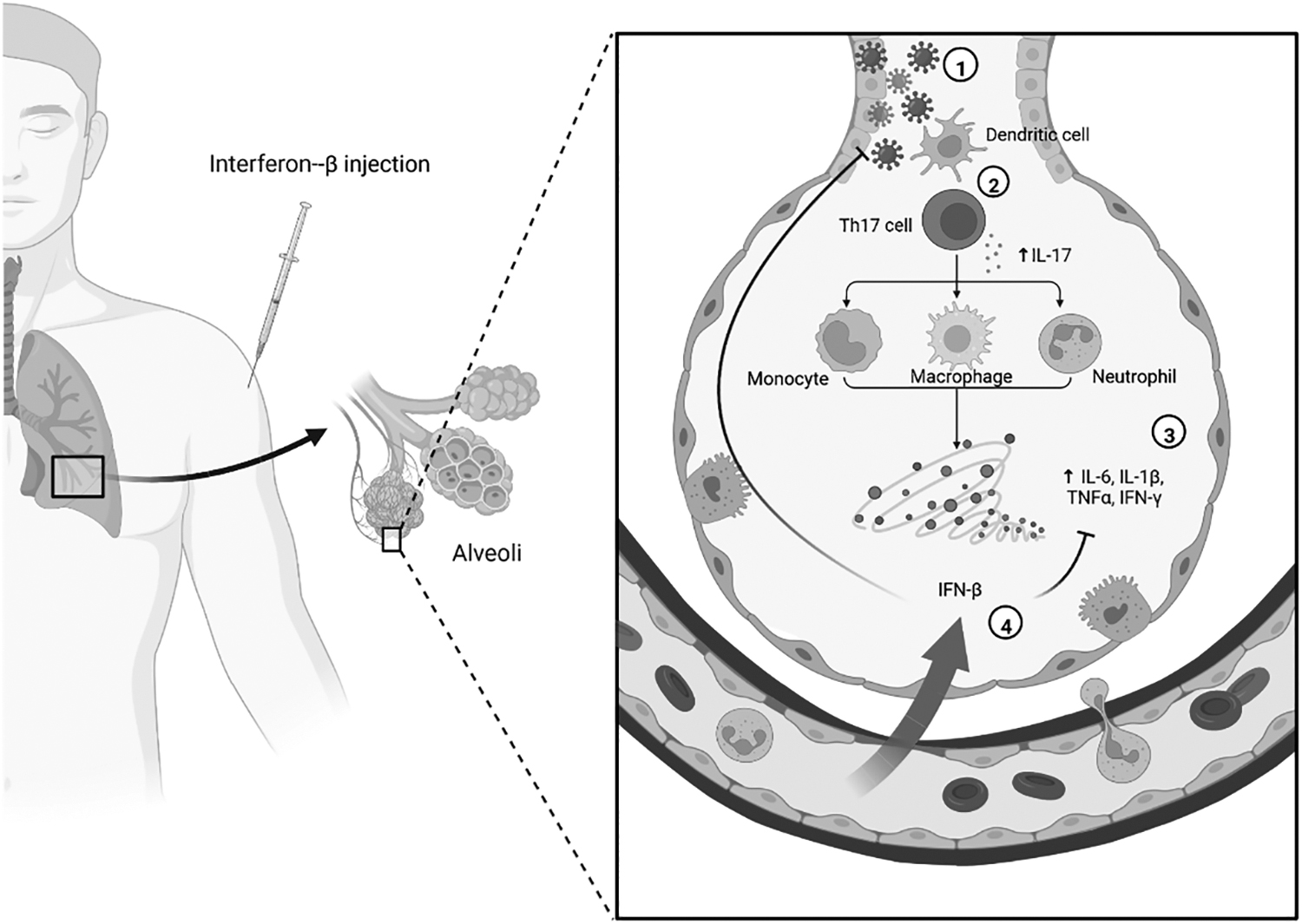
The process of cytokine storm in the lung and the inhibitory effect of IFN-β. (1) SARS-CoV-2 infects lung cells, (2) dendritic cells promote Th17 cells after interaction with the virus; then, Th17 cells secrete IL-17, which causes the activation of monocytes, macrophages, and neutrophils. (3) These cells produce a massive amount of inflammatory cytokines, such as IL-6, IL-1β, TNF-α, and IFN-γ, or in other words cytokine storm. (4) IFN-β reduces the production of inflammatory cytokines and also hinders the replication of the virus. IFN, interferon; IL, interleukin; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TNF, tumor necrosis factor.
Glatiramer Acetate
Glatiramer acetate (GA) is a synthetic protein that is composed of four amino acids resembling myelin basic protein (MBP). GA is a T cell receptor antagonist for the MBP epitope and competes with myelin antigens for interaction with APCs (Prod'homme and Zamvil, 2019). It also inhibits T cell responses to several myelin antigens through binding to MHC molecules. GA induces GA-specific regulatory CD4+ and CD8+ T cells and a Th1–Th2 shift that ultimately counteracts proinflammatory responses. GA is an immunomodulatory drug that modifies T cell responses to myelin (Boziki et al., 2019; Kasindi et al., 2022). Since GA is not associated with significant immunosuppression and a considerable risk of viral infection, it seems to be a safe drug (neither beneficial nor detrimental) for SARS-CoV-2-infected MS cases (Cabreira et al., 2021).
Dimethyl Fumarate
Dimethyl fumarate (DMF) is an anti-inflammatory drug that is widely used as an anti-inflammatory therapeutic in MS (Diaz et al., 2018). DMF works primarily through an activating nuclear factor erythroid-derived 2 (E2)-related factor (Nrf-2)-dependent mechanism to exert its antioxidant and anti-inflammatory effects. Nrf-2 induces cellular antioxidant defense systems and regulates tissue damage and the inflammatory response during infection (Yadav et al., 2019). Activation of the nuclear factor erythroid-derived 2-like 2 (NRF2) pathway by DMF can activate antiviral responses, limiting viral replication and the inflammatory process (Diebold et al., 2022).
Results of a survey by Olagnier et al. (2020) demonstrated that NRF2-response is suppressed in COVID-19 patient biopsies. They also showed that treatment with DMF as an agonist can inhibit SARS-CoV-2 replication, and regulate the expression of inflammation-associated genes (Olagnier et al., 2020). Moreover, some case-series studies have revealed that DMF has a protective role against SARS-CoV-2, and continuing DMF might be safe since COVID-19 severity and hospitalization rate were lower in MS patients receiving DMF (Barzegar et al., 2022).
Teriflunomide
Teriflunomide is an immunomodulatory DMT that reduces demyelination and axonal/neuronal injury in MS patients by inhibiting the proliferation of stimulated lymphocytes. In detail, teriflunomide reversibly inhibits dihydro-orotate dehydrogenase, which is a mitochondrial enzyme that plays a crucial role in the de novo pyrimidine synthesis pathway. Consequently, DNA synthesis in the S phase of the cell cycle and proliferation of B and T lymphocytes will be blocked (Tilly et al., 2021). There is compelling evidence that implies the antiviral effect of teriflunomide against a range of viruses, including ebola, cytomegalovirus, EBV, picornavirus, etc. (Bilger et al., 2017).
It is suspected that during SARS-CoV-2 infection, teriflunomide exerts its antiviral role through two mechanisms: interference with viral replication in infected cells and modulation of the immune system through inhibiting cytokine secretion, decreasing immune cell activation, and blocking cell proliferation (Maghzi et al., 2020). Since teriflunomide therapy may have a protective role against SARS-CoV-2, its consumption should not be interrupted in MS patients who developed SARS-CoV-2 infection (Capone et al., 2021).
Fingolimod
Fingolimod is a functional antagonist of the sphingosine-1-phosphate (S1P) receptors that are expressed by several cellular types, including lymphocytes, by blocking lymphocyte trafficking to target organs (Tran et al., 2020). Fingolimod sequesters lymphocytes in lymph nodes, preventing them from contributing to an autoimmune reaction. In addition to an overall reduction of 73% from baseline in the total mean circulating lymphocyte count, the treatment also preferentially sequesters naive and central memory lymphocytes over effector memory lymphocytes (Vahed et al., 2021). As a treatment for relapsing MS, fingolimod decreases the number of lymphocytes in secondary lymphoid organs by modulating peripheral lymphocyte counts (Chun et al., 2021). As a result, there are some concerns about the increased risk of SARS-CoV-2 infection in these patients. Fingolimod-treated MS patients are at greater risk of serious SARS-CoV-2 infection due to a lack of humoral and T cell immune responses. There have been 257 reports of COVID-19 in patients taking fingolimod. Most of the patients recovered completely despite lymphopenia.
Researchers have found that S1P signaling mediates lung injury in ARDS and that fingolimod promotes endothelial integrity, which may be beneficial in treating COVID-19. The use of fingolimod in MS patients is not associated with an increased risk of severe or symptomatic SARS-CoV-2 infection (Laroni et al., 2021; Meacci et al., 2020).
Alemtuzumab
The drug, alemtuzumab, is an immunoglobulin G1 (IgG1) antibody that targets CD52 and is used to treat chronic lymphocytic leukemia and MS (Qi et al., 2019). In addition to antibody-dependent cytotoxicity, it also acts through complement-dependent cytotoxicity. It also activates proapoptotic pathways in CD52-expressing cells. Following administration, alemtuzumab reduces the cellular count of T and B lymphocytes for many months (Zappulo et al., 2019). There were 37 reported patients on Alemtuzumab and COVID-19. Most had benign courses and healed completely. After the lymphocytes are depleted, Alemtuzumab produces new lymphocytes from a different lineage. By reconstituting lymphocytes, including changes in composition, phenotype, and function, the new lineage might be able to resist the virus or blunt the cytokine storm associated with SARS-CoV-2-associated complications (Carandini et al., 2020; Iovino et al., 2021; Matías-Guiu et al., 2020).
Cladribine-Phosphates
Cladribine-phosphates interfere with DNA synthesis and repair by incorporating into DNA and inhibiting enzymes involved in DNA metabolism, such as DNA polymerase and ribonucleotide reductase (Rammohan et al., 2020). This prodrug interferes with the metabolism of cells and inhibits DNA repair, causing apoptosis, particularly in lymphocytes. Cladribine mainly affects CD4+ and CD8+ T cells, as well as B cells (Hermann et al., 2019; Jacobs et al., 2018). Therefore, it could be hypothesized that the risk of severe SARS-CoV-2 infection from drugs leading to transient suppression of T, B, and NK cell responses may be augmented in the first few months after treatment, however, the few reported cases of COVID-19 shortly after alemtuzumab and cladribine treatments show a very mild disease course (De Angelis et al., 2020).
Anti-CD20 Antibodies (Ocrelizumab, Ofatumumab, or Rituximab)
Anti-CD20 antibodies are used for the treatment of several immune-mediated diseases, including MS, as well as in the treatment of B cell hematological malignancies. Anti-CD20 treatments directly affect B cell responses, and also have an impact on T cell responses, mainly through decreased interactions between T and B cells (Dierickx et al., 2011). In addition, anti-CD20 agents reduce proinflammatory B cell cytokines, such as IL-6. Some lines of evidence imply a higher risk of infection in MS patients on Rituximab than with platform MS DMTs. Hypogammaglobulinemia may be observed in patients who have had prolonged use of anti-CD20 therapies, but is rarely associated with severe infection (Ratanatharathorn et al., 2000).
There are several reports of COVID-19 in patients receiving anti-CD20 monoclonal antibodies (Patel et al., 2022). Results of a cohort study in Italy revealed an increased risk of severe forms of COVID-19 in MS patients treated with ocrelizumab. Moreover, the French cohort of 347 MS patients, while not demonstrating a detrimental role of DMTs on the risk of developing a severe form of COVID-19, reported the occurrence of ARDS in two obese patients treated with ocrelizumab (Schiavetti et al., 2022).
A study from Iran found an increased risk of COVID-19 cases in patients treated with rituximab, although the use of the drug was not associated with the increased possibility of hospitalization (Schiavetti et al., 2022). Although there have been critical and fatal COVID-19 cases among MS patients taking anti-CD20 agents, the severity of SARS-CoV-2 infection in these patients (ocrelizumab or rituximab) is comparable to the general population (Iyer et al., 2022).
Effect of DMTs on COVID-19 Vaccination Efficacy and Outcome in MS Patients
For people under DMTs, knowing which vaccine is more compatible with their treatment and less harmful is critical (Fig. 2). There are 18 approved vaccines used in the clinical phase, which are divided into four main groups: (1) nucleic acid vaccines, (2) protein-based vaccines, (3) viral vector vaccines, and (4) whole virus vaccines (live attenuated or inactivated vaccines) (Ndwandwe and Wiysonge, 2021). In this study, we will investigate the impact of DMTs on the efficacy of the most common types of COVID-19 vaccination, such as Pfizer-BNT162b2, Moderna, AstraZeneca, and Sinopharm.
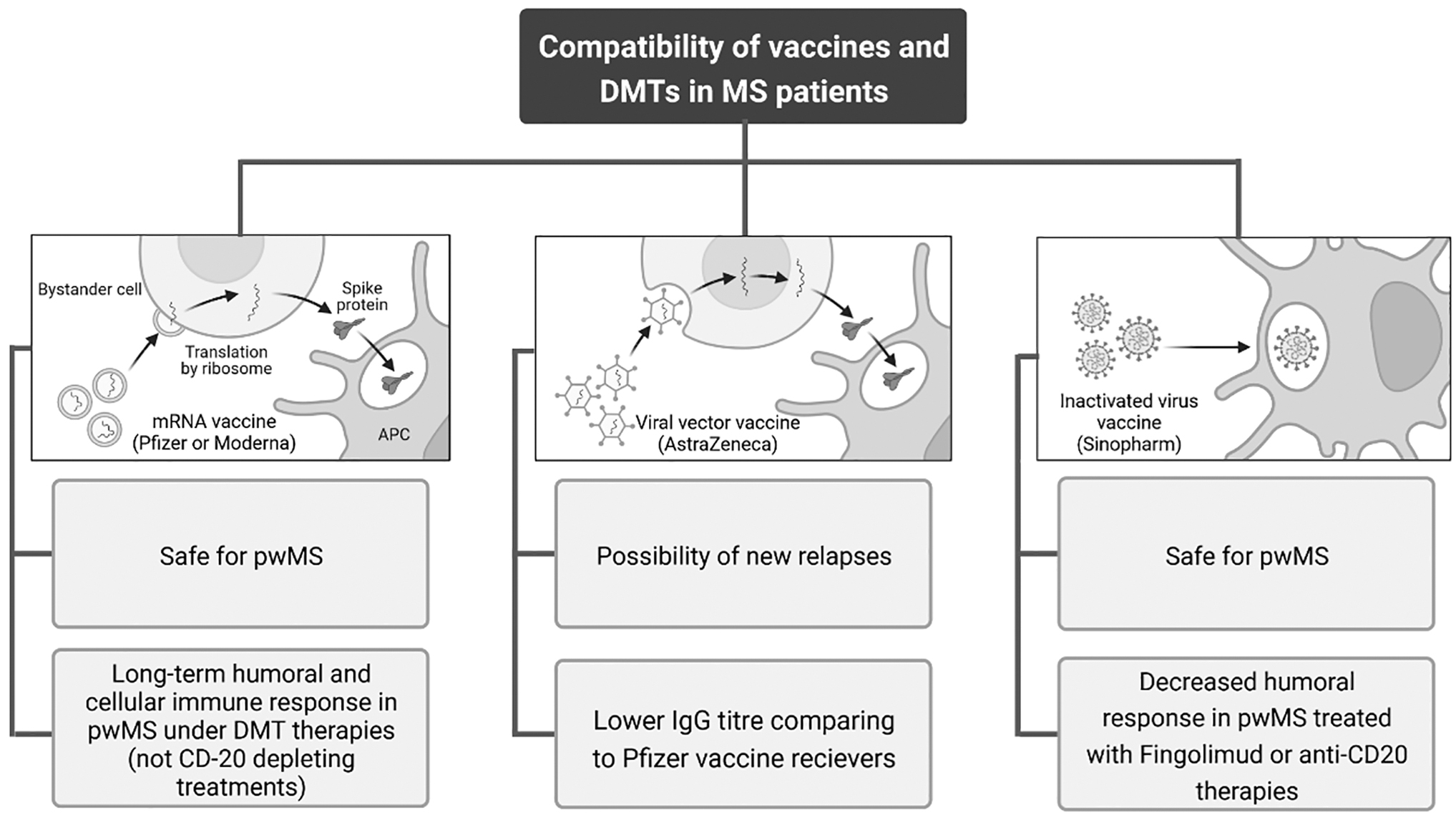
A brief comparison of the compatibility of the different kinds of vaccines and DMTs in pwMS. From left to right: mRNA vaccine; viral vector vaccine; inactivated virus vaccine. APC, antigen-presenting cell; DMTs, disease-modifying therapies; IgG, immunoglobulin G; mRNA, messenger RNA; MS, multiple sclerosis; pwMS, patients with multiple sclerosis.
Nucleic Acid Vaccines
Pfizer (BNT162b2) and Moderna (mRNA-1273) are the two successful mRNA vaccines against COVID-19. Moderna, which is mRNA-1273 in a prefusion-stabilized form, encodes the SARS-CoV-2 spike (S) protein. Whereas Pfizer, a synthesized mRNA combined with lipid nanoparticles, encodes the trimerized S protein receptor-binding domain of SARS-CoV-2 (Xu et al., 2020). Although the understanding of the innate and adaptive immune response to this type of vaccine is limited, there are a sufficient number of articles on the immune response of patients with (pw) MS to SARS-CoV-2 mRNA vaccines.
Brill et al. (2022) demonstrated that after receiving the second dose of the BNT162b2 mRNA vaccine, all MS patients treated with Cladribine tablets or IFN-β-1a had a positive serology response. In addition, in a case report study of asymptomatic SARS-CoV-2 infection in a female MS patient treated with Natalizumab (for the past 10 years), who was fully vaccinated by the BNT162b2 mRNA vaccine, efficient and specific anti-SARS-CoV-2 immunity through the activation of T cells has been shown. Anti-SARS-CoV-2 antibodies, on the other hand, were not detectable (Jakimovski and Weinstock-Guttman, 2022). Confirming this finding, a long-term humoral response after a full mRNA COVID-19 vaccination cycle has been proved in a 6-month follow-up study of pwMS treated with Natalizumab (Altieri et al., 2022).
Investigators have examined the effects of Fingolimod, Cladribine, and Ocrelizumab on the humoral immune response to the Pfizer-BNT162b2-COVID-19 vaccination in 125 MS patients. They found that 97.9% of healthy subjects, all untreated MS patients, and all MS patients treated with cladribine showed a high level of antibodies post-COVID-19 vaccination, whereas only 3.8% of Fingolimod-treated patients and 22.7% of Ocrelizumab-treated patients had an antibody response after vaccination (Achiron et al., 2021).
Similarly, Guerrieri et al. (2021) showed a positive serology response, but a weak one, in MS patients under Ocrelizumab (62.5%) and Fingolimod (37.5%) treatment after 2 weeks from the first dose of vaccination. In line with these results, other studies revealed an attenuated short-term and long-term humoral response in pwMS treated with these two DMTs who received the two doses of mRNA COVID-19 vaccine (Achiron et al., 2021; Capuano et al., 2022b; Sormani et al., 2021; Tallantyre et al., 2022). In a study on 140 pwMS in Italy, it has been shown that SARS-CoV-2 mRNA vaccines (Pfizer and Moderna) are safe and without any severe side effects.
The subjects in this study were a mixture of pwMS treated with baseline DMTs and high-efficacy DMTs. Although 86.8% of the study population showed a high titer of IgG against SARS-CoV-2, the amount of IgG titer in the group treated with Ocrelizumab and Fingolimod was significantly lower than in others (Capone et al., 2022).
The safety and efficacy of the third dose mRNA vaccination have also been confirmed by some articles (Dreyer-Alster et al., 2022; König et al., 2022). In a very recent article, researchers investigated the effect of the third booster dose on MS patients treated with Ocrelizumab and Fingolimod, and they found a significant increase in their antibody response after the booster vaccine without any relapses or severe clinical observations (Capuano et al., 2022a). Moreover, Madelon et al. (2022) stated that the third dose of mRNA vaccination can cause a strong T cell response against Delta and Omicron variants in pwMS treated with Ocrelizumab. Conversely, Achtnichts et al. (2021) showed that even after the third dose of SARS-CoV-2 mRNA vaccination, the level of IgG antibodies against the spike receptor-binding domain in pwMS who are under CD20-depleting therapies such as Rituximab and Ocrelizumab is modest. This study aligns with another that demonstrated a significantly lower rate of seroconversion in mRNA-vaccinated pwMS treated with CD20-depleting therapies (Ali et al., 2021).
Taken together, these findings show a long-term humoral response to mRNA COVID-19 vaccines in pwMS treated with DMTs other than CD20-depleting therapies, particularly ocrelizumab.
Viral Vector Vaccines
ChAdOx1 nCoV-19 (AstraZeneca) is a genetically engineered chimpanzee adenovirus vaccine developed by the University of Oxford (Kashte et al., 2021). There have been few studies looking into the safety and efficacy of AstraZeneca vaccination in pwMS. In a large-scale study, it was demonstrated that pwMS on DMTs (not anti-CD20-depleting therapies) who received ChAdOx1 nCoV-19 had a significantly lower IgG titer compared with a group receiving BNT162b2 mRNA vaccine with the same condition (Tallantyre et al., 2022). Moreover, Fragoso et al. (2022) reported new relapses, confirmed by magnetic resonance imaging, after 7–25 days from the first dose of AstraZeneca vaccination in 8 pwMS under DMTs, which is in line with the findings of a case report study (Nistri et al., 2021). These findings highlight the importance of taking precautionary measures when using ChAdOx1 nCoV-19 for pwMS.
Whole Virus Vaccines (Inactivated)
The safety of the BBIBP-CorV (Sinopharm) vaccine for pwMS has been proven in some articles, mostly carried out in Iran (Kavosh et al., 2022; Sahraian et al., 2021). Similar to the findings of DMTs on mRNA vaccination in pwMS, some studies have found that the humoral response after receiving the Sinopharm vaccine decreases in pwMS treated with Fingolimod or anti-CD20 therapies (Etemadifar et al., 2022; Ghaffari et al., 2022).
A few studies are showing the efficacy of BBIBP-CorV compared with other vaccines in MS. Drulovic et al. (2021) investigated 22 pwMS who were treated with Cladribine and Alemtuzumab. In this study, 11 subjects with Cladribine therapy and without prior SARS-CoV-2 infection were vaccinated. Four pwMS vaccinated with two doses of Pfizer developed SARS-CoV-2 IgG antibodies (74.3 ± 42.9), and only three out of seven pwMS (42.9%) vaccinated with two doses of Sinopharm showed a SARS-CoV-2 IgG titer (35.0 ± 7.2). It was also demonstrated that three out of four pwMS with Cladribine therapy and prior SARS-CoV-2 infection had a positive humoral response after vaccination; two of them received Pfizer and two others received Sinopharm. The one who had no antibodies was vaccinated with Sinopharm (Drulovic et al., 2021). This result may be explained by the fact that the population of this survey is limited, but it is clear that the protection rate of Sinopharm is lower than Pfizer in pwMS under DMTs.
Conclusion
Results of different studies provide encouraging evidence that COVID-19 risk may be individually anticipated in MS and that treatment options should be primarily focused on treating MS rather than the pandemic, except for a very small proportion of high-risk patients. pwMS are advised to receive the COVID-19 vaccination. The safety and effectiveness of COVID-19 vaccinations may be impacted by DMTs. For people with MS, different types of vaccines are probably safe. If possible, live-attenuated vaccines should be avoided in patients who are being treated. While CD20-depleting therapies (especially ocrelizumab) and S1P modulators are predicted to attenuate vaccine responses, other DMTs are not expected to significantly impact the efficacy of COVID-19 vaccines.
Footnotes
Authors' Contributions
E.J. drafted the article and reviewed the literature;
Authorship Confirmation
Dr. Jamali, Dr. Farrokhi, Dr. Vakili, Dr. Iravanpour, Dr. Tavakoli Oliaee, and Dr. Jafarinia are from Shiraz University of Medical Sciences (Shiraz, Iran). Dr. Jamali is also from Peyvand Pathobiology and Genetic Laboratory (Shiraz, Iran). Dr. Rostamzadeh is from Yasui University of Medical Sciences (Yasui, Iran), all where education and research are the primary functions.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
This study was funded by Shiraz University of Medical Sciences (Grant number: 26759).