
Abstract
Numerous studies have highlighted the emergence of coronavirus disease (COVID-19) symptoms reminiscent of Kawasaki disease in children, including fever, heightened multisystem inflammation, and multiorgan involvement, posing a life-threatening complication. Consequently, extensive research endeavors in pediatric have aimed to elucidate the intricate relationship between COVID-19 infection and the immune system. COVID-19 profoundly impacts immune cells, culminating in a cytokine storm that particularly inflicts damage on the pulmonary system. The gravity and vulnerability to COVID-19 are closely intertwined with the vigor of the immune response. In this context, the human leukocyte antigen (HLA) molecule assumes pivotal significance in shaping immune responses. Genetic scrutiny of HLA has unveiled the presence of at least one deleterious allele in children afflicted with multisystem inflammatory syndrome in children (MIS-C). Furthermore, research has demonstrated that COVID-19 exploits the angiotensin-converting enzyme 2 (ACE-2) receptor, transmembrane serine protease type 2, and various other genes to gain entry into host cells, with individuals harboring ACE-2 polymorphisms being at higher risk. Pediatric studies have employed diverse genetic methodologies, such as genome-wide association studies (GWAS) and whole exome sequencing, to scrutinize target genes. These investigations have pinpointed two specific genomic loci linked to the severity and susceptibility of COVID-19, with the HLA locus emerging as a notable risk factor. In this comprehensive review article, we endeavor to assess the available evidence and consolidate data, offering insights into current clinical practices and delineating avenues for future research. Our objective is to advance early diagnosis, stabilization, and appropriate management strategies to mitigate genetic susceptibility's impact on the incidence of COVID-19 in pediatric patients with multisystem inflammation.
Introduction
With the onset of the coronavirus disease (COVID-19) epidemic in 2019, there has been a surge in reports of febrile children exhibiting unusual clinical features akin to those seen in Kawasaki disease. These manifestations include acute abdominal conditions, encephalopathy, toxic shock syndrome, and other related symptoms. These symptoms are characterized by fever, gastrointestinal disturbances, heightened inflammatory markers, and multiorgan involvement (Jones et al., 2020; Levin, 2020). Notably, ∼10% of children have been found to contract COVID-19, with the majority either remaining asymptomatic or displaying mild symptoms (Eastin and Eastin, 2020). Acute disease manifestations are more likely to occur in children younger than 1 year and those with underlying comorbidities (Tezer and Demirdağ, 2020). In this context, British pediatricians alerted the National Health Service to a perplexing inflammatory ailment, subsequently termed Pediatric Inflammatory Multisystem Syndrome Temporally Associated with Severe Acute Respiratory Syndrome Coronavirus 2 (PIMS-TS) (Tezer and Demirdağ, 2020).
The Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) have both provided definitions for this condition, now referred to as multisystem inflammatory syndrome in children (MIS-C). National data from Asian, European, and North American countries suggest that 2.1% to 7.8% of pediatric cases of COVID-19 evolve into MIS-C (Flood et al., 2021). Given that most pediatric cases of COVID-19 present with mild or even asymptomatic symptoms, there is a prevailing hypothesis that multisystem inflammation may be an autoimmune response post-infection (Belhadjer et al., 2020). This condition typically surfaces around 1 month after exposure to COVID-19. It predominantly afflicts relatively older children, ranging from 3 to 8 years of age, marking it as a significant inflammatory disorder in the pediatric population during the COVID-19 pandemic (Jones et al., 2020; Mazer et al., 2022b).
As COVID-19 virus infections constantly engage the immune system, the extent of the immune response plays a pivotal role in determining the severity or mildness of the infection. It is imperative to understand that the immune system comprises two fundamental components: innate and adaptive immunity. The innate immune system acts as the body's first line of defense and encompasses natural killer (NK) cells, dendritic cells (DCs), macrophages, and neutrophils. In addition, adaptive immunity includes T cells and B cells. Remarkably, the coronavirus can directly infiltrate macrophages and T cells (Dandekar and Perlman, 2005; Rodrigues et al., 2023). Invasion by neutrophils, monocytes, and/or macrophages results in an excessive release of inflammatory cytokines, triggering a cytokine storm that inflicts lung damage (Queiroz et al., 2023). This cascade can also activate T-helper lymphocytes (Th1/Th17) and induce cytotoxic T cell activity, further amplifying the inflammatory responses (Dandekar and Perlman, 2005; Queiroz et al., 2022).
To delve into immunogenetic parameters and pinpoint specific genetic variants in the immune system, the human leukocyte antigen (HLA) genetic test is employed. HLA molecules are integral in regulating immune responses and are categorized into classes I and II (Bjorkman et al., 1987). Class I genes are primarily expressed by somatic and immune cells, while class II genes are expressed by B cells, activated T cells, macrophages, and DCs. Investigations into HLA alleles in the MIS-C context aim to uncover potentially hazardous alleles in affected children (Dandekar and Perlman, 2005).
In broader terms, immunogenetics refers to the molecular and genetic exploration of immune responses, encompassing the study of genetic factors influencing tissue compatibility, intraspecies variation, immunity, and tissue antigen inheritance (Martin and Carrington, 2005). Genetic conditions that disrupt the development or function of immune system components render individuals susceptible to autoimmune disorders or hinder their ability to combat infectious pathogens and even cancer, making them significant indicators of genetic disease progression (McCoy et al., 2020).
In this context, certain reports have suggested that MIS-C may manifest as a delayed immune-mediated response to the coronavirus (Jackson et al., 2023). Notably, most COVID-19-infected individuals develop antibodies against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which can be detected by assessing the level of viral RNA (Whittaker et al., 2020). These children, however, exhibit a distinctive serological profile characterized by the presence of Anti-S Antibodies, while Anti-N Antibodies have not been observed. In contrast, children with COVID-19 typically exhibit both Anti-S and Anti-N Antibodies (Weisberg et al., 2020). Furthermore, fewer than one-third of MIS-C patients exhibit detectable viral RNA, suggesting that MIS-C may arise from an aberrant immune response, particularly involving the T-helper 17 pathway, during the convalescent phase of COVID-19 (Patel et al., 2023; Weisberg et al., 2020).
Broadly, COVID-19 gains cellular entry through the binding of the angiotensin-converting enzyme 2 (ACE-2) to the receptor binding domain, facilitated by transmembrane serine protease type 2 (TMPRSS2), which cleaves the spike protein (S) (Deng et al., 2021). This cleavage enables viral entry into host cells and aids the virus in evading the immune system (Shang et al., 2020). Notably, individuals exhibit variations in cellular ACE-2 expression due to DNA ACE-2 polymorphisms described in human populations (Deng et al., 2021). These DNA ACE-2 polymorphisms may influence an individual's susceptibility to COVID-19 infection and the outcomes of the disease (Deng et al., 2021; Shang et al., 2020).
The molecules responsible for viral entry into cells exhibit genetic disparities that can lead to diverse responses among individuals. Numerous studies suggest the existence of genetic variations in the response to SARS-CoV-2 among different genders, races, and specific populations (Deng et al., 2021; Shang et al., 2020). The first study employing Genome-Wide Association Studies (GWAS) is a valuable scientific approach for identifying genetic variants associated with certain infectious diseases, including COVID-19 (Hou et al., 2020).
There remains much to be uncovered about the epidemiology, pathogenesis, clinical spectrum, and long-term consequences of pediatric inflammatory multisystem syndrome. In this review, we critically assess and consolidate the existing evidence, providing insights into current clinical practices and outlining implications for early diagnosis and stabilization, and the appropriate management of genetic susceptibility in the context of COVID-19 within pediatric multisystem inflammation.
COVID-19 Pathogenesis in Pediatric
As previously reported, the occurrence of COVID-19 infection in pediatric is less than in adults and they have milder symptoms, and several genes are involved in the intensity and weakness of COVID-19, which we will refer to later (Hou et al., 2020).
In the meantime, there can be a difference in the expression level of the ACE-2 gene in children and adults (Hou et al., 2020), or ACE-2 receptors are copiously expressed in differentiated ciliated epithelial cells, or even in pediatric. ACE-2 gene is less expressed in the alveolar cell epithelium; therefore, compared to adults, pediatric provide a qualitatively different response to COV-19 (Saule et al., 2006). Viral components usually enter through the apical side to the epithelial cells of the alveolar area and cause them to disappear, macrophages, epithelial cells, alveolar cells, and DCs intervene in the innate immune response. Also, the T cell response to SARS-CoV-2 is initiated by antigen presentation through DCs and then macrophages (Fujimoto et al., 2000).
Apoptotic epithelial cells infected with the virus can also be presented to the T cells. Following infection with COVID-19, there is a meaningful increment in the plasma concentration of proinflammatory cytokines, such as interleukin 10 and 6 (IL-10, IL-6), granulocyte colony-stimulating factor, monocyte chemoattractant protein 1 (MCP1), tumor necrosis factor α, and macrophage inflammatory protein 1-α (MIP1-α). In addition to IL-6, infected lung epithelial cells also generate IL-8, which is an attractant chemical for T lymphocyte cells and neutrophils, and the neutrophils that have been recruited cause the lung to suffer from infection-related damage (Saule et al., 2006).
COVID-19 Pathogenesis in Pediatric with Multisystem Inflammation: Clinical Evidence
Severe infection in pediatric with COVID-19 occurs more in children who have comorbidities or rare diseases (Shekerdemian et al., 2020). In this regard, MIS-C, which was a rare disorder in late April 2020, has been identified as a new medical issue in children, tentatively related to community-based COVID-19 activity, and many reports were rapidly published worldwide (Shekerdemian et al., 2020).
As far as MIS-C is a multisystem inflammatory syndrome concerned pediatric, who present with persistent fever, gastrointestinal symptoms, and mucocutaneous symptoms with rapid progression to cardiac shock and multisystem involvement. The incidence is unknown because it is rapidly evolving during a pandemic (Shekerdemian et al., 2020). Moreover, England included 58 cases, Switzerland and France 35 cases, some series including 30 cases and 17 cases and, 168 cases were reported across the United States (Whittaker et al., 2020). Minority populations are disproportionately affected in reported cases of MIS-C. For instance, East Indian children accounted for approximately 70% of the cases in the United Kingdom case series, while Spanish or Hispanic children constituted about 50% of the cases in the USA case series (Kaushik et al., 2020).
To reach these pandemic reports, laboratory methods have been used for assigning the MIS-C diagnosis. Therefore, some tests recommended have been mentioned here: COVID ELISA serology testing, COVID-19 molecular test, pharyngeal swab, pulmonary infection polymerase chain reaction (PCR) assessment, blood culture if sepsis suspected, CBC with differential, troponin, the examination of liver function, the analysis of lactate in blood gas, serum Ferritin, CRP, procalcitonin, triglycerides, PT/PTT, Pro BNP, and LDH levels (Wang et al., 2020b). Among these methods, molecular test (PCR) has more accuracy. Usually, results obtained from laboratory methods are compatible with clinical symptoms. In some studies, it was observed that clinical manifestations in pediatric were similar to previous reports and all the pediatric had significantly increased inflammatory markers; echocardiographic findings of cardiac damage, including myocardial systolic dysfunction, were demonstrated in 56% (Belhadjer et al., 2020).
Genetic screening holds paramount importance in the realms of prevention, preventive measures, and information management. It plays a pivotal role in discerning the risk factors contributing to the development of MIS-C, and it can significantly inform treatment decisions for affected patients (Saarenheimo et al., 2021; Souto et al., 2000). In this regard, the study conducted by Janet Chou et al. has illuminated specific methodologies that prove efficacious in genetic screening for pediatric patients with MIS-C. Cutting-edge techniques such as Next-Generation Sequencing, Single-cell RNA sequencing, flow cytometry, and transcriptome analysis offer enhanced capabilities for identifying previously healthy children at risk of developing MIS-C (Chou et al., 2021).
Collectively, it shows that this inflammatory syndrome is not caused by a direct virus invasion, but coincides with the development of acquired immune responses to SARS-CoV-2. Even though data related to cardiovascular involvement with MIS-C and COVID-19 are increasing, in MIS-C, several parameters have a role in cardiovascular probably (Kaushik et al., 2020). Moreover, liver damage was present in most children and one-third of patients had acute kidney damage. In addition to wall thickening of the bowel, ascites, and gallbladder abnormalities were also detected (Wang et al., 2020b). The pathophysiology of MIS-C is believed to be attributed to a hyperimmune response to the virus in genetically susceptible children (Whittaker et al., 2020).
As previously mentioned, MIS-C related to COVID-19 was initially characterized as a Kawasaki-like syndrome. Similar to Kawasaki disease, it has been proposed that MIS-C arises from an abnormal immune response to a pathogen, with COVID-19 being the specific pathogen in this case. The production of IgG antibodies against SARS-CoV-2 was observed in nearly all children (Jones et al., 2020; Kaushik et al., 2020). In addition, specific antibodies for the SARS-COV-2 spike (S) protein, which binds to the cellular receptor for viral entry, have been detected in actively infected patients and in children with mild disease, who have improved.
Antibodies to anti-S can expose neutralizing activity and are currently being pursued as a remedial option for injection into children during severe disease and targeted production in vaccines (Korber et al., 2020). No standard medication dietary has been yet reported for MIS-C and adjacent medications seem to be essential. Several therapeutic approaches were employed through various centers, which include steroids, aspirin, anticoagulant therapies, different immune modulators, and intravenous immunoglobulins (IVIG), which may have similar pathophysiology due to the overlapping features of this disease with Kawasaki disease and may contribute to similar treatments for responders; thereby, IVIG with a high dose and corticosteroids with a low to moderate dose is usually recommended for MIS-C treatment (Sperotto et al., 2021).
Collectively, as mentioned above, it has been found that clinical evidence of its benefits is still unproven; the role of antiviral therapy is unclear and drug selection may depend on physician preference, cytokine test results, and drug availability. These recommendations can be taken much more seriously when they are infected with COVID-19, and we need to be constantly careful about the early diagnosis and treatment of children with MIS-C.
Genetic Susceptibility in Pediatric
Owing to the low prevalence of COVID-19 infection among pediatric, small samples were often tested. Genetic studies of pediatric increase the ability to detect genetic relationships with limited environmental effects; however, according to presentation, GWAS found that some genetic variants, especially in the positions ACTN1, FMN1, MNS1, RSU1 TENM3, ADGRL3, SPRY4, SEMA6D, PDS5B, nuclear factor IA gene (NFIA), and MMP27 loci, play a role in the susceptibility to the infection of COVID-19 (Chamnanphon et al., 2022).
Also, several genes are involved in severe COVID-19, including CCRs, TDGF1, MAPT-AS1, LZTFL1, FYCO1, and IFNAR2; although it was shown in other studies in adults, it is now also seen in pediatric (Horowitz et al., 2022). HLA locus was identified as the target gene, which affects the severity and weakness of COVID-19 due to the presence of HLA types (Littera et al., 2020) and the NFIA binds to a palindromic sequence that is seen in both viral and cellular promoters and the source of adenovirus type 2 replication, and these genes can play a role in the cytokine storm in severe COVID-19. ACE 2, IL10RB, TYK2, and TMPRSS2 have been identified as the target genes.
Pediatric with COVID-19 carried different types of genes that cause interference in interferon (IFN)-1, for example, IFNAR1 effect on the severity of COVID-19 in children with multisystem and IFNAR2 a low-risk allele was mentioned for severe COVID-19 (Pairo-Castineira et al., 2021). TLR7 is an immune receptor that is expressed endosomal in some innate immune cells and detects the single-strand RNA (ssRNA) of viruses such as COVID-19. Also, in a smaller study, whole exome sequencing (WES) genes that interfered with immune regulation were seen, like the X-linked inhibitor of apoptosis (XIAP) gene in the MIS-C, which regulates apoptosis and moderates inflammation and leads to an increase in IL-18, IL-1β, and CXCL-9 (Pairo-Castineira et al., 2021; Thaventhiran et al., 2020b).
TBK1 gene mediates nuclear factor kappa B activation and is a known regulator of the interferon pathway, and activates interferon responses in pediatric with COVID-19, and the cytochrome b-245, beta subunit (CYBB) gene, is part of phagocyte NADPH oxidase and interferes with the cytotoxic responses of neutrophil in MIS-C (Pairo-Castineira et al., 2021; Schmidt et al., 2021). MIS-C with COVID-19 is affected by proinflammatory cytokine storm syndrome (CSS).
Dysregulation of the inflammatory response in children afflicted with SARS-CoV-2 infection is a pivotal factor contributing to the development of MIS-C (Nakra et al., 2020). This dysregulation results in varied responses to different forms of immune modulation (McArdle et al., 2021). Notably, the disruption of the synthesis and reduced functionality of IFN I and III, crucial for viral clearance, have been associated with this disease (Park and Iwasaki, 2020).
Conversely, when there is a temporal gap between SARS-CoV-2 infection and the onset of MIS-C symptoms (typically occurring ∼4–6 weeks later), and IVIG prove clinically effective in treatment, the adaptive immune system becomes implicated in the disease's pathogenesis (Blanco-Melo et al., 2020; Rowley, 2020). In these cases, the levels of T CD4+ cells in affected children are notably reduced, while the population of senescent T cells is elevated. This suggests that a defective T cell response may play a role in MIS-C pathogenesis (Consiglio et al., 2020).
Furthermore, when IFN-γ, IL-6, and IL-10 levels surge, it triggers a cytokine storm, a phenomenon linked to the development of MIS-C in pediatric patients. It is theorized that the heightened T cell levels observed in these children could be attributed to both an initial response to cell death and a secondary T cell-mediated immune response amplifying cytokine production (Sun et al., 2020). In chronic or severe disease cases, when the intensity of innate immune responses escalates, the severity of the disease tends to increase in individuals infected with SARS-CoV-2 (Read et al., 2021). This proinflammatory reaction subsequently culminates in thrombosis within the small vessels of the lungs, contributing to lung failure (Matricardi et al., 2020; Stasi et al., 2020).
The genes involved in this process are known to a large extent, for example, the AP321 gene is involved in vesicle biogenesis, and the UNC13D gene plays a role in the maturation and binding of cytolytic vesicle that both genes were enriched in individuals with higher serum cytokine levels (Luo et al., 2021).
In pediatric cases, including infants, the identification of a homozygous nonsense LYST mutation in the PGLY1675 gene, induced by SARS-CoV-2, has been observed. This mutation regulates the size of cytolytic vesicles and responds to IL-1 blockade. Furthermore, observations in pediatric patients with multisystem involvement have shown that the STX11 gene is responsible for regulating the membrane fusion of cytolytic vesicles. This gene also plays a significant role in IL-1 blockade (Vagrecha et al., 2021). In a study focusing on a segment of the gene in pediatric and children with MIS-C, Henderson et al. identified mutations in the CSS genes, highlighting the importance of recognizing children at risk for severe COVID-19 infection and the need for targeted treatment (Henderson et al., 2020).
Genetic Susceptibility in Pediatric with Multisystem Inflammatory Disorders
Epigenetic mechanisms are pivotal in regulating gene expression levels, contributing significantly to differentiation, cellular identity maintenance, and embryonic development. The epigenome is highly sensitive to environmental factors such as chemical pollutants, nutrition, temperature fluctuations, exercise, and early traumatic experiences (Feil and Fraga, 2012). These mechanisms encompass histone tail modifications, noncoding RNA interventions, and DNA methylation, which modulate gene expression without altering the underlying DNA sequence. They also play critical roles in physiological processes, cellular identity maintenance, embryonic development, and differentiation (Cassidy and Charalambous, 2018).
Consequently, the optimal expression of imprinted genes in the placenta is essential for fetal development (Green et al., 2015). Moreover, there appears to be a gender-specific interaction within the maternal-placental-fetal axis that exerts influences on both the fetus and the mother through genetic and epigenetic mechanisms (Hebert and Myatt, 2021). Epigenetic mechanisms can thus be instrumental in shaping gender- and age-specific relationships (Naumova et al., 2013). In addition, there is evidence indicating that drugs may elicit different responses in males and females due to biological disparities, potentially driven by sex-specific gene expression resulting from sex-specific epigenetic modifications (Flanagan et al., 2017).
Genetic counseling centers offer a valuable avenue for identifying individuals requiring genetic evaluation and tailored treatment management (Muramatsu et al., 2017). Knowledgeable genetic counselors can obtain family histories and provide comprehensive discussions encompassing clinical manifestations, genetic inheritance patterns, testing options, and implications for other family members (Ghemlas et al., 2015; Keel et al., 2016; Zhang et al., 2015).
Many diseases exhibit distinct sensitivities between males and females. Generally, the female immune system demonstrates a more robust response to pathogens, although potentially leading to overreactive immune responses and a higher prevalence of autoimmune diseases in women. Females also tend to exhibit stronger responses to antibodies (Ghosh and Klein, 2017). In fact, women have demonstrated higher innate resistance to infections during early life stages (Klein and Flanagan, 2016). Most differences in immune responses between genders are attributed to sex chromosomes rather than hormonal status (Libert et al., 2010).
Gender holds equal importance to age and environmental factors (intrinsic), all of which have the potential to modulate the risk of developing complex diseases (Oertelt-Prigione and Mariman, 2020). Moreover, environmental factors influencing disease susceptibility in both men and women may also exert effects on epigenetic changes (Jin et al., 2020). Gender differences have proven critical in studying many diseases, largely due to the interplay of hormones and sex chromosomes (Wang et al., 2020a). It is widely believed that variations in immune responses between overweight males and females contribute to differing reactions to infections (Ghosh and Klein, 2017; Lotze et al., 2019).
Given that age, gender, and underlying conditions are the primary risk factors (Organization, 2020), further research is essential to elucidate why some patients exhibit no or mild symptoms, while others experience severe manifestations (Zhou et al., 2020). Genetic risk factors are presumed to affect disease progression (Group, 2020). Although our understanding of host genetic risk factors for pediatric MIS-C remains limited (Rodriguez-Smith et al., 2021), it shares certain features with cytokine storm (Crayne et al., 2019). Consequently, it is plausible that MIS-C may have a genetic component that predisposes individuals to the associated CSS. By unraveling these genetic risk factors, we can potentially identify and mitigate symptoms arising from immune pathology caused by CSS. We can tailor treatments to better serve pediatric patients with MIS-C by selecting the right patients and timing.
In this regard, a study conducted in Boston employed Whole Exome Sequencing (WES) on approximately 20 pediatric patients with MIS-C. The findings revealed not only a deficiency in Suppressor of Cytokine Signaling 1 (SOCS1) but also impairments in CYBB and the apoptotic-related gene X-linked Inhibitor of Apoptosis (XIAP). This genetic diagnosis was achieved in 17% of the children. Additionally, an analysis of the transcriptome in unstimulated Peripheral Blood Mononuclear Cells (PBMCs) was conducted (Feldstein et al., 2020; Group, 2020; Mudde et al., 2021; Pairo-Castineira et al., 2021). This examination revealed differential gene expression downstream of signaling pathways associated with the inflammatory response, including interferon signaling type I, oncostatin M, nuclear factor κB, and IL-18.
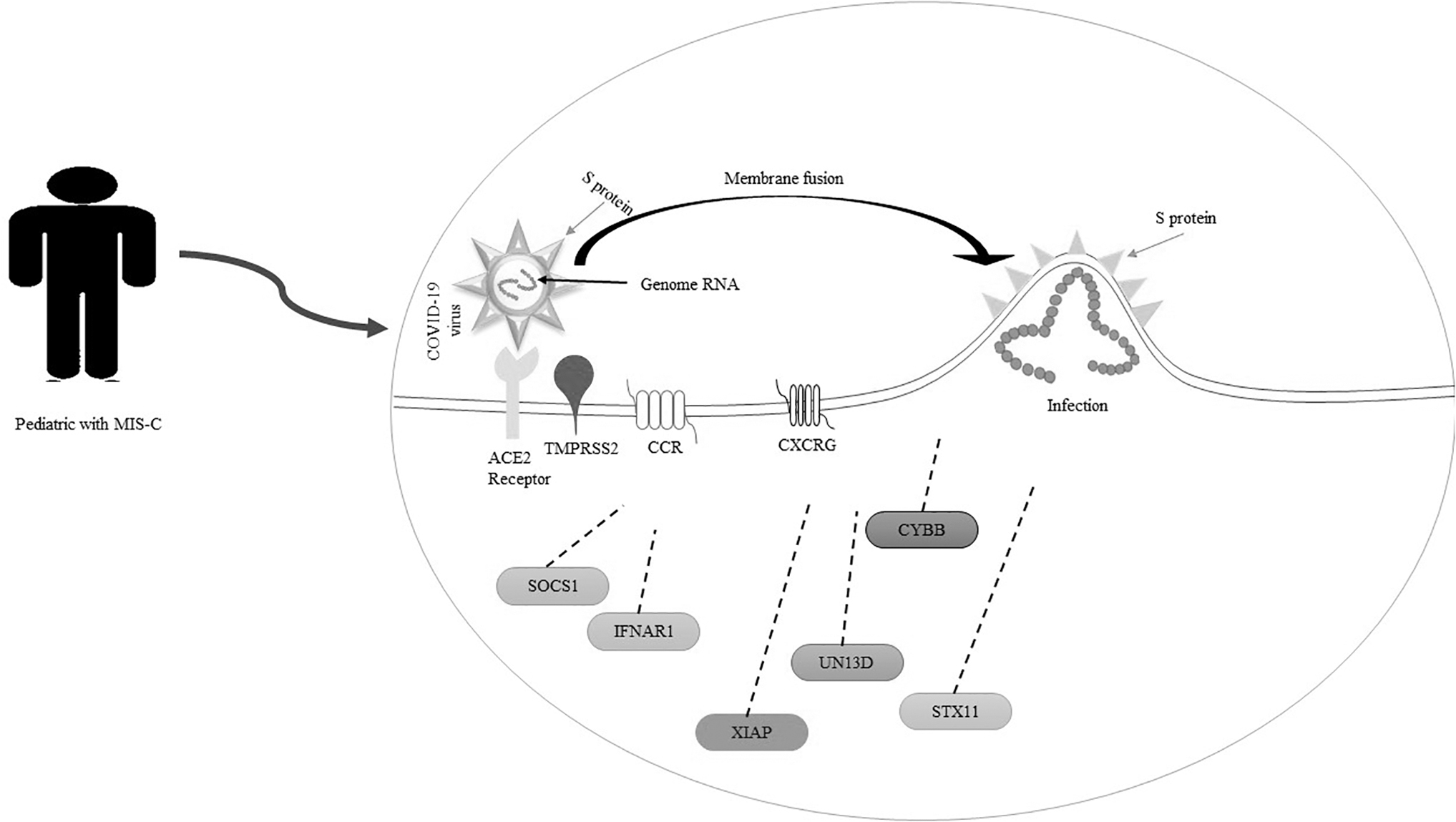
In children who recovered and did not undergo genetic screening for MIS-C, no increase in interferon or inflammatory gene expression was observed without stimulation PBMCs. This is in contrast to the robust activation of immune cells as a suitable index of active MIS-C could demonstrate by sequencing of RNA in PBMCs from children with MIS-C, notwithstanding the absence of any detectable molecular susceptible parameter (Thaventhiran et al., 2020b). In comparison to normal cells, patients with MIS-C showed expansion of variously expressed genes that enhance the signaling of IFNI in T lymphocytes (CD4+ and CD8+), NK cells, and CD14+CD16+ monocytes; therefore, pathways adjusted in PBMCs from recovered and genetically predisposed children converge with pathways upregulated in MIS-C disease (Lee et al., 2020) (Fig. 1).
Gene effects on COVID-19 severity in pediatric with MIS-C. Pursuant to GWAS, genes were reported in pediatric, which play a role in the susceptibility and severity of COVID-19 infection. These genes displayed in figure (CCRs, CXCR, SOCS1, XIAP, IFNAR1, CYBB, UN13D, and STX11) are effective in the severity and susceptibility of COVID-19 in pediatric with MIS-C. It has been shown that CCRs play a more important role. COVID-19, coronavirus disease; CYBB, cytochrome b-245, beta subunit; GWAS, genome-wide association studies; MIS-C, multisystem inflammatory syndrome in children; SOCS1, suppressor of cytokine signaling 1; XIAP, X-linked inhibitor of apoptosis.
Mutations in the XIAP gene have a significant impact on patients, as they disrupt the function of the hemizygous gene, rendering individuals susceptible to CSS and hemophagocytic lymphohistiocytosis (Marsh et al., 2010). This disruption in gene function leads to aberrant inflammatory signaling, potentially increasing the risk of developing MIS-C (Sweeny et al., 2021).
Similarly, mutations in the SOCS1 gene can have consequences due to reduced inhibition of Janus-activated kinases, resulting in elevated interferon tonic signaling, both type I and type II, in unstimulated PBMCs (Meda Spaccamela et al., 2019; Thaventhiran et al., 2020a; Wada et al., 2014). In a related context, some patients with mutations in the CYBB gene have been diagnosed with chronic granulomatous disease, and many of them have experienced CSS in conjunction with infections (Dinauer, 2018; Meda Spaccamela et al., 2019; Meissner et al., 2010). Consequently, mutations in these genes are likely to exert a more pronounced impact on the pediatric population affected by MIS-C.
Collectively, it has been found that pediatric with immunodeficiency or autoinflammation are at greater risk of infection with COVID-19 and different degrees of immunosuppression may conduct to determine the medical consequences from COVID-19 infection. In addition, the findings show that MIS-C could represent a serious disorder of immune imbalance (Lee et al., 2020).
Genetic Susceptibility Foot-Printing in the Intensity of COVID-19 Infection in Pediatric with Multisystem Inflammation: Decipher a Mystery
It has been found that HLAs are one of the proteins with the highest polymorphic state that provide an important function in adaptive immunity.
The proteins encoded by the HLA genes are primarily located on the surface of the body's cells. These unique HLA proteins serve as crucial markers that the immune system relies on to differentiate between self and nonself cells. In the context of multisystem diseases, HLA plays a pivotal role in assisting the immune system in distinguishing between the body's proteins and those produced by foreign invaders, such as viruses and bacteria (Kim et al., 1994).
Several immune activation markers become prominent during the acute stage of this disease. High expression of HLA-DR, along with the presence of CD4+ CCR7+ T cells and elevated CD64 expression on specific immune cells, such as neutrophils and monocytes, indicates the activation of this population of immune cells. Notably, it is well documented that patients with severe COVID-19 often exhibit immune dysregulation characterized by low HLA-DR expression, a phenomenon mediated by IL-6 (Kim et al., 1994).
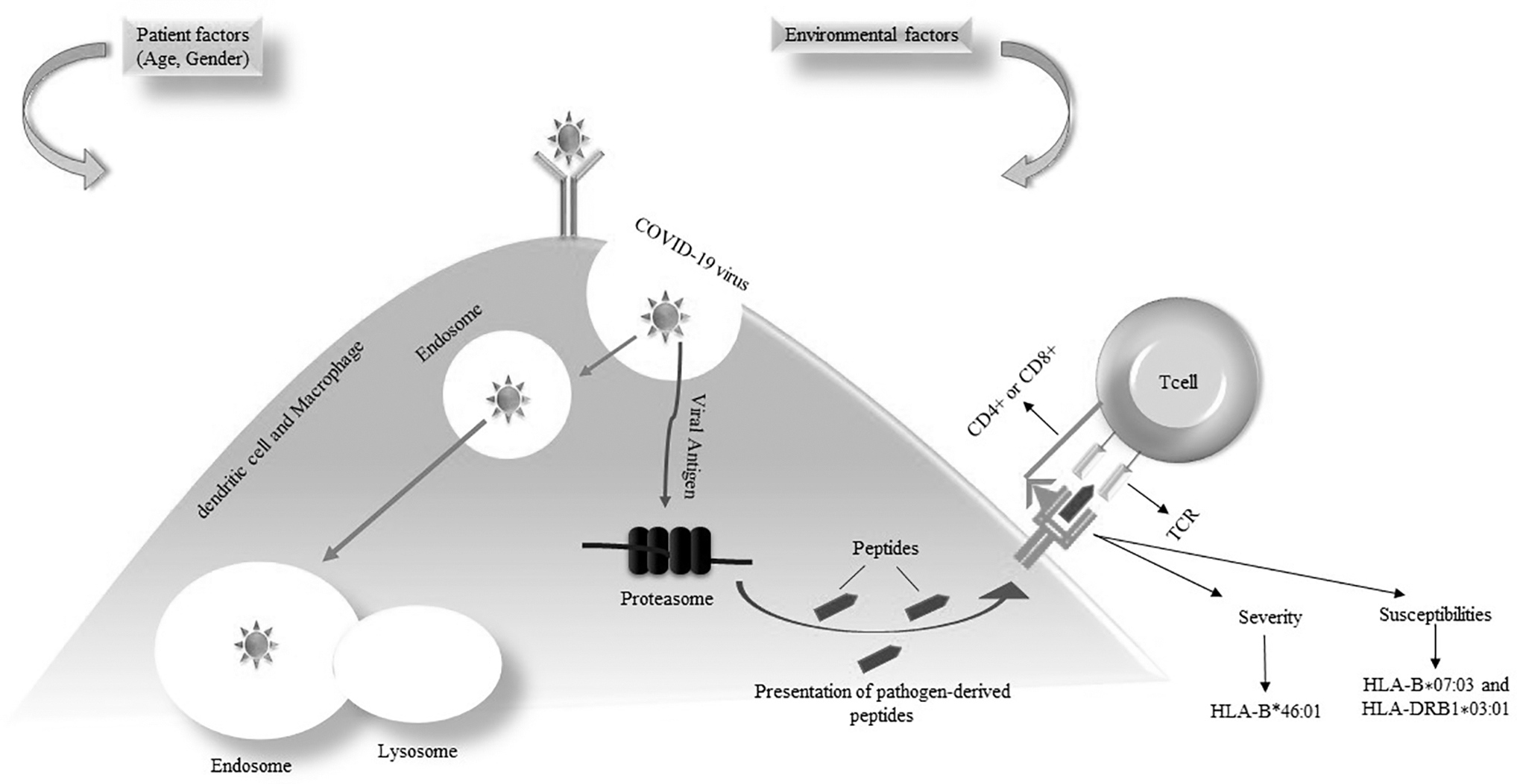
HLA can present peptides derived from pathogens to T cells and trigger immune feedback against the targets. Some studies show the HLA-B*46:01 allele is related to the severity of COVID-19 in a computational simulation by the complete genome of COVID-19, while the HLA-DRB1* 03:01 and HLA-B* 07:03 alleles are linked to susceptibilities to COVID-19 (Ng et al., 2004) (Fig. 2).
Immune response in genetic susceptibility with MIS-C Pediatric. When the COVID-19 virus enters the cell, HLAs play a role in the functioning of the immune system, presenting derived peptides on the cell surface, then being identified by T lymphocytes and causing an immune response against the pathogen. HLAs, human leukocyte antigens.
Moreover, investigations into HLA class I and class II alleles have been conducted in samples from individuals with MIS-C. These studies have unveiled intriguing findings, particularly in HLA class I alleles, where three primary genotypes—A02, B35, and C04—have been associated with an increased risk of MIS-C (Mazer et al., 2022a; Sacco et al., 2022). Similarly, within HLA class II, risk alleles DRB115:01 and DQB1*06:02 have been observed in children with SARS-CoV-2 infection (Valentini et al., 2021b). Consequently, the connection between MIS-C and the presence of these specific alleles underscores their role in genetic susceptibility and the development of MIS-C symptoms (Porritt et al., 2021).
As mentioned earlier, MIS-C is mediated by an aberrant immune response involving Th17 responses during the recovery phase of COVID-19. Additionally, a genetic variant of FCgR, HLA, and antibody-dependent enhancement contributes to excessive inflammation, affecting both Th17 and Treg pathways. Regulatory T cells (Tregs), crucial for maintaining environmental tolerance, preventing autoimmune diseases, and limiting chronic inflammatory conditions, play a key role in this process.
Studies have shown that risk elements related to genetics could affect the therapeutic function of COVID-19. It has been shown that TMPRSS-2 and DNA ACE-2 polymorphisms are forcefully related to the intensity, susceptibility, and clinical outcomes of COVID-19 (Hou et al., 2020). Since gender and age group are involved in causing differences in mortality and infection rate, the difference in the severity of the disease in children and the elderly can be observed completely, which can be due to different genetic particles such as TMPRSS2 (Hou et al., 2020). Also, little information is available about the children's population; thus, we are generally explaining people with COVID-19 in this section. According to the findings, elderly men who have underlying diseases are the most vulnerable groups.
SARS-COV-2 has a very powerful relationship with the ACE-2 receptor and it has an important role to enter the cell along with TMTMPRSS-2, men have a higher risk of contracting severe COVID-19 than women, and men account for more than 50% of mortalities (Tezer and Demirdağ, 2020). In women, the expression level of ACE-2 is higher than in men. The influence of single nucleotide polymorphisms in the TMPRSS2 gene (21q22.3) may play a more significant role in the overall population, particularly from a gender perspective. In this respect, being a receptor for SARS-CoV-2, ACE-2 may also mediate downstream processes following infection, such as inflammatory reactions (Gemmati et al., 2020). Receptors of ACE-2 are found throughout the body, particularly expressed in the vasculature, lung, intestine, testis, brain, and kidney highly.
To enter the cell, COVID-19 binds to ACE-2 receptors through spike protein and ACE-2 receptors utilize different methods to reduce the adverse effects of angiotensin II (Heurich et al., 2014). Initially, viruses could cleave angiotensin II and decrease its harmful exposure, and then, the virus exerts antiregulatory effects on angiotensin II by producing angiotensin. Multiple circumstances such as hypertension, elderly people, diabetes, heart failure, and genetics could cause a lack of ACE-2. According to the above information, ACE-2 deficiency plays an essential function in the infection of COVID-19, which contributes to the development of inflammation, genetic susceptibility, and thrombotic operations (Heurich et al., 2014).
Polymorphism in the single nucleotide of ACE-2 is related to various diseases; thus, these polymorphisms could affect mRNA levels, which results in the intensity of the disease; in addition, COVID-19 is pertinent to cytokine storm state, further inflammatory cytokines and chemokines and mediators are produced, in which many organs are injured. Because of this, the cytokine storm response was demonstrated positive in ACE-2 (Gemmati et al., 2020). Therefore, genetic polymorphism with ACE-2 in inflammatory mediators and the genes responsible for the synthesis of the cytokine cause different responses to COVID-19.
As the gene located on the X chromosome encodes ACE-2, it can be inferred that females expressing this allele may play a determinant role. Such individuals experience fewer side effects than those infected with COVID-19. Consequently, this genetic diversity contributes to variations in the severity, susceptibility, and gender differences observed among patients with COVID-19 in different racial groups (Beyerstedt et al., 2021). In this respect, in another study, it was shown that the transcriptional changes of TMPRSS-2 and ACE-2 are related to the consequences of SARS-COV-2 and not to the molecular predisposition to cause severe symptoms of COVID-19 (Beyerstedt et al., 2021; Heurich et al., 2014).
Some studies of the identified main genes are required to recognize the approaches by which these genes affect hospitalizations related to COVID-19, thereby linking host genetic variation with symptom profiles and laboratory characteristics (Pairo-Castineira et al., 2021). On the other hand, in some studies conducted in Brazil, it was reported that in their group of MIS-C patients, a clear male predominance (68.7%) was found (Beyerstedt et al., 2021). A male gender bias was also evident for hospitalizations and deaths due to COVID-19 compared to females, and it has been reported that female patients have stronger T cell activation during SARS-CoV-2 infection and male patients have higher plasma levels of innate immune cytokines (Dandekar and Perlman, 2005).
It has been considered that some singular variants that were clinically silenced before to COVID-19 can mitigate a less effective immune response to infection or stimulate an inflammatory reaction or a delayed proimmune response to COVID-19, accounting for susceptibility to infection MIS-C. Furthermore, HLA class I and II were investigated in MIS-C patients. In terms of class I alleles, the risk genotypes A02, B35, and C04 were identified in 62.5% of patients (Mazer et al., 2022b). Regarding HLA class II, the risk alleles DQB106:02 and DRB1*15:01, associated with pediatric COVID-19 infection, were predicted in 31.2% and 50% of patients, respectively (Valentini et al., 2021a). In total, Whole Exome Sequencing (WES) data predicted HLA alleles from MIS-C patients, providing the potential to identify at least one risk allele in all patients (100%).
The modulation of some laboratory or clinical results in this study was completely different from that introduced in large-scale nongenetic research, such as a higher proportion of thrombocytosis and coronary artery dilatation (Lee et al., 2020; Mazer et al., 2022b). This could be due to the low sample scale or one of the characteristics of the Latina population. With the tests that were performed, they found that about 30% of 60 children with MIS-C had symptoms of coronary artery dilatation (Lima-Setta et al., 2021a). In addition, patients with coronary changes (all of them were admitted to the Intensive Care Unit) had thrombocytosis, which can be addressed to an inflammatory involvement of the vascular endothelium; therefore, the inclusion of high-intensity ICU pediatric may have caused an overestimation of thrombocytosis.
Numerous studies have consistently identified the most prevalent clinical laboratory findings during the high-risk stage of MIS-C as elevated thrombocytosis and coronary artery dilation, both of which may be linked to inflammation of the vascular endothelium (Lima-Setta et al., 2021b). It is important to note that environmental and genetic factors influence thrombosis risk. While our understanding of the relative significance of genetic factors in thrombosis risk is limited, several genes with varying effects contribute to an individual's susceptibility to thrombosis, with genetic defects amplifying the risk (Lane et al., 1996; Rosendaal et al., 1997). Recent advancements in statistical genetics have enabled researchers to assess the extent of genetic influences on thrombosis and to evaluate the impact of specific genes on risk factors and disease development (Williams et al., 1999).
In this respect, this review article provides evidence for recent views that genetic factors can be pivotal for MIS-C. More research on larger cohorts should be performed to identify genetic risk factors for MIS-C; thus, the risk of MIS-C can be distinguished in various genetic elements of autoinflammation. Furthermore, the lack of common variants in different studies could be mainly due to the poverty of variants, the small number of studies focusing on the genetic susceptibility of the host to the MIS-C, and the differences related to the selection of patients and experimental design (Table 1).
Genes Implicated in Pediatric, Coronavirus Disease and Multisystem Inflammatory Syndrome in Children Severity and Susceptibility
ACE-2, angiotensin-converting enzyme-2; COVID-19, coronavirus disease; CYBB, Cytochrome b-245, beta subunit; HLA, human leukocyte antigen; TMPRSS2, transmembrane serine protease type 2; IL-1, interleukin-1; MIS-C, multisystem inflammatory syndrome in children; NFκB, nuclear factor kappa B; NFIA, nuclear factor IA gene; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SOCS1, suppressor of cytokine signaling 1; ssRNA, single-strand RNA; XIAP, X-linked inhibitor of apoptosis.
Conclusion
In conclusion, the global COVID-19 pandemic has had far-reaching economic and social consequences. While children generally experience milder cases of the disease, the emergence of MIS-C has highlighted the need for dedicated care and hospitalization in pediatric cases. Genomic studies have unveiled a link between the susceptibility and severity of COVID-19 infection and MIS-C. Specifically, the interaction between ACE-2 levels and COVID-19 susceptibility has been identified as a critical factor. ACE-2 plays a pivotal role in the outcomes of COVID-19, and genetic polymorphisms in the ACE-2 gene have been associated with increased susceptibility to COVID-19 infection, facilitated by TMPRSS2.
Furthermore, the intensity of the immune response, particularly in relation to HLA polymorphisms, has been observed to vary among pediatric patients with MIS-C, who are infected with COVID-19. WES data have indicated that children with multisystem involvement typically possess at least one risky HLA allele. These genetic predispositions result in varying degrees of immune response intensity.
Although our knowledge of host genetic susceptibility to MIS-C is still limited, the findings of this study underscore the importance of identifying genetic susceptibility factors in pediatric patients and emphasize the necessity of COVID-19 prevention measures in children. Given the multisystem nature of MIS-C, a multidisciplinary approach is crucial for its diagnosis and treatment.
Moving forward, efforts should be concentrated on identifying additional genetic susceptibility factors in pediatric cases of multisystem inflammatory disorders. Moreover, future research should focus on drug development and therapeutic discovery to better manage and treat these conditions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the Medical Research Program of Zhejiang Province, China (Grant No. 2018KY214).