
Abstract
Coronavirus disease 2019 (COVID-19), the illness caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged in late 2019 and spread very quickly across the world. Different responses to infections have been related to fragment crystallizable gamma-receptor II alpha (FcγRIIA) polymorphisms. The purpose of this investigation was to determine if FCγRIIA rs1801274 polymorphism was related to COVID-19 mortality among different variants of SARS-CoV-2. The FCγRIIA rs1801274 polymorphism was genotyped using the polymerase chain reaction-restriction fragment length polymorphism technique in 1,734 recovered and 1,450 deceased patients. Deceased patients had significantly higher minor allele frequency of the FCγRIIA rs1801274 G allele than in the recovered cases. The COVID-19 mortality was associated with FCγRIIA rs1801274 GG and AG genotypes in the Delta variant and with FCγRIIA rs1801274 GG genotypes in the Alpha and Omicron BA.5 variants. The reverse transcription-quantitative polymerase chain reaction Ct values revealed statistically significant differences between individuals with a G allele and those with an A allele. In conclusion, among the several SARS-CoV-2 variants, there may be a correlation between the mortality rate of COVID-19 and the G allele of FCγRIIA rs1801274. To confirm our findings, thorough research is still required.
Introduction
Coronavirus disease 2019 (COVID-19) can spread from person to person and is caused by a new coronavirus, called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). COVID-19 patients usually have fatigue, diarrhea, conjunctivitis, malaise, fever, and dry cough (Han et al., 2023). Globally, as of October 12, 2023, there have been 771,191,203 confirmed cases of COVID-19, including 6,961,014 deaths, reported to World Health Organization (WHO). According to WHO, the most severely affected regions are Southeast Asia, Africa, Europe, America, Eastern Mediterranean, and Western Pacific (Perveen et al., 2023). There are several SARS-CoV-2 variants with mutations in the viral structural proteins.
According to the Centers for Disease Control and Prevention (CDC) guideline, these variants are classified into variants of concern (VOC) and variants of interest (VOI) (Centers for Disease Control and Prevention, 2021). VOI encompasses Epsilon, Zeta, Eta, Theta, Iota, and Kappa variants, whereas VOC includes Alpha, Beta, Gamma, and Delta variants. The Omicron, a novel variant with 32 mutations in the spike protein alone, has recently been classified as a VOC. These variants either demonstrate a higher infection rate or facilitate it for the virus to replicate in the host cell due to particular changes in structural proteins (Cascella et al., 2023; Liu et al., 2022).
It is widely known that host genetic variants influence the immunological response of individuals infected with SARS-CoV-2. Host genetic factors may affect the susceptibility and severity of various infectious diseases and their clinical manifestation by selecting good candidate genes based on prior knowledge about the disease's pathophysiology and phenotype (Di Maria et al., 2020).
Assessing innate immune response and humoral immunity is one of the most useful approaches to determining the severity and prognosis of COVID-19 (Farag et al., 2020). Natural killer cells, macrophages, eosinophils, neutrophils, mast cells, and platelets are just a few immune cells with a protein, known as the fragment crystallizable (Fc) receptor, on their surface. The protein plays a vital role in inflammatory and infectious diseases. There are three families of Fc receptors for IgG (FcγRs), including FcγI, FcγIIa/b, and FcγIIIa/b, which are attached to the Fc domain of IgG already bound to the infected cells. Accordingly, infectious agents are killed by cytotoxic or phagocytic cells or by antibody-dependent cell-mediated cytotoxicity (ADCC) (Patel et al., 2019).
Human Fc gamma-receptor II alpha (FcγRIIA) is a critical member of the Fc receptor family and is necessary for controlling immunological responses, autoimmune illness, and local inflammation. It also serves as a vital link between the cells of adaptive immunity and humoral immunity. The gene encoding the FcγRIIA receptor has functional single nucleotide polymorphism (SNP) at 131 amino acid (aa) residues with a G to A point mutation, resulting in either arginine or histidine on the Ig-like domain at 131 aa (Hassan and Kadhim, 2022). The polymorphism variation will affect the function of these receptors by interfering with the cells' trafficking and localization, which is linked to the pathophysiology of infectious, autoimmune, and inflammatory diseases (Junker et al., 2020). Environmental cytokines such as interferon-α, interleukin-3 (IL-3), and IL-6, and dexamethasone enhance and decrease the expression of the FcγRIIA gene (Anania et al., 2019).
In this study, we investigated the function of FCγRIIA rs1801274 polymorphism in the risk of developing severe COVID-19 and its effects on mortality in these patients.
Materials and Methods
Sample selection
The study was approved by the Research Ethics Committees of the Islamic Azad University, Shahrood Branch (
During the three COVID-19 infection peaks, which included the Alpha, Delta, and Omicron BA.5 variants, from November 2020 to March 2022, the patients for this retrospective analysis were chosen from the Ilam University of Medical Sciences. Reverse transcription-quantitative polymerase chain reaction (RT-qPCR) analysis was used to detect the SARS-CoV-2 genome from pharyngeal swabs. All RT-qPCR tests were carried out by trained professionals with the same equipment.
Only 3,184 of the 13,227 patients matched the following criteria for inclusion: Submitting consent form before participating in our research, all patients with same ethnic background had no history of vaccination and COVID-19 infection, and without having any comorbid condition such as heart, kidney, liver, and lung disease, pregnancy, and cancer.
In this study, the COVID-19 patients were placed in two groups: Recovered and deceased patients. All clinical parameters were gathered from the electronic medical record system during prehospitalization visits.
Extraction of genomic DNA and genotyping of FCγRIIA rs1801274 polymorphism
The blood samples of infected patients (10 mL) were taken and placed in EDTA tubes. Total DNA was isolated with Yekta Tajhiz DNA extraction kit (YTA, Yekta Tajhiz Azma, Iran).
FCγRIIA rs1801274 polymorphism was genotyped using the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method.
The sense and antisense primers for FCγRIIA rs1801274 polymorphism with the PCR product sizes 366 bp included 5′-CAACAGCCTGACTACCTATTACGCGGG-3′ and 5′-CAACAGCTGGTCACCTATCACCTGAG-3′, respectively (Jiang et al., 1996). The PCR was performed under the following conditions: 94°C for initial denaturation for 7 min, 40 cycles of 94°C for 35 sec, 57°C for 45 sec, 72°C for 35 sec, and 72°C for the final extension for 10 min.
According to the manufacturer's instructions, the PCR products were digested with BstUI restriction enzyme and then visualized by electrophoresis on a 3% agarose gel. After digestion, the product sizes of the AA genotype were 343 and 23 bp, and the GG genotypes were 322 and 44 bp.
Several samples to confirm the RFLP method were randomly selected and sequenced using the Sanger sequencing method. The raw data were then analyzed using ChromasPro software.
Statistical analyses
Using SPSS software, version 22.0 (SPSS, Inc., Chicago, IL), the data were analyzed. Continuous data (numerical variables) were represented as a mean and standard deviation, whereas categorical variables were condensed as a frequency (%).
All normality assumptions of numerical variables were examined using the Shapiro-Wilk test. The Mann–Whitney U test was employed to compare normally distributed continuous variables. Categorical variables were compared using the Chi-square test. The effect of FCγRIIA rs1801274 polymorphism on COVID-19 mortality was evaluated using the area under the receiver operating characteristic curve (AUC-ROC) analysis. All tests were two stailed, and the threshold for significance was fixed at p < 0.05.
The online SNPStats tool was used to determine the inheritance models, Hardy-Weinberg equilibrium (HWE), and the minor allele frequency (MAF) of the chosen variant. Moreover, a 95% confidence interval (CI) and odds ratio (OR) were also computed. The Akaike Information Criterion (AIC) and the Bayesian Information Criterion were used to find the best model (BIC).
Results
Clinical characteristics of the studied patients
Table 1 presents the characteristics of COVID-19 research participants. As shown in this table, 3,184 patients participated in the study, with 1,022 Alpha variants having a mean age of 53.0 ± 12.7 years, 1,026 Delta variants having a mean age of 58.0 ± 11.8 years, and 1,132 Omicron BA.5 variants having a mean age of 53.7 ± 12.9 years. In the Alpha variant, the frequencies of males and females were 479 (46.9%) and 543 (53.1%), respectively. In the Delta variant, their frequency was 546 (53.2%), and it was 546 (53.2%) and 480 (46.8%) in the Omicron BA.5 variant. The Delta variant had a lower mean of 25-hydroxy vitamin D (p = 0.029) than the Alpha and Omicron BA.5 variants, which was statistically significant.
Comparison of Laboratory Parameters Between SARS-CoV-2 Variants
Statistically significant (<0.05).
ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; FBS, fasting blood glucose; FCγRIIA, fragment crystallizable gamma-receptor II alpha; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; qPCR, quantitative polymerase chain reaction; SD, standard deviation; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TG, triglyceride; WBC, white blood cells.
The susceptibility to COVID-19 infection with different variants of SARS-CoV-2 was significantly associated with alanine transaminase (p = 0.001), aspartate transaminase (p < 0.001), alkaline phosphatase (p < 0.001), cholesterol (p < 0.001), low-density lipoprotein (p < 0.001), high-density lipoprotein (p = 0.039), uric acid (p < 0.001), and creatinine (p < 0.001).
Correlation between RT-qPCR Ct values and COVID-19 mortality
The Delta variant had the higher mean RT-qPCR Ct value than the other variants. Delta, Alpha, and Omicron BA.5 had mean RT-qPCR Ct values of 17.4 ± 6.1, 20.1 ± 6.4, and 21.9 ± 6.0, respectively, which was statistically significant (p < 0.001).
The recovered group had a substantially higher observed Ct value (25.7 ± 4.1) than the deceased group (14.1 ± 3.6), which resulted in a difference of 11 cycles between the two groups (25.7 vs. 14.1 cycles). The difference was statistically significant (p < 0.001).
FCγRIIA rs1801274 polymorphism and COVID-19 mortality rate
Compared to patients with other genotypes, those with the FCγRIIA rs1801274 GG genotype had a significantly higher COVID-19 death rate.
Table 2 shows the findings of the inheritance model analysis of the FCγRIIA rs1801274 polymorphism. The best-fitting models for the FCγRIIA rs1801274 polymorphism were the codominant inheritance models, with the lowest AIC and BIC values. The FCγRIIA rs1801274 GG genotype was linked to an increased risk of COVID-19 mortality (p < 0.001, OR: 2.88, 95% CI: 2.34–3.56).
Statistically significant (<0.05).
AIC, Akaike Information Criterion; BIC, Bayesian information criterion; CI, confidence interval; COVID-19, coronavirus disease 2019; OR, odds ratio.
The FCγRIIA rs1801274 polymorphism was incompatible with HWE in both recovered and deceased patients (p < 0.05). The association between FCγRIIA rs1801274 polymorphism with the disease may be because these variants are not found in HWE. In the deceased patients, the MAF for FCγRIIA rs1801274 (G) polymorphism was higher (0.48) compared to the recovered (0.33).
We used logistic regression to create two distinct predictor variables for FCγRIIA rs1801274 genotypes. The AUC-ROC values were 0.758 (OR: 0.758, 95% CI: 0.769–0.801, p < 0.001) and 0.671 (OR: 0.671, 95% CI: 0.652–0.690, p < 0.001) in the presence and absence of FCγRIIA rs1801274 polymorphism, respectively, indicating that host genetic factors are frequently significant for the resolution of viral infection (Fig. 1).
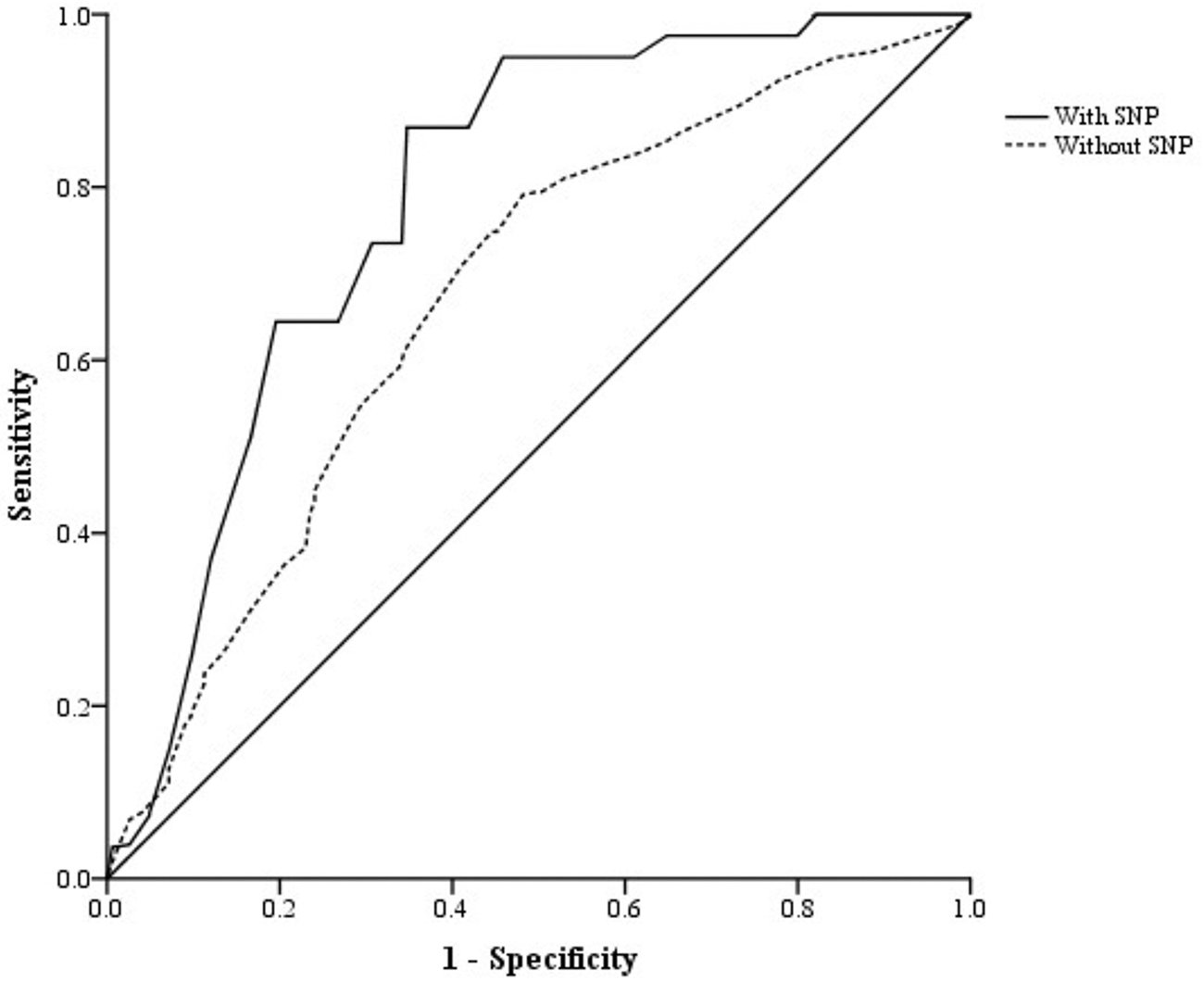
ROC curve for different predictor variable with and without the FCγRIIA rs1801274 genotypes. FCγRIIA, fragment crystallizable gamma-receptor II alpha.
FCγRIIA rs1801274 genotypes and COVID-19 mortality rate adjusted by SARS-CoV-2 variants
SARS-CoV-2 variants were significantly associated with mortality. Omicron BA.5 and Delta variants had low and high mortality rates, respectively (p < 0.001). FCγRIIA rs1801274 AA, AG, and GG genotypes in the Alpha variant were 343 (33.6%), 447 (43.7%), and 232 (22.7%), respectively. The frequencies of FCγRIIA rs1801274 AA, AG, and GG in the Delta variant were 417 (40.6%), 333 (32.5%), and 276 (26.9%), respectively. Moreover, FCγRIIA rs1801274 AA, AG, and GG frequencies in the Omicron BA.5 variant were 530 (46.7%), 474 (41.7%), and 132 (11.6%), respectively.
After adjusting FCγRIIA rs1801274 genotypes with SARS-CoV-2 variants, COVID-19 mortality was associated with FCγRIIA rs1801274 GG (OR: 2.59, 95% CI: 1.85–3.63) and AG (OR: 1.81, 95% CI: 1.33–5.44) in the Delta variant and with FCγRIIA rs1801274 GG (OR: 3.08, 95% CI: 2.17–4.38) in the Alpha and Omicron BA.5 variants (OR: 2.94, 95% CI: 1.97–4.37) (Table 3).
FCγRIIA rs1801274 Polymorphism Association with SARS-CoV-2 Variants
FCγRIIA rs1801274 polymorphism and RT-qPCR Ct value
We evaluated the correlation between viral load and FCγRIIA rs1801274 polymorphism. The RT-qPCR Ct value was used to make a semiquantitative prediction of viral load. The RT-qPCR Ct values performed when the patients' were admitted to the hospital were examined. A higher viral load is probably associated with a lower RT-qPCR Ct value, while a lower viral load is likely to be associated with a higher Ct value.
The RT-qPCR Ct values between individuals with FCγRIIA rs1801274 GG (p < 0.001) and AG genotypes (p = 0.002) and those with the AA genotype were statistically different, as shown in Figure 2, suggesting a possible relationship between the GG genotype and an elevated viral load. The Pearson correlation analysis also showed a tendency for the Ct value to decline when the G allele was present (p = 0.079).
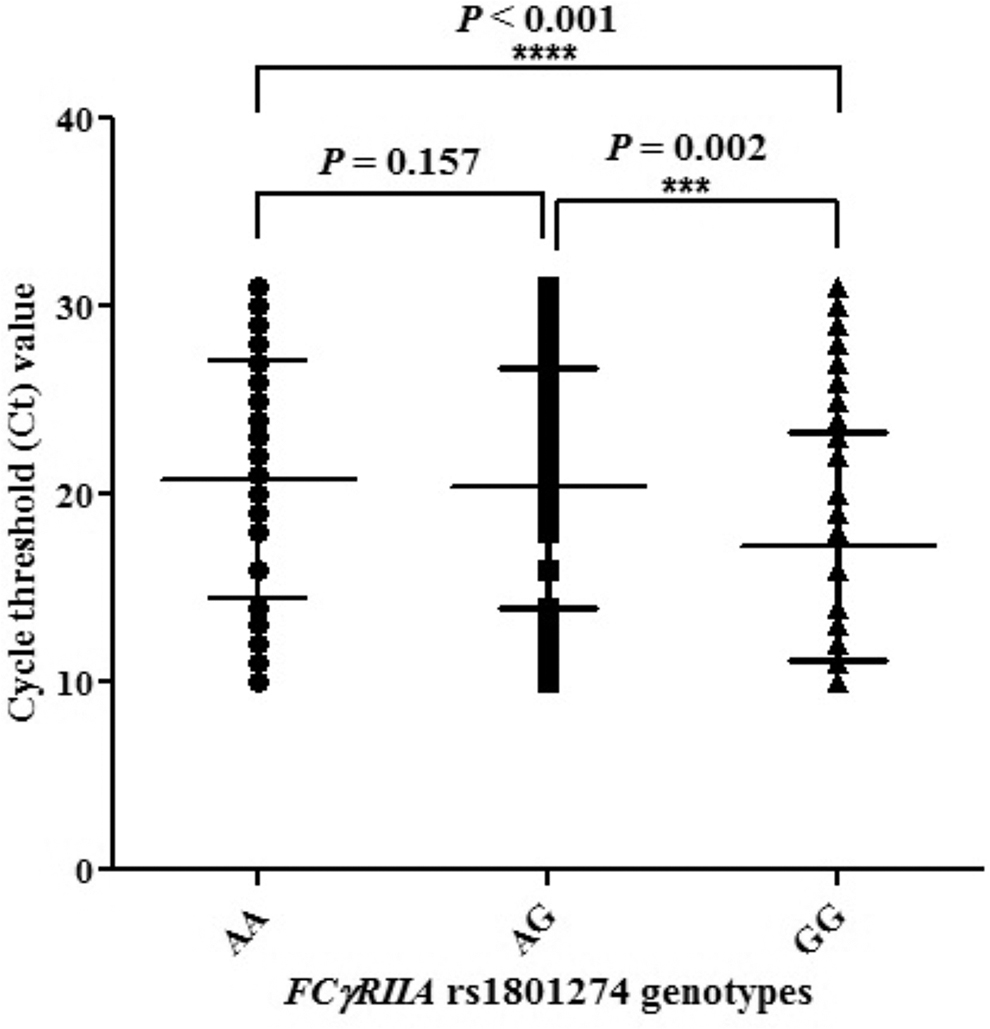
Analysis of PCR Ct values with FCγRIIA rs1801274 genotypes. ***P = 0.002, ****P < 0.001. PCR, polymerase chain reaction.
Discussion
This study revealed a statistically significant correlation between the case mortality rate of COVID-19 and the allele frequency of FCγRIIA rs1801274. To the best of our knowledge, this study was the first research demonstrating a significant relationship between the Iranian's COVID-19 mortality rate and the FCγRIIA rs1801274 SNP.
Throughout the course of human history, numerous viral epidemics have emerged, exerting profound effects on both global health and society. Several widely recognized viruses have been associated with epidemics, including smallpox, Influenza, human immunodeficiency virus-1 (HIV-1), Ebola, SARS-CoV-2, and monkeypox virus (Letafati and Sakhavarz, 2023; Letafati et al., 2023).
According to the findings, the FCγRIIA rs1801274 G allele was linked to a higher risk of COVID-19-related death. In this study, MAF (G-allele) for FCγRIIA rs1801274 was 0.40. According to the SNP database maintained by the National Center for Biotechnology Information (NCBI), the value in other regions was as follows: Asians (0.303), East Asians (0.275), South Asians (0.411), other Asians (0.416), Europeans (0.491), Africans (0.515), African Americans (0.514), and Latin Americans (0.475) (
In comparison to the recovered patients (0.33), the frequency of the FCγRIIA rs1801274 G allele was higher in the deceased ones (0.48). The MAF of rs1801274 showed a strong correlation with the COVID-19 mortality rate (Hassan and Kadhim, 2022; López-Martínez et al., 2022).
The role of host genetic factors in human susceptibility and/or disease progression has been the subject of research for decades (Ahmadi et al., 2022; Albu-Mohammed et al., 2022; Beheshti Shirazi et al., 2022; Khalilzadeh et al., 2022; Mirzaei Gheinari et al., 2022; Raheem Juhi Al-Kaabi et al., 2022; Rahimi et al., 2021; Tavakoli et al., 2022; Tavakoli et al., 2023). In contrast to other human genes, where genetic variations have not clearly influenced how an illness manifests itself, it is well known that the 1q23 locus, where the FcRIIA gene is located, is associated with a variety of infectious and autoimmune diseases. Moreover, there is a clear functional difference between the G and A 131 allele types (called H131R) of the FCγRIIA gene (Sananez et al., 2020).
The FCγRIIA rs1801274 G allele seems to be correlated with the severity of COVID-19. In this study, COVID-19 mortality was associated with FCγRIIA rs1801274 GG and AG genotypes in the Delta variant and with FCγRIIA rs1801274 GG genotype in the Alpha and Omicron BA.5 variants. The Delta variant had the highest mortality rate in this study. In this study, the FCγRIIA rs1801274 G allele was associated with the COVID-19 mortality rate in the Delta variant. The presence of this allele among patients is one of potential reasons for the high mortality of the Delta variant. Further research, however, is required to confirm this hypothesis. It is also indicated that the FCγRIIA rs1801274 GG genotype may be linked to more severe COVID-19, whereas the FCγRIIA rs1801274 AA genotype may be associated with a better prognosis for COVID-19 (Hassan and Kadhim, 2022; López-Martínez et al., 2022).
Compared to receptors encoded by the R 131 (G 131) allele, those by H-131 (A 131) allele exhibit higher affinities for IgG 1, 2, and 3 subtypes. The high binding affinity enhances the phagocytic activity of FCγRIIA-H131 receptors. Accordingly, scientists have investigated the relationship between H131R and its possible role in disease prevention (Bohmwald et al., 2019).
Several studies have investigated the association of this polymorphism with infectious and noninfectious diseases. The first hint that the H131 allele might play a role in immunity to an infectious disease came from comparing the allele frequencies of populations susceptible to malaria in Asia and Europe (Amiah et al., 2020). A significantly higher frequency of FCγRIIA rs1801274 GG genotype is reported in patients infected with the dengue virus, suffering from thrombocytopenia (Alagarasu et al., 2015). Similarly, a Chinese study by Qu et al. (2020) suggested that individuals with the FCγRIIA rs1801274 GG genotype is more likely to develop inhibitors in Hemophilic A patients.
In SARS-CoV-1 patients, compared to the control group, the FCγRIIA rs1801274 GG genotype in the SARS-infected ICU patients was significantly higher (Yuan et al., 2005). As in patients with COVID-19, during the SARS-CoV-1 outbreak, some cases of SARS-CoV-1 patients were successfully treated with plasma from convalescent patients recovered from the SARS infection (Duan et al., 2020; Klassen et al., 2021; Skowronski et al., 2005; Wong et al., 2003). Studies have examined the anti-SARS plasma's ability to neutralize viruses; however, it is still unknown how functionally significant anti-SARS antibodies are or whether they might function through an Fc-dependent receptor (Tan et al., 2004; Traggiai et al., 2004).
It would be beneficial to examine the FcγRIIA genotypes concurrently with the presence/level of antibody to SARS-CoV-1 in these SARS patients since the activation of FcγRIIA is triggered by antibody binding and is followed by numerous biologic processes such as signal transduction, phagocytosis, and ADCC, the release of inflammatory mediators, and interactions with other Fc receptors and complementary factors. Furthermore, FcRIIA genotyping may facilitate predicting the effectiveness of antibody-based immunotherapy (Yuan et al., 2005).
Given that the immune system can potentially cause and contribute to tissue damage, the higher affinity of the FcγRIIA gene may actively cause tissue damage by triggering an aggravated immune response and accelerating the infection process (Hassan and Kadhim, 2022).
The findings indicated the relationship between the RT-qPCR Ct value and COVID-19 mortality, in which a lower RT-qPCR Ct value was linked to a higher risk of death. This relationship has been reported in many studies (Gholemi et al., 2022; Rabaan et al., 2021; Raheem Juhi Al-Kaabi et al., 2022; Rahimi et al., 2021).
The RT-qPCR Ct values showed a statistically significant difference between patients with GG and AG genotypes of FCγRIIA rs1801274 and those with the AA genotype, suggesting the likely relationship between this genotype and an elevated viral load in this study. The severity of the COVID-19 infection appears to be exacerbated by the FCγRIIA rs1801274 G allele by an increase in viral load. The patients with FCγRIIA rs1801274 GG may exhibit a reduced capacity for SARS-CoV-2 clearance, which is related to the defective induction of the inflammatory pathway.
One of the limitations of this study was the use of RT-qPCR Ct value to show the extent of viral load in the samples. Moreover, the sampling time could affect the RT-qPCR Ct value, where some individuals referred to the clinics earlier, while others referred to the clinics later when symptoms became more severe. This was another limitation of the RT-qPCR Ct value. The next limitation of our study was not considering healthy controls and not exanimating the frequency of FCγRIIA rs1801274 genotypes in different Iranian races to confirm the findings.
In conclusion, the FCγRIIA rs1801274 polymorphism was correlated with COVID-19 mortality. The COVID-19 mortality was associated with FCγRIIA rs1801274 GG and AG genotypes in the Delta variant and with FCγRIIA rs1801274 GG genotypes in the Alpha and Omicron BA.5 variants. The RT-qPCR Ct values differed statistically significantly between individuals with a G allele and those with an A allele. It will be critical to establishing whether the FCγRIIA rs1801274 SNP is consistently linked to COVID-19 mortality in the future.
Footnotes
Authors' Contributions
N.M. and F.S.: Performed the experiments and article preparation; I.A. and E.A.: Clinical sample and data acquisition; M.T.G. and S.M.: analyzed data and interpreted data; A.F.: designed and supervised clinical study, interpreted data, and read and approved article. All authors reviewed the article.
Authors' Confirmation Statement
N.M. and M.T.G. are from Islamic Azad University of Shahrood (Shahrood, Iran); S.M., F.S., and A.F. are from Pasteur Institute of Iran (Tehran, Iran); and I.A. and E.A. are from Ilam University of Medical Sciences (Ilam, Iran), all where education and research are the primary functions.
Data Availability Statement
The data generated in this study are present in the main text.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.