
Abstract
Hepatitis B virus (HBV) is a global public health concern, and China continues to face a high burden of HBV cases. Vaccination plays a critical role in controlling and eradicating HBV. However, studies have shown that some individuals may experience waning immunity over time, highlighting the importance of enhanced immunization strategies. This study aimed to investigate the relationship between age, gender, and anti-HBs antibody levels, as well as the prevalence of serum hepatitis B surface antigen (HBsAg)/HBV e antigen (HBeAg) positivity. This retrospective study included 43,609 pediatric patients who visited the outpatient department between January 2013 and December 2022. Serum biomarkers (HBsAg, anti-HBs, HBeAg, anti-HBe, and anti-HBc) were measured using Roche Cobas 8000. There is a significant difference in anti-HBs titer between genders and across different age groups (p < 0.05). The serological markers HBsAg/HBeAg exhibited the highest positivity rate in the age group of 15–18 years. The findings demonstrate a gradual decrease in anti-HBs levels following HBV vaccination. The prevalence of serum markers HBsAg/HBeAg is higher among adolescents aged 15–18 years, which should be a matter of concern and attention.
Introduction
Human hepatitis B virus (HBV) is a double-stranded DNA virus transmitted through blood or bodily fluids. It can cause acute hepatitis, fulminant hepatitis, chronic hepatitiss, cirrhosis, and hepatocellular carcinoma (HCC). Patients with cirrhosis have a 2–5% risk of developing HCC annually (Hadziyannis, 2011; Liver, 2017). The widespread transmission of HBV is a significant global public health issue. China still has a large number of HBV-infected individuals, despite making tremendous efforts in controlling hepatitis diseases (Yue et al., 2022). Recombinant hepatitis B vaccines are the most effective intervention for global control and eradication of hepatitis B. By the end of 2022, infant hepatitis B vaccination had been promoted in 190 countries and made a substantial contribution to reducing the incidence of hepatitis B. On July 18, 2023, the World Health Organization announced that the global coverage with three doses of hepatitis B vaccine is estimated to be at 84%.
In China, since early 1992, the country has implemented a mandatory HBV immunization program (Wang et al., 2014). Since 2006, a free HBV vaccine program for newborns has been implemented, making all infants eligible for basic three-dose HBV vaccination at birth, 1 and 6 months, with each dose containing 5 μg (Kane et al., 2013). Despite these efforts, owing to the large population in China, the absolute number of HBV cases remains high (Liu et al., 2019). Therefore, it is crucial to identify recent trends in the positivity rate of hepatitis B surface antibodies (anti-HBs) and assess the effectiveness of strengthening immunization.
Research on the hepatitis B vaccine and its antibody production has been reported, with some studies coming from China (Doi and Kanto, 2021; Zhu et al., 2021). Several studies have confirmed that after three doses of primary immunization during the neonatal period, the immune protection provided by the hepatitis B vaccine can last for 10–15 years and even exceed 25–30 years (Beran et al., 2016; Bruce et al., 2016; Van Der Meeren et al., 2016). However, a survey of 6,156 high school students who received their first immunization revealed that ∼10–25% lost their immune response to hepatitis B surface antigen (HBsAg) (Lu et al., 2008).
Owing to individual variation in the response to the hepatitis B vaccine, basic immunity in newborns may fail (Su et al., 2007b; Zuckerman, 2006), and over time, the levels of anti-HBs antibodies may decrease or even disappear (McMahon et al., 2005; Poovorawan et al., 2011). Other studies have provided evidence supporting the need for enhanced immunization among adolescents, based on individuals who failed to elicit memory immune responses (Jan et al., 2010; Zhu et al., 2011). It is noteworthy that children who have received the hepatitis B vaccine are generally protected against the virus. However, in rare cases, breakthrough infections can occur because of contact with individuals carrying a high viral load or through exposure to mutant strains of the virus (Jing et al., 2020; Qin and Liao, 2018).
However, there have been no large-scale research reports on this issue in the central region of China over the past 10 years. Therefore, the main focus of this study was to investigate the changes in anti-HBs antibody levels with respect to age and gender, as well as the prevalence of serum markers HBsAg/HBV e antigen (HBeAg).
Materials and Methods
Subjects
In China, the hepatitis B vaccine is administered to children at 0, 1, and 6 months after birth. Vaccinating infants against hepatitis B is not only free but also reduces the risk of contracting the HBV. It is also a mandatory requirement for enrollment in schools, making it an essential prerequisite. Consequently, there is no evasion of vaccination. The first dose of the vaccine is injected within 24 h of newborn delivery, followed by subsequent doses administered by community health centers at 1 and 6 months. Testing for HBsAg and anti-HBs can be requested for reasons such as family curiosity, before higher education internships, or before surgeries. In this study, a retrospective evaluation was conducted on 43,609 patients who visited the pediatric outpatient department between January 2013 and December 2022, and HBsAg and anti-HBs levels were tested. The male-to-female ratio in our study was 2.20:1, which is similar to the higher male population in China. The study population included only children aged 7 months and older who completed the three doses of the hepatitis B vaccination, as the final dose is typically administered at 6 months of age.
We retrieved serum biomarkers (HBsAg, anti-HBs, HBeAg, anti-HBe, and anti-HBc), as well as age and gender, of the study population from the Laboratory Information System database. Information on vaccination history and the presence of HBV-infected individuals among family members was obtained from the Hospital Information System database. A cutoff level of anti-HBs titer ≥10 IU/L is considered as the protective threshold, indicating a response to the vaccine. Lower levels suggest a lack of protection. For patients with multiple anti-HBs titer results at different time intervals, the latest recorded anti-HBs test result was included in the study. All data mentioned previously were sourced from Renmin Hospital of Wuhan University.
Children were divided into five age groups, namely group I to group V, as follows: 7 months < group I ≤ 3 years, 3 years < group II ≤5 years, 5 years < group III ≤10 years, 10 years < group IV ≤15 years and 15 years < group V ≤ 18 years. The seropositivity rate and levels of anti-HBs were compared among these age groups. A positive result for serum markers HBsAg/HBeAg indicates hepatitis B infection. Among these cases, 43,609 cases were selected, which showed only anti-HBs positivity or combined anti-HBs with other antibody markers, for analyzing the relationship between anti-HBs levels, age, and gender. The study received approval from the Ethics Committee of Renmin Hospital of Wuhan University.
Measurements
The measurement of serum biomarkers (HBsAg, anti-HBs, HBeAg, anti-HBe, and anti-HBc) was analyzed using electrochemiluminescence immunoassay on Roche Cobas 8000 (Roche Diagnostics, Indianapolis, IN).
The cutoff index value for HBsAg is 1.1. If the HBsAg level is >1.1 COI, the sample is considered positive; if the HBsAg level is <1.1 COI, the sample is considered negative. The measurement range for anti-HBs is 2–1000 IU/L, and anti-HBs ≥10 IU/L is defined as positive. Samples with anti-HBs ≥1000 IU/L are recorded as 1000 IU/L, whereas samples below the limit of detection (2 IU/L) are recorded as not detectable. The cutoff index value for HBeAg is 1.0. If the HBeAg level is >1.0 COI, the sample is considered positive; if the HBeAg level is <1.0 COI, the sample is considered negative. The cutoff index value for anti-HBe is 1.0. If the anti-HBe level is >1.0 COI, the sample is considered negative; if the anti-HBe level is <1.0 COI, the sample is considered positive.
The cutoff index value for anti-HBc is 1.0. If the anti-HBc level is >1.0 COI, the sample is considered negative; if the anti-HBc level is <1.0 COI, the sample is considered positive. HBsAg is an indicator of probable chronic HBV infection. Its presence in an individual suggests an ongoing infection with the virus. On the contrary, anti-HBc suggests infectious contact with HBV and probable recovery. When an individual has detectable anti-HBc antibodies, it indicates that they have been exposed to the virus at some point, even if they have cleared the infection or are currently in a state of recovery. It is essential to consider both markers when evaluating the status of HBV infection and its implications for individuals, as they provide valuable information about the nature and progression of the disease.
According to a previous study, anti-HBs levels were divided into four groups: (1) nonreactive or negative (<10 IU/L), (2) low responders (10–100 IU/L), (3) moderate responders (100–1000 IU/L), and (4) high responders (>1000 IU/L).
Statistical analysis
Chi-square test was used to compare the frequency and proportion of qualitative data. Owing to the skewed distribution, median and 95% confidence interval were used to represent the anti-HBs levels. Nonparametric test (Kolmogorov–Smirnov Z) was performed to analyze the anti-HBs levels. IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY) and GraphPad Prism 9.5.1 (GraphPad Software, San Diego, CA) statistical software were utilized for plotting and data analysis. A value of p < 0.05 was considered statistically significant.
Results
Age distribution of HBV serum markers
Figure 1 depicts 7 serum infection models. When considering the number of positive cases for HBV serum markers, the anti-HBs+anti-HBc infection model exhibits the highest count, followed by the HBsAg+HBeAg model. Among all infection models, the age group of 15–18 years demonstrates the highest incidence of reported infections (Fig. 1A). In addition, the positivity rate of HBsAg and/or HBeAg is also greatest within the 15–18 age group (Fig. 1B). Of interest, the anti-HBs+anti-HBc model exhibits the highest positivity rate in the 7-month to 3-year-old age group (Fig. 1C).
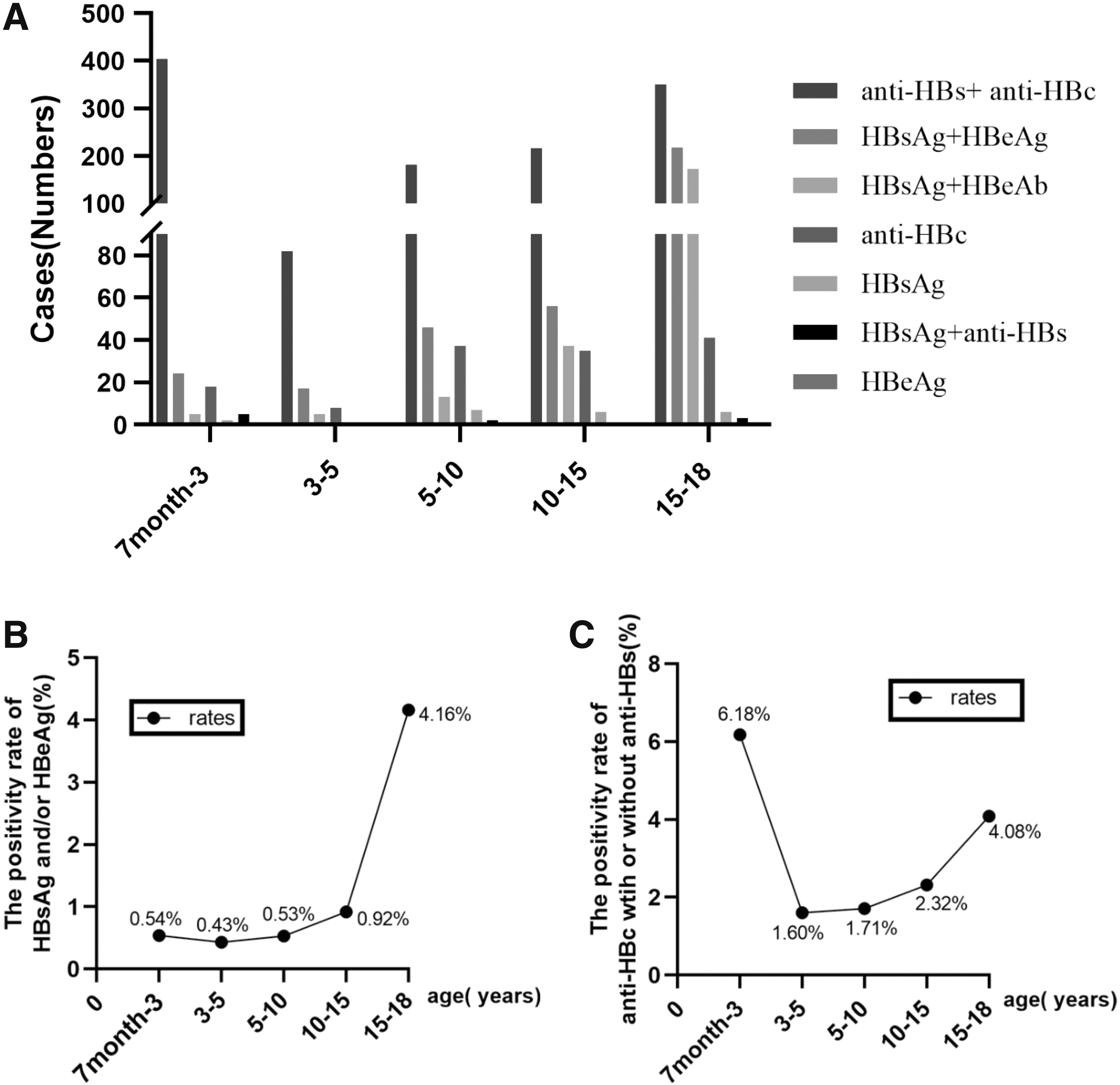
Age distribution of HBV serum markers. The combination pattern of HBV refers to the classification and description of different conditions of hepatitis B infection based on the detection results of related serum markers. The age ranges mentioned include the upper limit but exclude the lower limit.
Prevalence of anti-HBs titer by gender and age groups
There is a significant difference in anti-HBs titer between genders (p < 0.05). For the 0–10 IU/L group, females had a slightly higher ratio than males. The number of cases with anti-HBs titer >1000 IU/L is the lowest, regardless of gender. There is also a significant difference in anti-HBs titer across different age groups (p < 0.05). In the anti-HB–positive group (>10 IU/L), the 7 month < y ≤ 3 years age group has the highest or relatively higher number of cases than others. In the age group of 7 month < y ≤ 3, children exhibited a higher prevalence of anti-HBs levels concentrated in the 100–1000 IU/L and >1000 IU/L categories. Conversely, in the age group of 3 < y ≤ 5 years, there is a higher prevalence of anti-HBs levels concentrated in the 10–100 IU/L category. Overall, as age increases, there is a decreasing trend in the number of cases in different anti-HBs titer groups (Table 1).
Distribution of Anti-Hepatitis B Surface Titer in Age Groups and Gender Groups
The data in the table does not include patients who tested positive for HBsAg or anti-HBc.
HBs, hepatitis B surface; HBsAg, hepatitis B surface antigen.
Seroprotection rate and anti-HBs titer
With increasing age, the seroprotection rate gradually decreases and maintains a relatively low dynamic equilibrium after the age of 7. Of interest, females have a higher seroprotection rate than males before the age of 7. As age increases, anti-HBs titer gradually declines and maintains a relatively low concentration level after the age of 5. During the stages of 7 months to 5 years, females have slightly higher anti-HBs levels than males, whereas at the ages of 12, 13, and 15, males have slightly higher anti-HBs levels than females (p < 0.05) (Fig. 2).
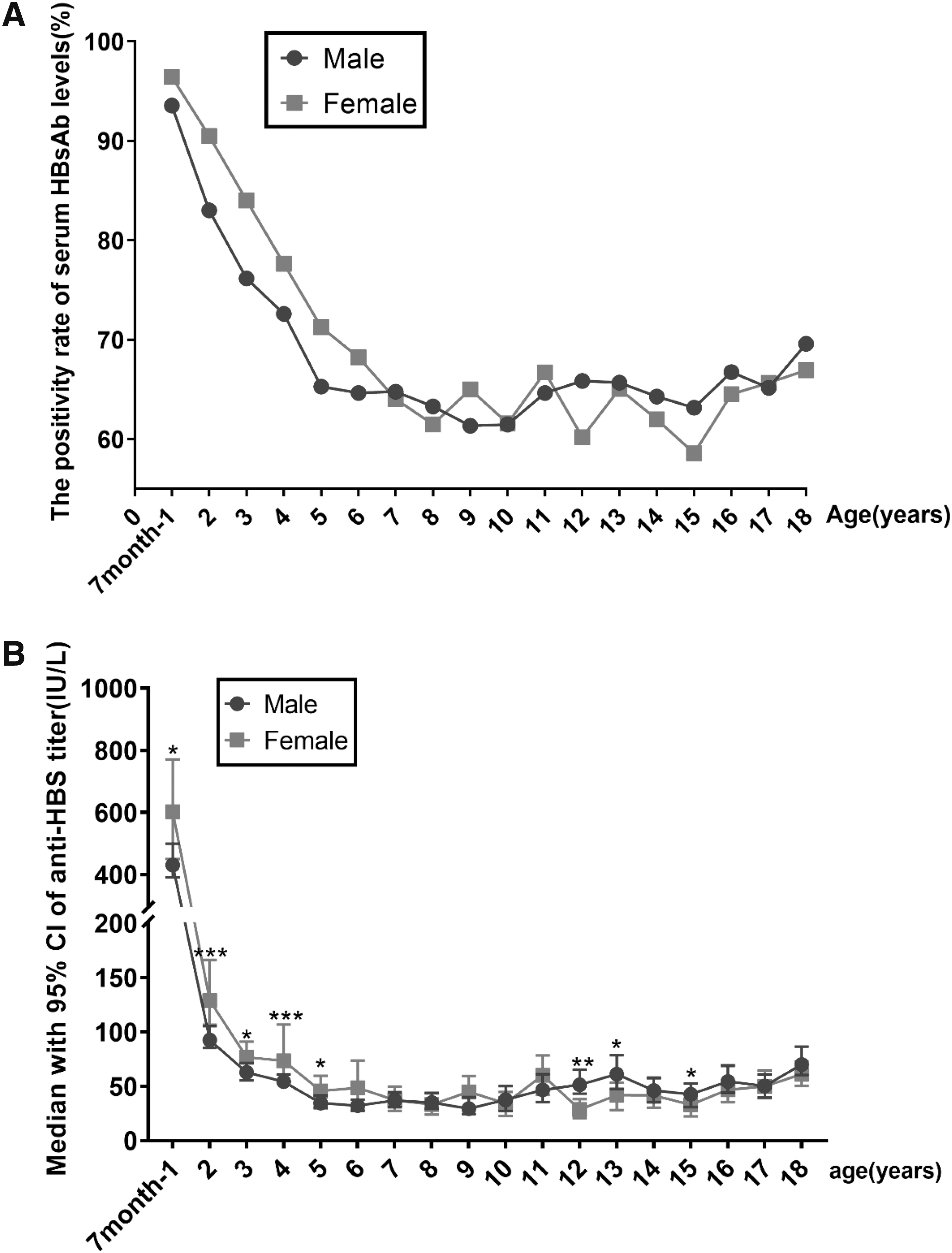
Year after vaccination.
Discussion
This study focuses on the relationship between anti-HBs levels and age/gender in individuals aged 7 months to 18 years who received hepatitis B vaccination in Wuhan, a city in central China, over the past 10 years. It is important to note that these individuals received their first dose of hepatitis B vaccine at birth.
Our study demonstrates that the seroconversion rate for anti-HBs antibodies after completing three doses of hepatitis B vaccination was ≥94%. According to literature, the proportion of individuals with protective anti-HBs levels after vaccination varies from 24% to 97%, depending on epigenetic factors (Mahmood et al., 2018; Zimmermann and Curtis, 2019). In our study, the 7 months to 3 years age group had a higher proportion in both the 100–1000 IU/L and >1000 IU/L titer groups compared with other age groups. In addition, the 3–5 years age group had a higher proportion in the 10–100 IU/L titer group compared with other age groups. We found that even in the age group with the lowest anti-HBs levels in our study, the rate of maintaining protective antibody levels was higher than what has been reported in previous studies (Dabrowska-Leonik et al., 2022). Individuals with autoimmune diseases, type 1 diabetes, and other related conditions have been found to exhibit a lower response to hepatitis B vaccination (Liu et al., 2017; Mormile, 2017; Saco et al., 2018). However, as our study did not investigate underlying medical conditions, we cannot provide any specific comments on this matter.
One-year postvaccination, a significantly higher seropositivity rate was observed among girls, with 96.43% showing protective antibody levels against hepatitis B compared with 93.55% in boys in 7 months to 1 year group. It is widely recognized that sexual dimorphism exists in both humans and animals regarding immune responses and viral infections. Females typically exhibit a lower susceptibility to viral infections compared with males, as they mount a more efficient, intense, and sustained immune response involving innate, humoral, and cell-mediated components (Giefing-Kröll et al., 2015; Ruggieri et al., 2016). The innate immune response, which serves as the first line of defense against viruses, is mediated by pattern recognition receptors such as Toll-like receptors (TLRs), retinoic acid–inducible gene I-like receptors, and nucleotide oligomerization domain-like receptors. These receptors recognize viral elements and trigger the production of type 1 interferon and inflammatory cytokines.
Once a viral infection is established, adaptive immune responses are activated by antigen-presenting cells and B cells, leading to the production of antibodies specific to viral antigens. In the majority of cases, females exhibit a stronger immune response, characterized by higher antibody titers and a greater frequency of seroconversion to HBeAg and HBsAg antibodies, after prophylactic HBV vaccination or in chronic carrier states (Klein et al., 2015; Su et al., 2007a). Regarding HBV vaccination, it has indicated that girls vaccinated after the age of 1 year tend to exhibit a 1.2-fold higher median antibody titer compared with boys in Italy (Trevisan et al., 2020). Similar trends have been reported for other childhood vaccines, with females displaying increased antibody titers and longer-lasting immune responses (Fischinger et al., 2019). These differences may be attributed to enhanced TLR-7 responses in females, including more pronounced inflammatory reactions to vaccine adjuvants.
Studies in mice have also demonstrated higher rates of seroconversion, elevated anti-HBs antibody titers, stronger T cell responses, and improved immunological memory in females following HBV vaccination (Kosinska et al., 2017; Li et al., 2019). However, the precise role of androgens and estrogens in regulating T cell responses to HBV infection remains unclear, although some evidence suggests their involvement (Yan et al., 2012). The extent to which these differences impact the efficacy of HBV vaccination in supporting elimination efforts remains uncertain; however, they highlight fundamental disparities in the quality and quantity of immune responses, which may contribute to a certain degree of elevated susceptibility in males, although quantifying this susceptibility is challenging. In addition to the above, we cannot solely attribute the higher overall positivity rate in our study compared with the literature to the influence of gender, as we had a larger number of male participants than female participants.
We observed a decline in both the seropositivity rate and levels of anti-HBs over time following the initial vaccination. However, despite this decline, we found that the prevalence of HBsAg and/or HBeAg carriage among individuals younger than 15 years old was >1%. This indicates that the hepatitis B vaccine still provides protection, even when antibody titers are <10 IU. Numerous studies have shown that a decline in antibody titer below the level of 10 IU/L does not necessarily indicate the disappearance of protective effect. After the initial HBV vaccination, circulating HBsAg-specific T cells were detected, indicating the generation of a specific immune response. Functional HBsAg-specific memory T cells and B cells were observed in some vaccinated individuals, even in the absence of subsequent antibodies (Bauer and Jilg, 2006; Brunskole Hummel et al., 2016; Lu et al., 2008).
One study has reported that more than half of the children who had their antibody levels turn negative after initial vaccination showed high-titer antibody responses after a single-dose booster vaccine administered 15 years later (Hammitt et al., 2007). Although the prevalence of hepatitis B infection has reached very low levels owing to the widespread use of the hepatitis B vaccine, the causes underlying postvaccine chronic infections are still worth pondering. Hepatitis B vaccination is recommended for susceptible adults at risk of HBV infection, including individuals who frequently require blood products, dialysis patients, incarcerated individuals, intravenous drug users, people with multiple sexual partners, men who have sex with men, health care workers, and close contacts of individuals with chronic HBV infection (Schillie et al., 2018).
However, the reasons behind ongoing infection rates in vaccinated populations can be attributed to two main factors: the variability of the HBV virus and inadequate immune responses after vaccination. HBV exhibits a unique life cycle with a high mutation rate, resulting in different genetic variants. Mutations in the S gene of HBV can lead to breakthrough infections in vaccinated individuals, as the antibodies induced by the vaccine may not recognize these mutated forms (Hudu et al., 2015; Qin and Liao, 2018). Universal HBV vaccination programs have been effective in preventing chronic liver disease and HCC in China, but cases of HBV vaccine breakthrough infection and occult hepatitis B infection have still been observed, potentially linked to S gene mutants.
Furthermore, although intramuscular administration of three vaccine doses should trigger a protective antibody response, some individuals may not develop sufficient immunity even after completing the recommended series (Kim et al., 2003; Schillie et al., 2013). Known as nonresponders, this group may be influenced by factors such as age, obesity, smoking, alcohol consumption, immunosuppression, genetics, and comorbid conditions like diabetes. In summary, the patterns of HBV infection in the vaccinated population remain unknown owing to the HBV virus's variability and inadequate immune responses following vaccination.
Unfortunately, we have also observed that compared with other groups, adolescents above the age of 15 have an increased anti-HBs positivity rate. The increased prevalence of hepatitis B infection can be attributed to individuals being infected during infancy but remaining undetected until adolescence when they undergo medical examinations or hospitalizations. This may be owing to the rarity of contact with individuals chronically infected with HBV in vaccinated young children, as reflected by a low percentage of HBsAg. However, beyond the age of 15, sexual activity and intravenous drug abuse increase the likelihood of infectious contacts and infections, especially in individuals with low levels of anti-HBs antibodies (Klinger et al., 2018). Upon examining the factors contributing to nonvaccination at enrollment, Meriki et al. observed that a majority of sexual partners and household contacts of chronically infected individuals had not received vaccination owing to a lack of awareness (Meriki et al., 2018). This lack of awareness manifested in two ways: some participants had never heard of hepatitis B infection, whereas others were unaware of the existence of a vaccine against HBV infection. Therefore, the Centers for Disease Control and Prevention (CDC) should determine the anti-HBs levels and administer a booster dose of hepatitis B vaccine at this age. Some researchers suggest administering a booster dose of hepatitis B vaccine to adolescents with low levels of protective hepatitis B antibodies during their teenage years, to increase their immunity to hepatitis B in adulthood (Aghakhani et al., 2011; Floreani et al., 2004). The purpose of vaccination was to ensure that adolescents and adults are protected against HBV infection when the risk increases.
It is worth mentioning that the prevalence of HBsAg and/or HBeAg among infants aged 7 months to 1 year is 0.54%. Although this rate is low, it does reflect a certain risk of infection among newborns and is largely responsible for the increasing infection rates with age. In China, mother-to-child transmission (MTCT) is considered the primary route of chronic HBV infection, accounting for 40–50% of new HBV infections (Xu et al., 2013). The National Health Commission implemented the integrated prevention of MTCT program, which mandates HBsAg screening for pregnant women and the provision of free extra HBIG (100 IU) within 24 h after birth for infants born to HBsAg-positive mothers. Administering HBIG and hepatitis B vaccination to infants born to HBsAg-positive mothers has proven highly effective in preventing MTCT of HBV.
However, infants born to pregnant women with a high HBV-DNA load still experience infection (Xu et al., 2013). Studies have shown a higher failure rate of HBIG plus vaccination among infants born to mothers with high HBV-DNA load compared with those born to mothers with a low HBV-DNA load (Lin et al., 2014; Zou et al., 2012). Nevertheless, recent studies have reported significantly lower failure rates when HBIG and vaccination are administered as early as possible after birth for infants whose mothers are HBsAg positive (Jourdain et al., 2018; Wei et al., 2018). Although the MTCT of HBV among HBsAg-positive pregnant women has declined, several factors contribute to the higher prevalence of HBsAg in pregnant women (Cui et al., 2018). Limited economic and health resources, inadequate public health education about HBV, and low awareness of infection risks result in less active screening and prevention efforts in these areas.
In addition, specific cultural practices in certain ethnic minority regions may contribute to the frequent occurrence of high-risk behaviors. Therefore, additional strategies must be implemented to decrease HBsAg prevalence among pregnant women, particularly in remote, rural, or ethnic minority areas. These strategies include strengthening the implementation of universal hepatitis B vaccination programs, intensifying public health education to discourage high-risk behaviors, and prioritizing HBV screening and prevention. Timely administration of HBIG and birth-dose hepatitis B vaccination, along with strict adherence to the immunization schedule for infants born to HBsAg-positive mothers, is crucial for preventing MTCT of HBV (Hou et al., 2019).
The limitations of our study include its retrospective design and the reliance on patient information obtained from the hospital's medical database. This article presents a retrospective study based on data from the past decade. One limitation of this study is the challenge in obtaining participants' vaccination history or information regarding their refusal of vaccination owing to the considerable time elapsed. Another limitation is that we did not assess whether participants had any underlying illnesses, given that certain diseases can have a negative impact on vaccine response.
Footnotes
Authors' Contributions
Z.N., the study design and data collection. P.Z., the data analysis and interpretation of results.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.