
Abstract
Global investment in developing COVID-19 vaccines has been substantial, but vaccine hesitancy has emerged due to misinformation. Concerns about adverse events, vaccine shortages, dosing confusion, mixing vaccines, and access issues contribute to hesitancy. Initially, the WHO recommended homologous vaccination (same vaccine for both doses), but evolving factors led to consideration of heterologous vaccination (different vaccines). The study compared reactogenicity and antibody response for both viral protein spike (S) and nucleocapsid (N) in 205 participants who received three vaccination regimens: same vaccine for all doses (Pfizer), two initial doses of the same vaccine (CoronaVac or AstraZeneca), and a Pfizer booster. ChAdOx1 and BNT162b2 vaccines were the most reactogenic vaccines, while CoronaVac vaccine was the least. ChAdOx1 and BNT162b2 achieved 100% of S-IgG seropositivity with one dose, while CoronaVac required two doses, emphasizing the importance of the second dose in achieving complete immunization across the population with different vaccine regimes. Pfizer recipients showed the highest S-IgG antibody titers, followed by AstraZeneca recipients, both after the first and second doses. A third vaccine dose was essential to boost the S-IgG antibodies and equalize the antibody levels among the different vaccine schedules. CoronaVac induced N-IgG antibodies, while in the Pfizer and AstraZeneca groups, they were induced by a natural infection, reinforcing the role of N protein as a biomarker of infection.
Introduction
According to the World Health Organization (WHO), as of April 2024, more than 775 million people have been infected with the SARS-CoV-2 virus, resulting in approximately 7 million deaths worldwide during the COVID-19 pandemic (World Health Organization, 2023). Confronted with the high mortality rate and the absence of a specific therapeutic approach, there has been intense investment and dedication worldwide towards the development of effective vaccines against COVID-19.
Various technologies were employed in the development of these vaccines, including nucleic acid, viral vector, and inactivated or protein subunit approaches (Chiu et al., 2021). mRNA vaccines, as Pfizer-BioNTech and Moderna, operate by introducing mRNA encoding the spike (S) viral protein of the SARS-CoV-2. This mRNA prompts cellular synthesis of the viral protein, which, recognized as foreign by the immune system, elicits an immune response. Viral vector vaccines, like AstraZeneca and Johnson & Johnson, utilize harmless viruses as vectors to deliver genetic material from SARS-CoV-2 into host cells, inducing production of the viral S protein and subsequent immune response activation. Analogous to mRNA vaccines, viral vector vaccines do not contain live virus. Inactivated or protein subunit vaccines, represented by CoronaVac and Covaxin, encompass either whole, inactivated viruses or specific viral proteins. These formulations facilitate immune recognition and subsequent immune response activation (Fernandes et al., 2023).
In the early stages of the pandemic, the World Health Organization (WHO) recommended homologous vaccination, which involves using the same vaccine for both doses of a vaccination series. However, SARS-CoV-2 variants of concern (VOCs) prompted a shift from homologous to heterologous vaccination. Heterologous vaccination refers to a vaccination strategy in which different vaccines or vaccine platforms are used for different doses within a vaccination series. The shift from homologous to heterologous vaccination strategy occurred due to several reasons. Firstly, some variants appeared to be more resistant to the protection offered by a single specific vaccine. Therefore, using different vaccines for the doses may enhance the immune response and protection against these variants. Additionally, some vaccines may have varying efficacy against certain variants. Thus, a heterologous approach was adopted to maximize vaccination effectiveness in response to the specific characteristics of the predominant variants in certain regions or at certain times (Borobia et al., 2021; Folegatti et al., 2020).
Brazil started the COVID-19 immunization in January 2021 with CoronaVac, initially prioritizing health care professionals, the elderly, and individuals with comorbidities. As vaccination progressed and more vaccine options became available, priorities for vaccination groups and vaccine choices were adjusted. Initially, CoronaVac was widely used in Brazil due to its availability and storage ease (Cerqueira-Silva et al., 2022). However, with the availability of mRNA vaccines like Pfizer and Moderna, and viral vector vaccines such as AstraZeneca, there was a shift towards these vaccines. The transition from CoronaVac to AstraZeneca and Pfizer vaccines in Brazil was driven by many factors, among them vaccine availability and emergence of VOCs (Santos et al., 2023).
Numerous COVID-19 vaccines have emerged, each exhibiting distinct safety profiles and levels of efficacy. Given the limited real-world data available for various COVID-19 vaccination protocols, the present study aims to compare the reactogenicity and antibody response in individuals who received three different vaccination regimens: a scheme employing the same vaccine for all three doses (BNT162b2/Pfizer-BioNTech), and two alternative regimens employing a combination of different vaccines, with the initial two doses using the same vaccine (CoronaVac/Sinovac or ChAdOx1 nCoV-19/AstraZeneca), followed by a booster dose using BNT162b2 (Pfizer-BioNTech).
Methods
Ethical aspects
The study received approval from the Ethics Committee of the Instituto de Saúde e Gestão Hospitalar (ISGH) with the identification number 5.417.716. The study’s participants were selected through random assignment.
Cohort and study design
The prospective study was conducted between January 2021 and July 2022, in Ceará, Brazil. We included a total of 205 participants of both sexes, aged ≥18 years, who had received a primary vaccination regime of two doses of CoronaVac (Sinovac), BNT162b2 (Pfizer-BioNTech), or ChAdOx1 nCoV-19 (AstraZeneca). The interval between the doses was in accordance with the manufacturer’s instructions for each vaccine. Subsequently, all participants received a third (or booster) dose of the BNT162b2 vaccine (Fig. 1). The CoronaVac group received the first vaccine dose in January 2021, followed by the second dose administered 4 weeks later, in February 2021. The BNT162b2 group received the first vaccine dose in May to June 2021, with the second dose typically administered 12 weeks later, between August and October 2021. Similarly, the ChAdOx1 group received their first vaccine dose between May and July 2021, with the second dose administered 8 weeks later, between May and July 2021 as well. The rollout of the third dose of the COVID-19 vaccine began in Brazil in September 2021 with the BNT162b2 vaccine. The CoronaVac group received their third dose in October 2021, while the BNT162b2 group received it between December 2021 and January 2022, and the ChAdOx1 group between December 2021 and February 2022.

Flowchart illustrating the immunization schedules for the different COVID-19 vaccines, CoronaVac (Sinovac), BNT162b2 (Pfizer-BioNtech) and ChAdOx1 nCOVID-19 (Astrazeneca), and the blood sample collections. Antibody responses were evaluated 28 days after the first dose ± 15 dias (1D), 28 after the second dose ± 15 dias (2D), two months ± 30 dias (2mA3D), and six months ± 30 dias (6mA3D) after the third dose.
Clinical data were gathered through the administration of a questionnaire, while blood samples were meticulously collected and subjected to serological tests at Fundação Oswaldo Cruz (Fiocruz) in Ceará, Brazil, with full adherence to participants’ informed consent. The reactogenicity was evaluated within the first week after each vaccine dose. The variables used in this study included demographic data, such as sex, age, and self-reported COVID-19 symptoms. For ethnicity, we employed a self-reported standard Brazilian skin color/ethnicity classification encompassing five categories: White, Black, Brown, Asian, and Indigenous.
Laboratory analysis
We collected samples at specific time points: 28 days (±15 days) after the first dose (1D), 30 days (±15 days) after the second dose (2D), two months (2mA3D, ±30 days), and six months (6mA3D, ±30 days) after the third dose (Fig. 1). The intervals between vaccination and blood collection were the same in all three groups. For the CoronaVac group these periods corresponded to February 2021, March to May 2021, November 2021 to January 2022, and March to April 2022. For the BNT162b2 group, the periods were June to July 2021, September to October 2021, January to March 2022, and May to July 2022. For the ChAdOx1 group, the periods were June to July 2021, August to October 2021, January to March 2022, and May to July 2022. Antibody presence was evaluated using the chemiluminescence method on the Abbott Architect i2000SR platform (Abbott®). The chemiluminescent immunoassay measures antibodies against the nucleocapsid protein (N) and the receptor-binding domain (RBD) of the S1-subunit of the Spike (S) protein from the original strain of SARS-CoV-2. The established thresholds were 50 AU/mL for S IgG and 1.4 index value for N IgG.
Statistical analysis
Statistical analyses were performed using GraphPad Prism version 8.0.1 (https://www.graphpad.com). Continuous variables were described using the median and interquartile range. Percentages and proportions were used to depict count data. To examine the antibody levels over time, analysis of variance was employed. For group comparisons, Student’s t-test, or the Mann–Whitney test was utilized. Statistical significance was determined for differences with p < 0.05.
Results
The cohort consisted of 205 volunteers who participated in at least one data collection during the study. Among them, 58 volunteers received two doses of the ChAdOx1 nCoV-19 vaccine, 46 received the BNT162b2 vaccine, and 101 received the CoronaVac vaccine. The third (or booster dose) administered to the cohort was the BNT162b vaccine. Females were the predominant gender within the cohort, with 153 (74.6%) individuals, while males accounted for 52 (25.4%) individuals. For ethnicity, 52.2% (107) of the participants self-declared as Brown, 39% (80) as White, 5.4% (11) as Black, and 3.4 (7) as Asian. The average age of the cohort was 36.60 (95% confidence interval [CI]: 19–74 years). The average ages were similar for the three groups, ChAdOx1 with 39.22 (95% CI: 20–67 years), BNT162b2 with 34.26 (95% CI: 19–58 years), and CoronaVac with 36.16 (95% CI: 20–74 years).
The incidence of adverse events (AEs) was lower in the group that received CoronaVac, with rates of 19.4% and 25.8% after the first and second doses, respectively. In contrast, the BNT162b2 group exhibited rates of 63% and 56.1% for the first and second doses, while the ChAdOx1 group showed rates of 70.7% and 53.4% for the first and second doses, respectively (Fig. 2).
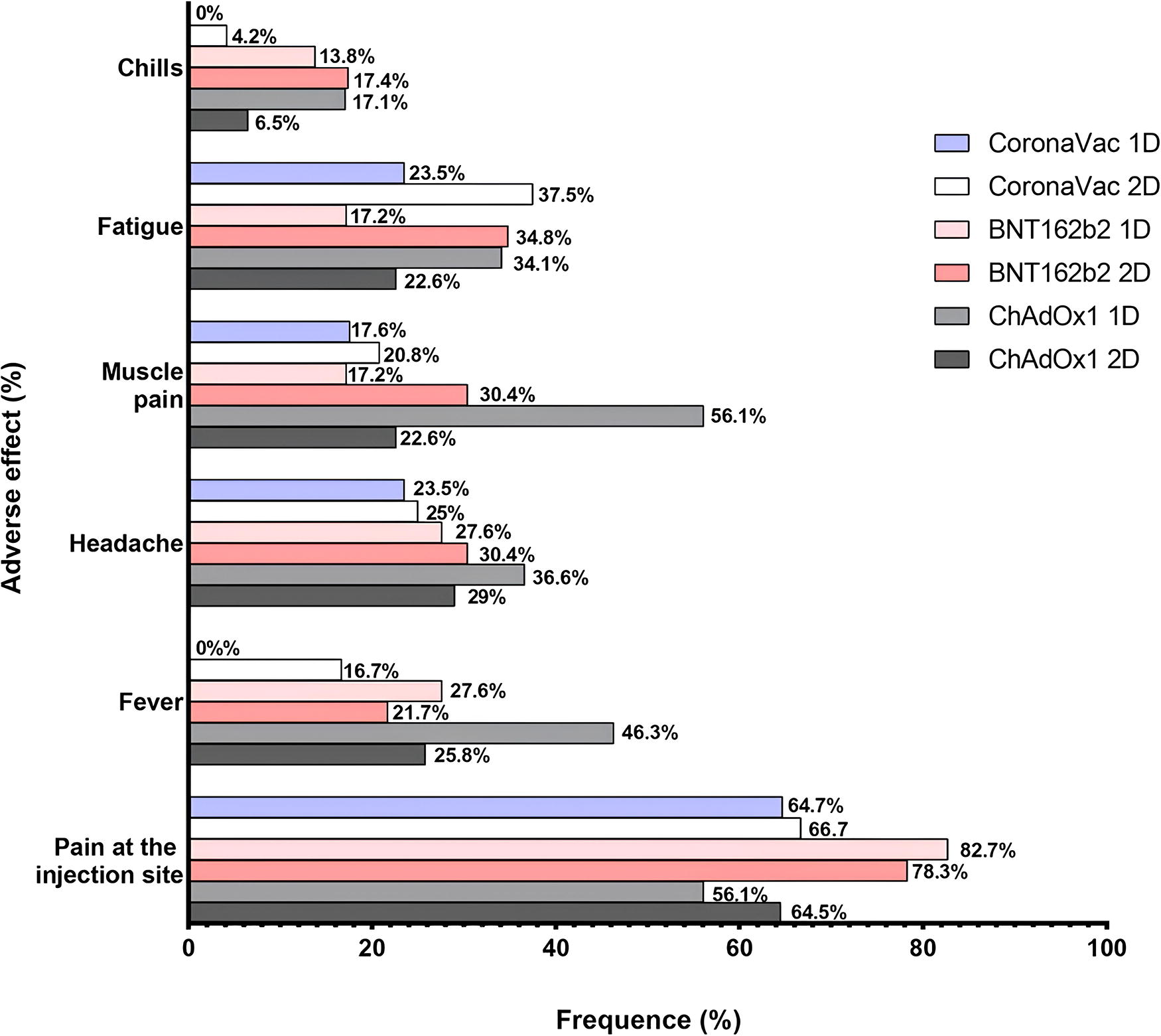
Comparison of adverse events frequencies among CoronaVac (Sinovac), BNT162b2 (Pfizer-BioNtech), and ChAdOx1 nCOV-19 (AstraZeneca) vaccines following the first (1D) and the second doses (2D).
Regardless of the vaccination schedule, pain at the injection site was the most frequently reported AEs among participants. After the first dose, 64.7% (11/17) of CoronaVac recipients reported pain at the injection site, compared with 82.7% (24/29) in the BNT162b2 group and 56.1% (23/41) in the ChAdOx1 group. After the second dose, the frequency of pain at the injection site was 66% (16/24) for CoronaVac, 78.3% (18/23) for BNT162b2, and 78.3% (18/23) for ChAdOx1. After the third dose, 80/145 (55%) of participants experienced AE. The main reported AE were pain at the application site (79%), followed by pain in the body (39%), fatigue (26%), fever (25%), headache (19%), and chills (7.5%).
We evaluated the seropositivity and antibody levels of IgG for S (S-IgG) and for N (N-IgG) proteins, after the first (1D) and second (2D) doses of ChAdOx1, BNT162b2, or CoronaVac, as well as two months (2mA3D), and six months (6mA3D) after the third dose with BNT162b2. Regarding S-IgG antibodies (Fig. 3A, Table 1), the seropositivity was 100% for individuals who received either ChAdOx1 or BNT162b2 vaccines in 1D. However, those who received CoronaVac exhibited a seropositivity of 82.1%. In terms of antibody levels, participants who received BNT162b2 showed significantly higher antibody levels (median [IQR] = 13,742 [1,420–18,708]), compared with CoronaVac (median [IQR] = 164.8 [61.5–439.3], p < 0.0001) and ChAdOx1 (median [IQR] = 2,474 [208.9–6,763], p = 0.0043). Additionally, the ChAdOx1 group exhibited higher S-IgG levels compared with the CoronaVac group (p < 0.0001). During the 2D period, all groups achieved 100% of seropositivity for S IgG. In terms of S-IgG levels, individuals who received BNT162b2 maintained the highest antibody levels (median [IQR] = 11363 [7,258–14,099]), while those who received the CoronaVac had the lowest levels (median [IQR] = 1011 [477.8–1,779]). Following the booster dose (2mA3D), S-IgG seropositivity remained at 100%, and an antibody boost was observed, particularly in the CoronaVac and ChadOx1 groups (p < 0.0001). The levels were standardized, and there was no statistical difference among the groups. However, at 6mA3D, while S-IgG seropositivity was sustained, a statistical disparity in S-IgG levels emerged between the BNT162b2 and the ChAdOx1 groups (median [IQR] = 15,213 [7,291–28,432] versus 6,096 [3,745–14,271], p = 0.0243).
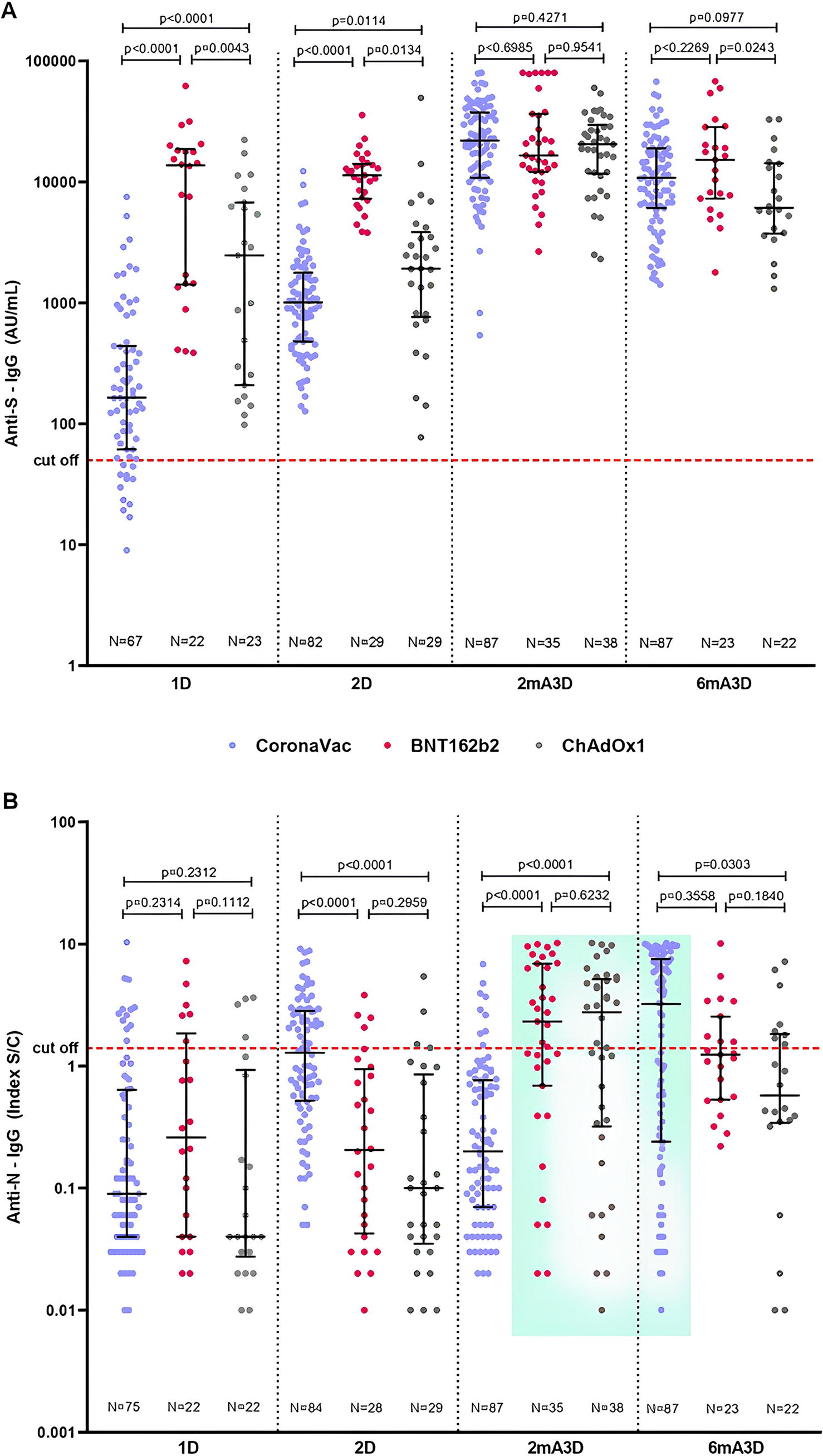
Antibody levels in recipients of two doses of CoronaVac (Sinovac), BNT162b2 (Pfizer-BioNTech), or ChAdOx1 nCoV-19 (AstraZeneca), and a booster dose of BNT162b2 (Pfizer-BioNTech).
The Median (and IQR) Values of the Antibody Levels after COVID-19 Vaccine Doses, in Recipients of Two Doses of CoronaVac (Sinovac), BNT162b2 (Pfizer-BioNTech), or ChAdOx1 nCoV-19 (AstraZeneca), and a Booster Dose of BNT162b2 (Pfizer-BioNTech)
Antibody responses were evaluated 28 days after the first dose (1D), 28 after the second dose (2D), two months (2mA3D), and six months (6mA3D) after the third dose. N, nucleocapsid protein; S, spike protein. CoronaVac (Sinovac), BNT162b2 (Pfizer-BioNtech), and ChAdOx1 nCOVID-19 (Astrazeneca).
Regarding N-IgG antibodies (Fig. 3B, Table 1), the seropositivity was 22.7%, 18%, and 13% in the BNT162b2, CoronaVac, and ChAdOx1 groups, respectively, at 1D. For N-IgG levels, no significant difference was observed between groups in this timepoint. At 2D, the CoronaVac group exhibited a seropositivity of 47.6%, while the BNT162b2 and ChAdOx1 groups showed a seropositivity of 13.8%. the CoronaVac group also showed higher antibody levels, (median [IQR] = 1.28 [0.52–2.83]) compared with BNT162b2 (median [IQR] = 0.205 [0.04–0.94], p < 0.0001) and ChAdOx1 (median [IQR] = 0.1 [0.04–0.86], p < 0.0001) groups. Interestingly, at 2mA3D, the seropositivity declined to 10.5% in the CoronaVac group, but increased to 55.3%, and 57.9% in the BNT162b2 and ChAdOx1 group, respectively. Similarly, the groups that received BNT162b2 and ChAdOx1 showed higher IgG-N levels (median [IQR] = 2.32 [0.69–6.91], and 2.76 [0.32–5.17], respectively) compared with the CoronaVac group (median [IQR] = 0.20 [0.07-0.86], p < 0.0001). By 6mA3D, the N-IG seropositivity was 55.2% in the CoronaVac group, 39.1% in the BNT162b2 group, and 36.4% in the ChAdOx1 group. N-IgG levels were higher in the CoronaVac group (median [IQR] = 3.23 [0.24–7.53]) compared to ChAdOx1 group (median [IQR] = 0.58 [0.34–1.83] p = 0.0303), but no statistically significant differences were found when compared to the BNT162b2 group (p = 0.3558).
After evaluating of the completed questionnaires submitted by the participants, the incidence of COVID-19 infections was documented across different phases. In the initial dose phase (1D), infection rates stood at 18% within the CoronaVac group, 22.7% within the BNT162b2 group, and 13% within the ChAdOx1 group. Moving to the second dose phase (2D), infection rates experienced a decline to 10% for the CoronaVac group, 7% for the BNT162b2 group, and 17.2% for the ChAdOx1 group. Subsequently, during the phase observed two months after the administration of the third dose (2mA3D), infection percentages were recorded at 8.0% for the CoronaVac group, 34.3% for the BNT162b2 group, and 44.7% for the ChAdOx1 group. Impressively, after six-month of the third dose (6mA3D), COVID-19 infections were exclusively reported by the CoronaVac group, constituting a rate of 48.3%.
Discussion
The aim of vaccination is to generate immunity against a disease while also reducing the severity of symptoms, accompanied by a low occurrence of AEs. The meticulous selection of a vaccine characterized by a diminished incidence of AEs assumes critical importance in ensuring extensive vaccine coverage across the population. Furthermore, vaccines associated with low rates of AE may be prioritized within specific cohorts, pregnant women, young children, the immunocompromised and the elderly. Hence, comparative analyses of the immunogenicity and reactogenicity of diverse SARS-CoV-2 vaccine-regimens hold the potential to refine vaccine strategies. In light of this, the present study assessed the immunogenicity and reactogenicity of the principal vaccines employed in Brazil: CoronaVac (Sinovac), a whole inactivated virus vaccine; BNT162b2 (Pfizer-BioNTech), an mRNA vaccine; and ChAdOx1 nCoV-19 (AstraZeneca), a viral-vectored vaccine (Flaxman et al., 2021; Palacios et al., 2021; Vogel et al., 2021).
The three different vaccine types (platforms) displayed distinct reactogenicity profiles, which also varied between the first and second dose of each specific vaccine. ChAdOx1 vaccine recipients exhibited the highest incidence of AEs compared with the other vaccines after the first dose. Compared AEs between homologous and heterologous vaccination regimens, finding higher incidences among homologous ChAdOx1 recipients (Eybpoosh et al., 2023). However, our findings showed that, after the second dose, this trend reversed, with the BNT162b2 vaccine recipients showing a higher rate of AEs in comparison to the ChAdOx1 vaccine. In contrast, the CoronaVac vaccine recipients demonstrated a lower occurrence of adverse events both after the first and second doses. These findings are in accordance with a systematic review conducted by Sutton and colleagues (Sutton et al., 2022), where they highlighted that inherent biological differences among these vaccines (such as mRNA vs inactivated virus) as well as the inclusion of different adjuvants or vaccine dosage influence on the occurrence of AE. According to them, mRNA vaccines are the most reactogenic, while inactivated vaccines are the least reactogenic. However, the occurrence of AEs can vary depending on the dose. mRNA vaccines tend to manifest higher rates of events following the second dose, viral-vectored vaccines show elevated rates after the first dose (compared with the second dose), and inactivated virus vaccines show comparable rates of AEs after both the first and second doses. The main AEs reported in the study were injection site pain (79%), followed by body pain (39%), fatigue (26%), fever (25%), headache (19%), and chills (7.5%), regardless of the vaccination schedule. Similarly, in a study by Alghamdi and colleagues (Alghamdi et al., 2021), recipients of the AstraZeneca vaccine mentioned muscle aches (49%), fever (42%), and headache (40%) as the most frequent AEs. Likewise, Eybpoosh et al. (Eybpoosh et al., 2023) reported a high incidence of fatigue, myalgia, and chills in individuals vaccinated with homologous ChAdOX. Moreover, Mahase (Mahase, 2020) described injection site pain as the primary AE reported following the Pfizer vaccine. Additionally, Ramezani and colleagues (Ramezani et al., 2023) compared AEs in individuals vaccinated with inactivated-virus based vaccine (BBIP-CorV) and protein-subunit based vaccines (PastoCovac/Plus). They reported pain at the injection site in 15.9%, 11.3%, and 4.5% of the PastoCovac Plus, BBIBP-CorV and PastoCovac groups, respectively. Furthermore, systemic AEs were observed in 19.4% of BBIBP-CorV, 14.3% of PastoCovac, and 4.5% of PastoCovac Plus recipient`s, among which headache and weakness were the most common. In immunogenicity analyses, CoronaVac group exhibited the lowest S-IgG seropositivity after the first dose, as well as lower levels of anti-S IgG after both the first and second doses. A total of 82.1% individuals who received the CoronaVac vaccine developed IgG antibodies after receiving only one dose. In contrast, all individuals who received the ChAdOx1 or BNT162b2 vaccines became seropositive with a single dose. Following the administration of second vaccine dose, all individuals achieved 100% of seropositivity. These findings reflect the importance of the second dose of CoronaVac in achieving complete immunization across the population. In terms of antibody levels, recipients of BNT162b2 showed the highest antibody levels, followed by ChAdOx recipients, both after the first and second doses. In fact, mRNA vaccines have emerged as promising alternatives to provide protection against SARS-CoV-2 due to their potency of induction of high levels of S-IgG and neutralizing antibodies, as well as and their low-cost production (Salleh et al., 2022; Sauré et al., 2022). It is important highlighted that mRNA and vector recombinant vaccines can also generate cellular immunity, in addition to humoral immunity. Cytotoxic T cells (CD8+) and helper T cells (CD4+) are important components of the cellular immune response and play a crucial role in eliminating virus-infected cells (Ura et al., 2022).
A boost in S-IgG was observed after the third vaccine dose with BNT162b2, particularly within the CoronaVac and ChadOx1 groups. The third vaccine dose led to an equalization of S-IgG levels among the groups. The notable increase in the S-IgG levels within the CoronaVac and ChadOx1 groups post the third dose reinforced the significance of this additional vaccine dose (Fonseca et al., 2022; Kontopoulou et al., 2022; Silva-Valencia et al., 2022). Furthermore, an antibody decay was observed at 6mA2D within the CoronaVac and ChadOx1 groups, with a more pronounced effect in the latter group. No diminishment of antibody levels was noted within BNT162b2 group. The decline in antibody levels following COVID-19 vaccination is already well-established, however, whether this decline signifies an increased risk of re-infection is still a matter of debate (Ali et al., 2021; Cheetham et al., 2023; Wei et al., 2022). Although the group vaccinated with BNT162b2 did not show waning antibodies, it is important to emphasize that the efficacy of mRNA vaccines may be compromised by the newly emerging variants of SARS-CoV-2 (Salleh et al., 2022), since they provided immunity exclusively against the S protein.
For N-IgG levels, no significant difference was observed among the groups at 1D. However, in 2D, the CoronaVac group showed higher antibody levels compared to BNT162b2 and ChAdOx1 groups. This result was expected, given that CoronaVac vaccine elicits immunity against all proteins of the SARS-CoV-2, including the N protein. In opposition, BNT162b2 and ChAdOx1 vaccines induce a limited response to the S protein. Interestingly, after the booster dose (2mA3D), the groups that received BNT162b2 and ChAdOx1 showed higher levels of N-IgG compared with the CoronaVac group. As these groups were not immunized against the viral N protein, the increase in N-IgG levels could be explained by a natural infection. Indeed, 34.3% of BNT162b2 group and 44.7% of the ChAdOx1 group reported a SARS-CoV-2 infection at 2mA3D, in contrast to 8% in the CoronaVac group. The same explanation can be applied to the highest N-IgG levels in the CoronaVac group at 6mA3D, considering that 48.3% of them reported an infection, while no infections were reported in the other groups at this time point. The increase in natural SARS-CoV-2 infections during this period is associated with the Omicron wave in Brazil. The peak of the Omicron outbreak in Brazil was between November 2021 and March 2022 (Duong et al., 2022; Valverde., 2022), which aligns with the evaluated timeframes. Since the Omicron variant has mutations in S protein that confer immune escape, an initial infection can occur in vaccinated people (Willett et al., 2022). We can observe that, unlike the S protein, the N protein fluctuates according to natural infections. Indeed, the viral N protein plays an important role in the coronavirus life cycle, and have been described as an important diagnostic marker for COVID-19 (Wu et al., 2023).
This study has limitations since the different COVID-19 vaccines arrived at different times in Brazil, and therefore, the groups could not be evaluated at the same time. However, it is important highlighted that the intervals between vaccination and blood collection were the same in all three groups.
In conclusion, ChAdOx1 and BNT162b2 vaccines were the most reactogenic vaccines, while CoronaVac vaccine was the least. All individuals who received the ChAdOx1 or BNT162b2 vaccines became S-IgG seropositive with a single vaccine dose. The same seropositivity was achieved just with two CoronaVac doses. These finding reflect the importance of the second dose in achieving complete immunization across the population with different vaccine regimes. In terms of antibody levels, recipients of BNT162b2 showed the highest S-IgG antibody levels, followed by ChAdOx recipients, both after the first and second doses. A third vaccine dose was essential to boost the S-IgG antibodies and equalize the antibody levels among the different vaccine schedules. The N-IgG antibodies were induced by the vaccine in the CoronaVac group, while in the BNT162b2 and ChAdOX groups, they were induced by a natural infection, reinforcing the role of N protein as a biomarker of infection. The boosted in N antibodies in the CoronaVac group six months after the third dose and during the omicron wave in Brazil, suggest an immunological memory.
Footnotes
Acknowledgments
The authors thank the health care workers of state of Ceará, Brazil, for participating in this study.
Authors’ Contributions
A.C.M.D.P., M.F.S.S., F.C.E.O., and M.H.G.F. conceived the work, contributed to the design of the study and the writing of the article. A.C.M.D.P., M.F.S.S., F.C.E.O., M.M.L.G., V.B.M., G.A.D., and T.C.M. were responsible for the recruitment, follow up, data collection, laboratory analysis and data processing work. M.H.G.F. contributed to sample collection and review and supervised the project. A.C.M.D.P. made the graphs and figures. All authors involved in writing, review and editing, approved the final article version.
Ethics Statement
The study was approved by the Ethics Committee of the Hospital Geral Dr. César Cals, through CAAE 39691420.7.0000.5049. Informed consent was obtained from all the individual participants.
Data Availability
Data will be made available on request. The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
The project is funded by Fiocruz and Ministério da Saúde, Brazil.