
Abstract
The enduring impact of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and its disease manifestation, COVID-19, on public health remains significant. Postacute sequelae of SARS-CoV-2 infection (PASC) affect a considerable number of patients, impairing their quality of life. While the role of the cytokine storm in acute COVID-19 is well established, its contribution to the pathophysiology of PASC is not fully understood. This study aimed to analyze the cytokine profile of patients with PASC following in vitro stimulation of Toll-like receptor (TLR) pathways, comparing them with a healthy control group. From October 2020 till March 2021, Brugmann University Hospital’s clinical research unit included patients with PASC in the study. Whole blood samples were collected from 50 patients and 25 healthy volunteers. After in vitro stimulation under five different conditions, cytokine levels were measured using a multiplex method. Significantly decreased cytokine levels were observed in patients with PASC compared with healthy volunteers, particularly after TLR4 (interleukin [IL]-1α, IL-1β, IL-2, IL-10, interferon (IFN)α, IFNγ, IFNω, and tumor necrosis factor (TNF)α) and TLR7/8 (IL-1α, IL-1β, IFNα, IFNω, IFNγ, and TNFα) pathway stimulation. Principal component analysis identified two distinct clusters, suggesting a likely dysregulation of immunity involving TLR4 and TLR7/8 pathways in patients with PASC. Our study suggests that TLR4 and TLR7/8 pathways play a role in the pathophysiology of PASC. Continuous basal activation of immunity could explain the high basal concentrations of cytokines described in these patients and the decreased amplitude of response of these signaling pathways following specific stimulation.
Introduction
In December 2022, the World Health Organization defined the postacute sequelae of SARS-CoV-2 infection (PASC) as “the continuation or development of new symptoms 3 months after the initial severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, with these symptoms lasting for at least 2 months with no other explanation” (World Health Organization, n.d.).
Although the pathophysiology of acute disease linked to SARS-CoV-2 (COVID-19) is not entirely clear to that day, it seems that the main mechanisms involved in the symptomatology of acute COVID-19 include direct toxicity of the virus, endothelial and microvessel damage, dysregulation of the immune system and the presence of exaggerated inflammation, a state of hypercoagulability leading to multiple thromboses, and, ultimately, a lack of adaptation of the angiotensin converting enzyme 2 pathway (Nalbandian et al., 2021). The mechanism responsible for the appearance of PASC has not yet been established despite numerous studies. Several physiopathological mechanisms have been suggested: the persistence of a toxic effect on the affected organ despite the clearance of the virus or, on the contrary, the persistence of the virus in situ, the predisposing effect of underlying mood disorders on the appearance of neurocognitive disorders, dysregulation of the immune system, the impact of SARS-COV-2 on the microbiota, autoimmunity, endothelial dysfunction, and dysfunction signaling in the central nervous system (Bellan et al., 2022; Davis et al., 2023; Machkovech et al., 2024; Munipalli et al., 2022). The hyperinflammatory state or “cytokine storm” thus seems to be strongly involved in the physiological mechanisms of acute COVID-19 as well as at a lesser degree in PASC (Verma et al., 2023). It has been suggested that the internalization of the angiotensin-converting enzyme 2 receptor upon viral entry leads to a shift in the renin angiotensin system and has a proinflammatory effect. Moreover, several authors proposed that Toll-like receptors (TLRs) and the signaling cascades they regulate seem involved in the pathophysiology of acute COVID-19 and may play a role in the severity of the disease (Brauns et al., 2022; Lee et al., 2023; Nazerian et al., 2022). Also, it has been demonstrated that the spike protein of the virus interacts with TLR4 and activates the secretion of proinflammatory cytokines (Gracie et al., 2024). Hence, TLRs emerge as an interesting lead for understanding the PASC disease.
Objective
The link between cytokine storm and acute COVID-19 has been formally established, but its role in PASC remains uncertain. It therefore seems interesting to look for cytokine dysregulation in patients with persistent post-COVID-19 symptoms. The objective of this work was to compare the cytokine profile differences, after in vitro stimulation of TLRs under five different conditions, between a control group of healthy volunteers and a group of patients presenting symptoms of PASC.
Materials and Methods
Starting in October 2020, patients presenting to the consultation at the Department of Clinical Research at Brugmann University Hospital, complaining about the long-term effects of their SARS-CoV2 infection, were included in our study focusing on the long-term impacts of COVID-19 on the central nervous system, referred to as the “long COVID” study. An extensive neurological and psychiatric examination was carried out in order to characterize the patients’ complaints. Data on medical history, comorbidities, and ongoing treatments were also collected. A whole blood sample on a sodium heparin tube and a serum tube were collected during the first consultation. Patients’ follow-up was planned for a period of 1 year. The follow-up and frequency of consultations were adapted according to the persistence of symptoms. In total, samples from 55 patients were collected.
This project received approval from the Brugmann University Hospital Ethics Committee, and informed consent forms were collected from all individuals participating in the study.
Patients’ selection
As a more refined definition of PASC was published after the beginning of our study (World Health Organization, n.d.), a more precise selection of patients was carried out for data analysis. The patients selected had to meet the following criteria: Beginning of symptoms within 12 weeks after suspected or proven SARS-CoV2 infection. Persistence of symptoms for at least 2 months. Exclusion of any other condition that could explain the patient’s symptoms.
In total, five patients were excluded because they did not meet the revised selection criteria. Fifty samples were analyzed (Fig. 1).
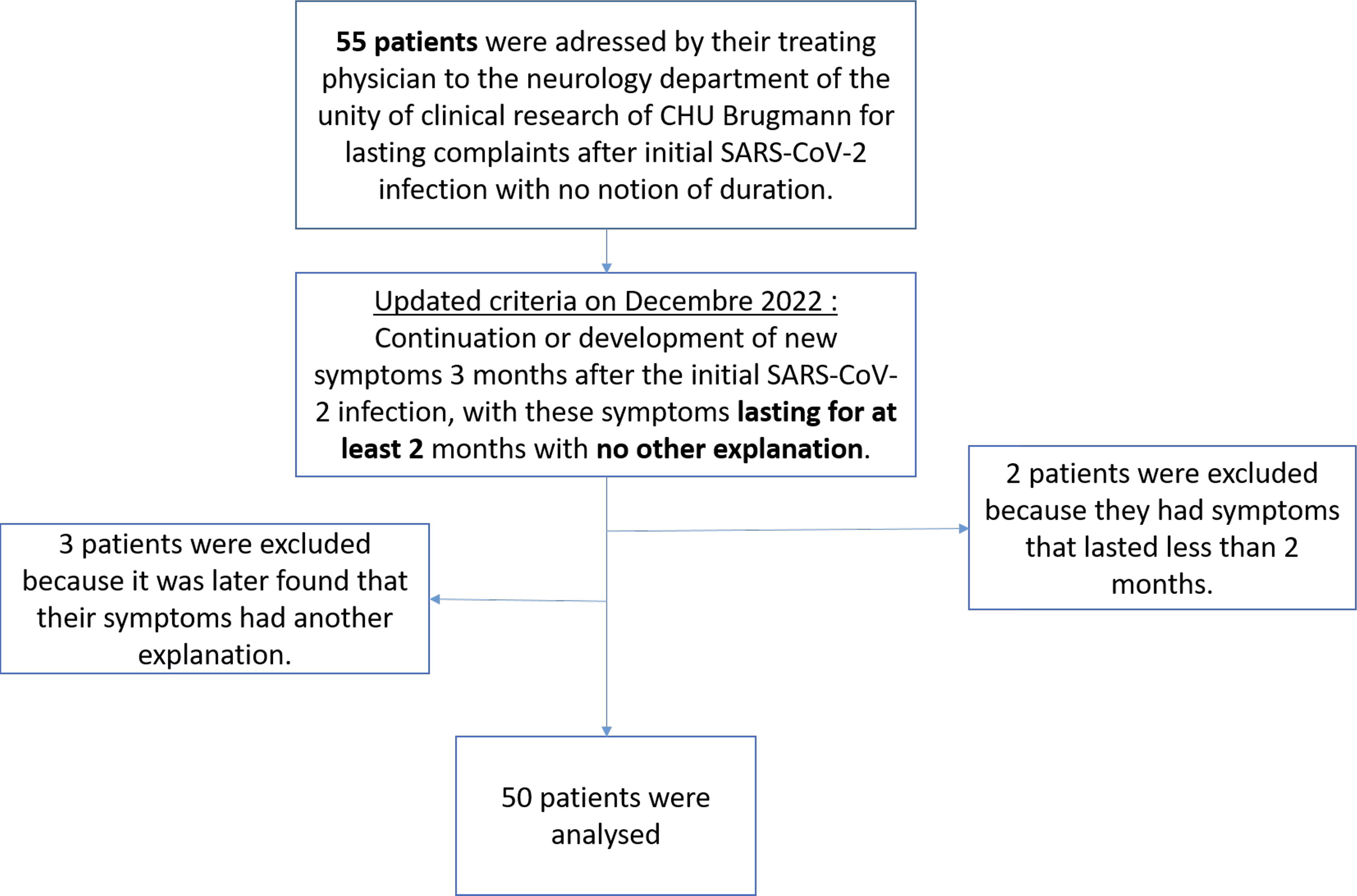
Flowchart representing the selection of patients.
Data collected
The data collected were age, sex, suspected date of infection, time between infection and sampling, duration of symptoms, and clinical symptomatology (predominant complaint and other complaints).
Healthy volunteers’ recruitment
Twenty-five healthy volunteers were recruited among health care workers. Upon recruitment, the volunteers were asked questions about their general health, the presence of a history of acute COVID-19, and the presence of long-term symptoms. Sixteen healthy volunteers had a history of acute nonsevere COVID-19 without persistent symptoms, and nine had no history of acute COVID-19.
In vitro stimulation
A volume of heparinized whole blood was diluted 1:5 in a mixture of phenol-red free Roswell Park Memorial Institute (RPMI 1640) (Invitrogen Life Technologies®), penicillin at a final concentration of 50 IU/mL, streptomycin at a final concentration of 50 IU/mL, and fetal bovine serum (Invitrogen Life Technologies) in order to obtain a cell suspension of approximately 1.106 leukocytes/mL.
In a 24-well plate, 1 mL of the previously prepared mixture was introduced into each well. Five wells were used per patient, each well corresponding to a given stimulation condition. Basal condition in the presence of the RPMI and antibiotic mixture only. Stimulation of the TLR4 pathway in the presence of Escherichia coli 026:B6 lipopolysaccharides (LPS) (Sigma-Aldrich®), at high concentration (10−6 g/mL) (Lefèvre et al., 2012). Stimulation of the TLR4 pathway in the presence of LPS at low concentration (10−9 g/mL) (Lefèvre et al., 2012). Stimulation of the TLR7/8 pathway in the presence of resiquimod (R848) (InvivoGen®) at a concentration of 10−6 g/mL (Lefèvre et al., 2012). Stimulation of the TLR3 pathway in the presence of polyinosinic–polycytidylic acid (Poly I:C) at a concentration of 10−5 g/mL (Alexopoulou et al., 2001; Duffy et al., 2014).
The plates were then incubated overnight at 37°C at 5% CO2 and 95% humidity in an incubator (Heraeus HBB 2472 b, Heraeus® Instrument GmbH). After 24 h of incubation, the supernatant was collected and stored at −80°C. Then, the cytokine assay was carried out.
Cytokine assay
The custom Q-Plex™ Human Cytokine Inflammation Panel 1 (9-Plex) and Q-Plex™ Human Innate Immunity (custom 7-Plex) kits (Quansys® Biosciences) were used. These kits allow the determination of IFNα, IFNβ, IFNγ, IFNω, TNFα, IL-1α, IL-1β, IL-2, IL-4, IL-6, IL-8, and IL-10.
The plates were read on the Q-View™ Imager LS device (Quansys), and the results were analyzed using the Q-View™ software (Quansys).
Statistical analysis
Descriptive statistics were performed on GraphPad Prism® software (version 5.0, GraphPad Software). Nonparametric statistical analyses and principal component (PC) analyses were performed using SPSS® software (Version 22.0, IBM Corp).
A Mann–Whitney test was performed within the healthy volunteers group in order to compare the one with a history of acute COVID-19 with the one with no history of acute COVID-19.
The assay results between the group of healthy volunteers and the group of patients were compared using a Mann–Whitney test. Following the results of the Mann–Whitney test, the cytokines for which the levels were significantly different between the group of healthy volunteers and the group of patients were selected. Two PC analyses were carried out: the first taking into account the cytokine levels after stimulation of the TLR7/8 pathway and the second taking into account the cytokine levels after stimulation of the TLR4 pathway. The PCs differ from each other by the weight assigned to each parameter included in the analysis. Thus, the variables are summarized into several PCs for each patient. Then, from these PCs, a point distribution graph is generated. When there were more than two PCs, the two-dimensional graph allowing the best separation of the healthy volunteers and patients groups was selected.
Results
Patients’ description
Descriptive data for the healthy volunteer group and the patient group are summarized in Table 1. These data include the age of the participants as well as the male–female ratio. All the participants were of Caucasian origin. No patient had an autoimmune disease nor was under immunosuppressant therapy. Twelve patients did not have any comorbidities or treatment, 17 patients had an underlying treated psychiatric condition (i.e., burnout and depression), 19 patients had allergies, 7 patients had gastrointestinal conditions (i.e., gastritis and gastroesophageal reflux), 2 patients had metabolic syndrome, and 1 patient had hypothyroid. A Mann–Whitney test shows a significant difference between the median ages of the two groups (p < 0.05).
Descriptive Statistics for Age and Male–Female Ratio
PASC, postacute sequelae of SARS-CoV-2 infection.
Neurocognitive symptoms were the most frequent predominant symptoms (38%) followed by the feeling of physical fatigue (30%). The association of multiple symptoms was also frequent in our cohort. The co-occurrence network (Fig. 2) shows the association of symptoms for our patients, without taking into account the predominance of the symptoms. Fatigue was the most frequent symptom followed by the neurocognitive symptoms, commonly called “brain fog” and dysautonomia. The association of these three symptoms was the most frequent. The distribution of symptoms between men and women was homogenous.

Co-occurrence network of the symptoms of patients with PASC. The diameter of the circle and the width of the line are proportional to the frequency of the symptoms and the frequency of the association between two symptoms, respectively. PASC, postacute sequelae of SARS-CoV-2 infection; POTS, postural orthostatic tachycardia syndrome; RHV, respiratory hyperventilation.
Comparison of cytokine levels between patients and healthy volunteers
After overnight stimulation, the levels of 12 cytokines were measured in the supernatant using the chemiluminescence immunoassay (CLIA) multiplex method. No significant differences in cytokine levels were observed among healthy volunteers, between those with a history of acute COVID-19 and the ones without (data not shown). The levels of two cytokines were significantly higher in men compared with women: IL-10 after LPS 10-9 stimulation and TNFα after R848 stimulation (data not shown).
Concerning the comparison of the cytokine level between the group of patients and the group of healthy volunteers, the results are summarized in Table 2. The Mann–Whitney test reveals the presence of significantly higher levels of the following cytokines in patients complaining of PASC symptoms when compared with healthy volunteers:
p-Values for the Comparison of Cytokine Levels Between Patients and Healthy Volunteers
The light gray cases represent the cytokines for which the level is decreased in patients compared with healthy volunteers. The dark gray cases represent the cytokines for which the level is increased in patients compared with healthy volunteers.
p < 0.05.
IFN, interferon; IL, interleukin; LPS, lipopolysaccharide; TLR, Toll-like receptor; TNF, tumor necrosis factor.
IL-1α, IL-1β, IFNα, IFNω, IFNγ, and TNFα after stimulation of the TLR7/8 pathway with R848 (p < 0.05*) (Fig. 3).
IL-1α, IL-1β, IL-2, IL-10, IFNα, IFNγ, and TNFα after stimulation of the TLR4 pathway with LPS at the highest concentration (p < 0.05*) (Fig. 4).
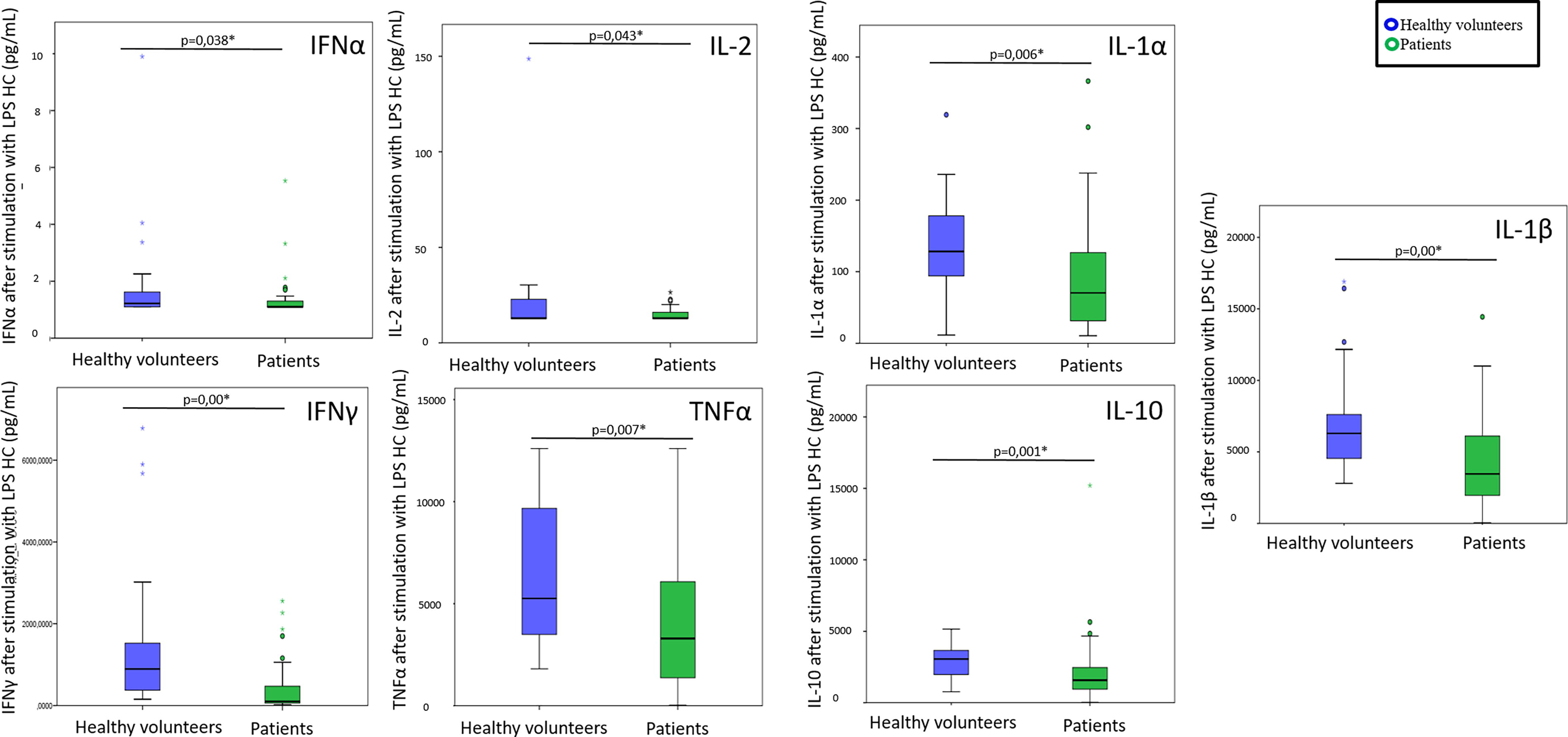
IL-1α, IL-1β, IL-2, IL-10, IFNα, IFNω, and IFNγ after stimulation of the TLR4 pathway with LPS at the lowest concentration (p < 0.05*) (Fig. 5).
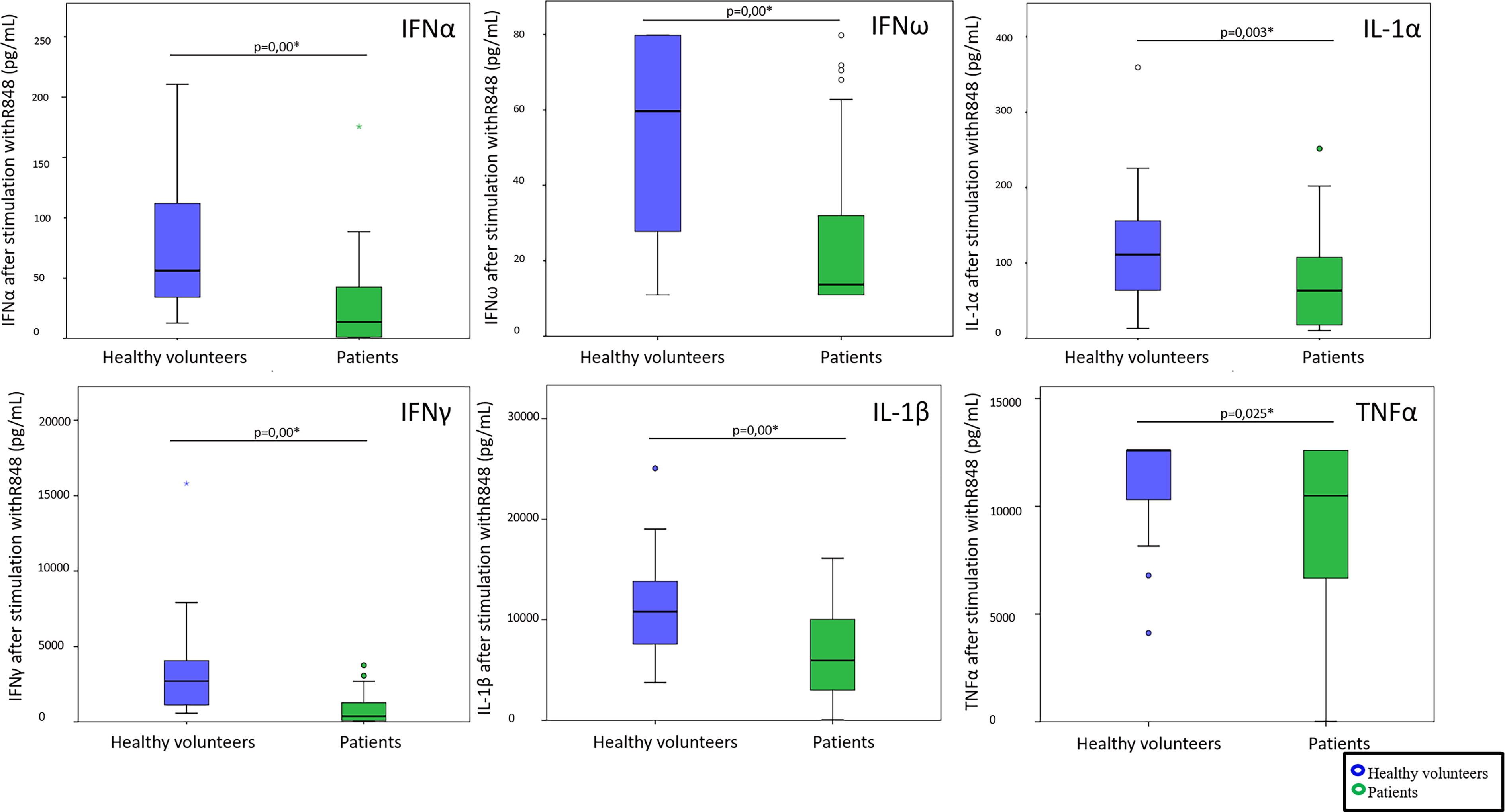
Cytokine levels after stimulation of the TLR7/8 pathway with R848. The blue box represents the healthy volunteers, and the green box represents the patients. TLR, Toll-like receptor. Color images available online at www.liebertonline.com/vim
Cytokine levels after stimulation of the TLR4 pathway with LPS at the highest concentration. The blue box represents the healthy volunteers, and the green box represents the patients. HC, high concentration; LPS, lipopolysaccharide. Color images available online at www.liebertonline.com/vim

Cytokine levels after stimulation of the TLR4 pathway with LPS at the lowest concentration. The blue box represents the healthy volunteers, and the green box represents the patients. LC, low concentration. Color images available online at www.liebertonline.com/vim
Multivariate analysis of the poststimulation cytokine profile for different TLR pathways
The first PC analysis takes into account the parameters that significantly differ between the patients group and the healthy volunteers group after stimulation of the TLR7/8 pathway and summarizes them into two independent main axes. For PC1, the levels of IL-1β, IFNα, and IFNω are the parameters with the greatest degrees of significance (Fig. 6).

Summary of the results of the principal component analysis.
The second PC analysis takes into account the parameters that significantly differ between the group of patients and the group of healthy volunteers after stimulation of the TLR4 pathway with LPS and summarizes them into four independent axes. For PC1, IL-1β levels after stimulation at both concentrations of LPS, TNFα, and IL-1α at the highest concentration are the parameters with the greatest degrees of significance (Fig. 6).
Finally, a graph combining the PC1s of each PC analysis is generated (Fig. 6).
We notice that, despite a slight overlap, the cluster representing the patients, in green, stands out from that of the healthy volunteers group, in blue.
A PC analysis restricted to a group of patients does not allow separating patients according to their symptomatology or the duration of symptoms (data not shown).
The boxplot representation of variables generated by PC1 of each PC analysis shows a clear decrease in values in the patients group compared with healthy volunteers (p < 0.05*) (Fig. 5). This is in agreement with the results of the Mann–Whitney test that shows significantly lower levels of cytokines after TLR7/8 and TLR4 pathways stimulation in patients complaining of PASC.
Discussion and Conclusion
The impact of PASC on quality of life is now clearly established. Work incapacity due to PASC symptoms affects ∼38% of patients with PASC and results in a reduction in quality of life and a significant cost to society (Centers for Disease Control and Prevention, 2020; O’Mahony et al., 2022). Symptoms improve over time in some patients, but adequate care and effective treatment remain necessary. In order to implement an optimal strategy against PASC, it seems essential to clarify, on the one hand, the definition of this disease and, on the other hand, the underlying mechanism. This is all the more important as the effect of vaccination on PASC is difficult to assess. Indeed, if large-scale vaccination against SARS-CoV-2 has shown a very positive impact on the occurrence of severe forms of COVID-19, the impact of this vaccination on PASC remains unknown for the moment (Centers for Disease Control and Prevention, 2020; Watson et al., 2022). The majority of studies relating to PASC were carried out during the third wave of COVID-19, that is, between October 2020 and March 2021. At that time, vaccination was still not widespread, and vaccination schedules were often incomplete. Furthermore, the numerous mutations of the virus introduce a significant bias into the interpretation of most studies of PASC. It is therefore difficult to differentiate the effect of vaccination, the impact of a less virulent strain, and the effect of time on PASC symptoms.
In our study, the cytokine release after in vitro stimulation of TLRs shows significant differences between the group of healthy volunteers and the group of patients, particularly following TLR4 and TLR7/8 activation. Notably, the levels of cytokines after stimulation are observed to be lower in patients compared with those in the volunteers group.
In our study, in basal condition (presence of the RPMI and antibiotic mixture), we did not observe any significant difference between the group of patients and the group of healthy volunteers. However, most studies focusing on the cytokine profile in patients with PASC have shown a continuous activation of the immune system in the basal state: the dosage of cytokines having been carried out without prior in vitro stimulation (Bellan et al., 2022; Queiroz et al., 2022; Schultheiß et al., 2022). Our study is, to our knowledge, the first study to analyze the effect of TLR stimulation in patients with PASC.
The results obtained in this study of cytokine levels after stimulation of TLRs seem to favor a dysregulation of immunity, which is in agreement with the current literature. A study by Brauns et al., published in 2022, described a decrease in the synthesis of numerous proinflammatory cytokines in patients with severe and very severe forms of COVID-19, during the acute phase, after in vitro stimulation of TLR4 and TLR7/8 (Brauns et al., 2022). The differences observed after targeted stimulation of TLR4 and TLR7/8 in our study further indicate an involvement of these TLR pathways in the pathophysiology of PASC. This substantiates the involvement of these two TLR pathways in immune activation in the presence of SARS-CoV-2 over both the short and the long term.
In our study, the median age of the patient group differs significantly from that of the healthy volunteers group but remains below the age limit from which the immunosenescence phenomenon is described (Aw et al., 2007). Thus, it seems unlikely that the age difference between these two groups would bias the results observed. Furthermore, the age of patients complaining of PASC is consistent with the cases described in the literature (O’Mahony et al., 2022; Peter et al., 2022). The decrease in the levels of cytokines secreted after in vitro stimulation of TLRs in patients with PASC could be explained by the fact that, in these patients, we observe significant and continuous basal activation. This continuous stimulation of the innate immune system might be related to viral persistence, as recently demonstrated (Machkovech et al., 2024). It has been suggested that continuous and chronic activation of TLRs could cause a decrease in their expression on the cell surface. Downregulation of certain TLRs expression on the surface of cells has, for example, been suggested as a mechanism for the hepatitis C virus to escape from the innate immune system or as a mechanism for tolerance to bacterial LPS at the intestinal level. Therefore, it seems possible that the expression of TLRs on cell surfaces or endosomes is reduced in patients with PASC (Chang et al., 2010; Kayesh et al., 2022; Sato et al., 2007; Ueda et al., 2010). Such downregulation could explain the diminution in the responsiveness amplitude of TLRs to specific agonists.
In the aging population and in people living with HIV (PLWH), it has been demonstrated that constant basal activation of the immune system leads to a dysfunction of both innate and adaptive immune responses. For example, aging people and PLWH have increased susceptibility to infections and decreased efficacy of vaccination compared with healthy volunteers (Lee et al., 2022, 2023; Tortellini et al., 2023). The findings of our study suggest that PASC might also lead to an immune dysfunction in people living with the disease.
In conclusion, PASC is a multisystemic pathology that has a deleterious impact on the patients’ quality of life, thereby generating a significant cost for society. Several hypotheses are proposed concerning the underlying pathophysiological mechanisms. Immune dysregulation seems to be strongly involved, as for acute COVID-19.
Our study suggests the participation of TLR4 and TLR7/8 pathways in the pathophysiology of PASC. Continuous basal activation of immunity could explain the high basal concentrations of cytokines described in these patients and the decreased response amplitude of these signaling pathways following specific stimulation. Long-term monitoring of these patients, until symptoms eventually disappear, would be necessary in order to prove the causal link between the dysregulation of immunity and the persistence of symptoms.
Footnotes
Acknowledgments
The authors gratefully acknowledge all the laboratory staff for their technical help.
Authors’ Contributions
N.G.: Writing—reviewing and editing, methodology, and data collection. A.P.: Methodology and formal analysis. T.B.-H. and A.R.: Conceptualization. F.C.: Conceptualization, methodology and supervision, and project administration. C.N.: Conceptualization, methodology, and supervision. All authors have read and agreed to the published version of the article.
Data Availability Statement
Data will be available upon request.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This study was funded by the Foundation Brugmann grant 2020.