
Abstract
The corona virus disease-2019 (COVID-19) pandemic has affected most of the world with varying degrees of morbidity and mortality. The presence of genetic polymorphisms may be associated with the severity and outcome of COVID-19 infection. This work aimed to evaluate the genetic polymorphisms of interleukin (IL-6) and IL-10 genes with the outcome of COVID-19 infection. This cross-sectional study was conducted on 354 patients who were classified into moderate and severe cases (including alive and deceased cases). All individuals were genotyped for one SNP for IL-6 (rs1800795) and one SNP for IL10 (rs1800896) using allelic discrimination real-time PCR technique. In this study, 198 cases were moderate, and 156 cases were severe. The risk of allele carriage of the minor allele of IL-6 rs1800795 (C) was significantly higher among the severe group when compared with that of the moderate group (p < 0.0001), while there was a mild significant difference of same allele carriage among alive cases when compared to that of deceased one (p < 0.04). Furthermore, the risk of the C allele of IL-10 rs1800896 was significantly increased in severe cases when compared with the moderate group (p < 0.0001), while there was no significant difference of the risk of the C allele in deceased cases when compared with that of alive ones (p > 0.05). In conclusion, the C allele (rs1800795) of IL-6 and the C allele (rs1800896) of IL-10 were highly significant in severe cases than in moderate cases. The C allele carriage of IL-6 showed only a significant difference between alive and deceased patients and not with the C allele of IL-10.
Introduction
The World Health Organization’s (WHO’s) declaration of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [corona virus disease-2019 (COVID-19)] as a worldwide pandemic has since been associated with varying degrees of morbidity and mortality (McIntosh et al., 2020). The causative culprit has been identified by phylogenetic analysis to be a novel virus relatively similar to the SARS-like coronavirus (genus Betacoronavirus) which originated from bats in China (Zhou et al., 2020b). Although similar to diseases caused by other coronavirus family members, such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) (Nandy et al., 2020), infection with COVID-19 is associated with a multitude of respiratory and nonrespiratory symptoms, namely, cardiac, neurological, gastrointestinal, and thromboembolic, often necessitating patient admission into the intensive care unit (ICU) (Bi et al., 2020, Zhou et al., 2020a).
International guidelines for diagnosis of COVID-19 require findings of positive PCR and suggestive radiology. However, it had been determined that ICU-admitted patients with COVID-19 pneumonia exhibit an increase in immunological and chemical biomarkers related to inflammation, such as cytokines, chemokines, and TNF-α when compared with more mildly affected cases (Bi et al., 2020, Rokni et al., 2020c). Although the outcome of COVID-19 infection is determined by a number of viral and host factors, including viral load, duration of infection, and viral mutations as well as patient age, gender, comorbidities, and genetic background, whether there is a relationship between inflammatory markers and infection severity remains unclear (Karcioglu Batur and Hekim, 2021, Rokni et al., 2020b).
It has been proposed that host genetic polymorphism may partake in the pathogenesis of COVID-19, thereby contributing to the severity and prognosis of infected patients (Liu et al., 2020). This study attempted to evaluate the association between genetic polymorphism of interleukin (IL-6) and IL-10 with the outcome of COVID-19 infection.
Patients and Methods
This cross-sectional study was conducted on 354 inpatients hospitalized at Mansoura University Isolation Center for COVID-19. They were classified according to the WHO scale into moderate (WHO scale 1–4) and severe (WHO scale 5–8). Severe cases were further classified according to the outcome into alive cases and deceased cases. All patients above the age of 18 years with definitive nasopharyngeal swab testing positive for SARS-CoV-2 using viral RT-PCR [in the Molecular Genetic Unit of Endemic Hepatogastroenterology and Infectious Diseases (MGUHID), Mansoura Faculty of Medicine] and chest computed tomography indicative of pneumonia were included. Exclusion criteria were the presence of fever and respiratory symptoms despite negative PCR for SARS-CoV-2. All individuals were genotyped for one SNP for IL6 (rs1800795) and one SNP for IL10 (rs1800896) using allelic discrimination real-time PCR technique. The research design of this study adhered to the guidelines outlined in the Declaration of Helsinki and received ethical approval from the Medical Research Ethics Committee Institutional Review Board Mansoura Faculty of Medicine, Mansoura University (R.20.05.830). Every method was executed in strict adherence to the approved guidelines. Before commencing the investigation, written informed consent was obtained from everyone who participated.
Sampling
Blood samples of 10 mL were drawn from each participant and then divided into four different blood tubes as follows: sterile EDTA tube, plain tube, citrate blood tube, and EDTA blood tube.
Biochemical investigation
Complete blood count was performed on 1 mL EDTA blood sample using Sysmex XP-300™ Automated Hematology Analyzer. Routine biochemical tests, including liver and renal function tests, were conducted using commercial kits (ELITech, Puteaux, France) and (Human, Germany), respectively. The degree of inflammation was evaluated by C-reactive protein (CRP) determination in serum, and values of D-dimer and international normalized ratio (INR) were also recorded.
Molecular biology
The molecular studies were conducted in the MGUHID at the Faculty of Medicine of Mansoura University.
DNA extraction
Qiagen DNA isolation kit (QIAamp DNA Mini kit; Qiagen, Hilden, Germany) was used to extract DNA for each participant from 5 mL of sterile EDTA patient blood according to the manufacturer’s instructions. Following extraction, the concentration and purity of DNA were examined using NanoDrop spectrophotometer (NanoDrop™2000/2000c spectrophotometer, Thermo Scientific, CA).
Genotyping
Polymorphisms of IL-6 and IL-10 genes included in the study are summarized in Table 1.
Polymorphisms of IL-6 and IL-10 Genes Included in the Study
IL, interleukin.
Each well contains a total volume 15 μL consisting of 6 μL TaqMan™ Genotyping Master Mix (Applied Biosystems™), 5.4 μL sterile H2O, 0.6 μL readymade genotyping assay (Thermo Scientific, CA) and 3 μL of DNA sample. Allelic discrimination was performed using real-time PCR (Applied Biosystems, 7500) incorporating the thermal profile of enzyme activation for 10 min at 95°C followed by 50 cycles of denaturation at 95°C for 15 sec to end with the annealing/extension step at 60°C for 1 min. Ten percent of samples were genotyped by two independent researchers to ensure the quality of the result. The data were exported as an Excel file, and allele carriages and frequencies were counted in each group.
Statistical Methods
Version 23 of the Statistical Package for Social Sciences (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.) was used to enter and analyze data for this study. Mean and standard deviation were used to present parametric quantitative data with nonparametric variables presented as median and tested for significance using the Mann–Whitney test. Qualitative data were displayed as number and percent and compared between groups using the Pearson Chi-square (χ2) test. Hardy Weinberg equilibrium was assessed in each group separately using χ2 tests. The allele carriage is defined as the number of individuals carrying at least one copy of a specific allele. Allelic frequencies are defined as the number of occurrences of the test allele divided by the total number of alleles in the group. The odds ratio at 95% confidence interval (CI) of the specific allele carriage was calculated compared with the noncarriage of the target allele using MedCalc software. Statistical significance was determined at p-value ≤ 0.05.
Results
Tables 2 and 3 show the demographic, clinical, and laboratory data of the studied cases. The mean age of patients was 56 years with 58.2% of them being males. Fever and dry cough were the commonest symptoms: 49.4% of patients were admitted to ICU. According to the WHO assessment at admission, patients were classified into moderate cases (198, 55.9%) and severe cases (156, 44.1%), where the mortality among severe cases at discharge were 33 cases (21.2%), whereas the alive cases were 123 cases (78.8%).
Demographic and Clinical Characteristics of Studied Patients (354)
Mean ± SD, mean ± standard deviation; WHO, World Health Organization.
Biochemical and Laboratory Data of Studied Patients (354)
Mean ± SD, mean ± standard deviation; SO2, saturation of oxygen; TLC, total leukocytic count; INR, international normalized ratio; ALT, alanine transaminases; AST, aspartate transaminases; CRP, C-reactive protein.
Table 4 shows the comparison of demographic and clinical data between moderate and severe cases. It reveals that severe cases significantly associated with age ≥60 years, presence of diabetes with other comorbidities, and low oxygen saturation more than moderate cases (p < 0.01).
Comparison of Demographic and Clinical Data Between Moderate and Severe Cases
COR, crude odds ratio; CI, confidence Interval; r, ratio.
For example, cardiac and bronchial asthma.
Table 5 shows the comparison of demographic and clinical data between alive and deceased cases. No difference between the two groups with regard to age, sex, DM, hypertension, and other comorbidities. Only mean SO2 was shown to be significantly lower in deceased patients more than in alive cases (79.1 versus 86) (p < 0.001).
Comparison of Demographic and Clinical Data Between Alive and Deceased Cases
COR, crude odds ratio. n, number
For example, cardiac and bronchial asthma.
Table 6 shows the SNPs of IL-6 rs1800795 (G/C) and IL-10 rs1800896 (T/C) genes genotyped from 354 COVID-19 patients with different stages of the disease. Both SNPs were located in the nontranslated regions of both genes. The allele frequency of rs1800795 (C allele) was 0.23 compared with 0.14 among the global population, whereas that of rs1800896 (C) was 0.18 compared with 0.27 globally (global data stratified from SNPedia https://www.snpedia.com).
Demographic Distribution of Different Alleles of Selected SNPs in Different Groups
M/H/N, number of homozygous individuals carriage major allele/number of heterozygote/number of minor allele homozygote; AJ, major allele; AI, minor allele; MAF, minor allele frequency.
Table 7 and Figure 1 show the risk of carriage of the minor allele for severe and moderate groups in both autosomal dominant and recessive modes of inheritance. The risk of carriage of the minor allele of IL-6 rs1800795 (C) was significantly higher in the severe COVID-19 group when compared with the moderate group in both models of inheritance (dominant OR: 4.9656, CI: 3.2128–7.6747, p < 0.0001, whereas recessive OR: 6.0854, CI: 2.7211–3.6094, p < 0.0001). A slightly significant difference in the C allele carriage of IL-6 rs1800795 was found in the alive group when compared with the deceased group in both models of inheritance (dominant OR: 2.1549, CI: 1.0057–4.6172, p < 0.0483, whereas recessive OR: 2.6961, CI: 1.1447–6.3500, p < 0.0233), indicating that the C allele of IL-6 rs1800795 may play a pivotal role with the severity and outcome of COVID-19-infected patients (Fig. 1A). Similarly, the risk of carriage of the IL-10 rs1800896 C allele was significantly increased in severe cases than in moderate cases in both the model of inheritance (dominant OR: 3.6410, CI: 2.4063–5.5092, p < 0.0001, whereas recessive OR: 3.2285, CI: 1.7101–6.0951, p < 0.0003). However, no significant difference in risk of the C allele carriage was detected between the alive and deceased groups of patients in both dominant (OR: 2, CI: 9114–4.3890, p < 0.0839) and recessive models (OR: 2.0912, CI: 0.8764–4.9895, p < 0.0964), indicating that IL-10 may promote morbidity but not mortality of this infection (Fig. 1B).
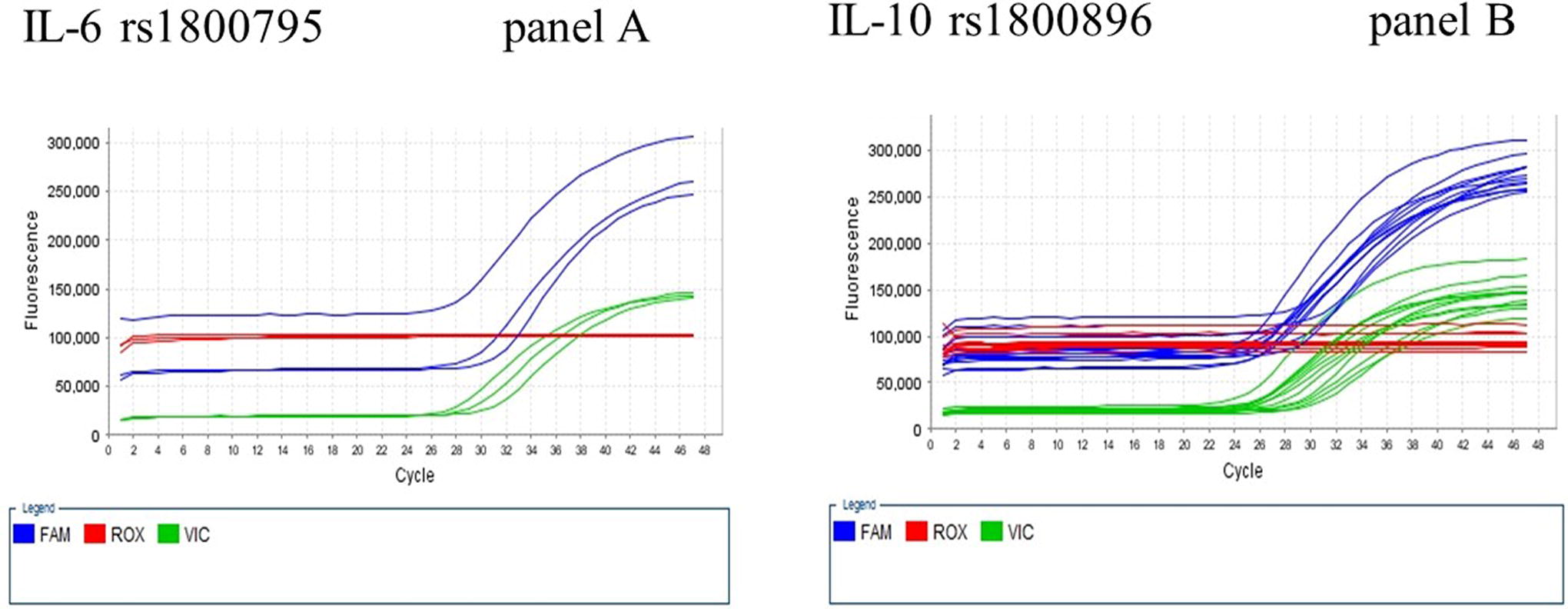
Multicomponent plot of allele discrimination software.
Association of IL-6 and IL-10 SNPs in Different Groups both in Autosomal Dominant and Recessive Models
IL, interleukin; vs, versus; OR, odds ratio; CI, confidence interval; p, p-value.
Discussion
Corona viruses such as SARS-CoV, MERS-CoV, and the novel SARS-CoV-2 are commonly associated with acute respiratory distress syndrome as an immunopathological consequence to the cytokine storm resultant from these infections (Martinez-Ocaña et al., 2013). SARS-CoV infection results in a massive systemic inflammatory response, whereby effector cells release immense amounts of proinflammatory cytokines such as interferon (IFN)-α and -γ, TNF-α and -β, and ILs 1, 6, and 12, as well as chemokines including CCL2, 3, and 5, and CXCL8, 9, and 10 (Huang et al., 2020, Heidari Nia et al., 2022). Similarly, patients infected with severe MERS-CoV also demonstrate significantly elevated levels of IL-6, IFN-α, CCL5, and CXCL8 and 10 when compared with milder or moderate forms of the disease (Song et al., 2019, Rokni et al., 2020c).
Patients with COVID-19 infection, especially if severely or critically ill, were found to exhibit increased levels of the inflammatory cytokine IL-10 (Diao et al., 2020). Hence, IL-10 was recently identified in a meta-analysis of 18 clinical studies on COVID-19 to be a covariate to accurately predict the outcome of disease severity in these patients (Dhar et al., 2021). Likewise, an increased IL-6 level has also been associated with a higher incidence of mortality in severe COVID-19 infection and more advanced chest CT findings, whereas recovered patients showed lowered IL-6 levels with improvement in CT radiography (Zhang et al., 2020, Liu et al., 2020).
The present study showed that several factors are implicated in the progression of severe COVID-19. Zhang et al. conducted a meta-analysis showing that the risk of progression of COVID-19 infection was higher in patients who had radiological findings of bilateral pneumonia, with mortality more commonly being associated with symptoms such as increased sputum production and hemoptysis in addition to increased CRP and total bilirubin (Zhang et al., 2021). Another European study similarly identified symptoms such as fever and dyspnea to be more prevalent in moderate-to-severely infected COVID-19 patients (Lechien et al., 2020, Rokni et al., 2020a), whereas advanced age ≥75 years was found to be a risk factor for mortality by Feng et al. (Feng et al., 2020).
Numerous studies have shown an association between chemokines and proinflammatory interleukins, especially IL-6 polymorphism with different viral infections, both respiratory, such as influenza and respiratory syncytial virus (RSV), and nonrespiratory, such as HBV and HCV (Attallah et al., 2018, El‐Bendary et al., 2017, El-Bendary et al., 2019, Elsayed et al., 2017, El-Bendary et al., 2015). In fact, IL-6 polymorphism represents one of the most important valid indicators of the severity of COVID-19 infection. The current study showed that the risk of allele carriage of the minor allele of IL-6 rs1800795 (C) was significantly higher in the severe group compared with the moderate group in both models of inheritance (p < 0.0001).
Previous studies have shown an association between IL-6-174 CC genotype (rs1800795) and severe RSV (Doyle et al., 2010). The immunogenetic effect of IL-6 polymorphism on respiratory and nonrespiratory viral diseases may provide the basis to establish new therapeutic modalities and vaccinations for COVID-19 (Kirtipal and Bharadwaj, 2021). Although this polymorphism is not directly correlated with COVID-19 pneumonia infection, it has been shown that patients with severe pneumonia who are carriers of the IL-6-174C allele also demonstrate increased levels of IL-6 (Karcioglu Batur and Hekim, 2021, Martinez-Ocaña et al., 2013, Ulhaq and Soraya, 2020).
To avoid the host immune response, SARS-CoV and MERS-CoV employ a number of different strategies. In general, host pattern recognition receptors (PRR) recognize microbial structures known as pathogen-associated molecular patterns (El-Bendary et al., 2018, Neamatallah et al., 2020). However, a study on Chinese patients with pneumonia-induced sepsis showed that the IL-6 rs1800795 G allele may have acted as a protective factor, whereas the IL10 rs1800896 A allele possibly was an indicator of risk (Mao et al., 2017). An important role of the IL-6 C allele and IL-6R CC genotype on COVID-19 severity was reported by other authors in Amazonian (Rodrigues et al., 2023) and Iranian populations (Rokni et al., 2022). On the other hand, Falahi et al. (2022) found that there were no significant differences in the genotype or allele distribution of selected IL-6 SNPs (rs1800795) in patients with severe or mild COVID-19 (Falahi et al., 2022).
Furthermore, in addition to being associated with the clinical stage of sepsis in the patients, these polymorphisms also appeared to significantly influence the secretion of IL-6 and IL-10 (Liu et al., 2020). In the Egyptian population, the severity of COVID-19 has been shown by genotyping analysis to be strongly associated with IL-10 (rs1800872) gene polymorphism although IL-10 rs1800896 polymorphism conveyed no such risk of severity (Rizvi et al., 2022). Regarding SARS-CoV and MERS-CoV, these viruses induce the production of double-membrane vesicles lacking PRRs followed by replication within these vesicles, thus avoiding detection of their dsRNA by the host. Type I interferons (IFN-α and IFN-β) are protective against SARS-CoV and MERS-CoV, although they are inhibited in infected mice. Sheikhi et al. (2023) showed that COVID-19 severity is related to the IL-10 (rs1800872) gene polymorphism, with the GA genotype providing protective effects but not with IL10 rs1800896 (Sheikhi et al., 2023). On the other hand, Abbood et al. (2023) found that the COVID-19 mortality rate was associated with the IL10 rs1800896 GG and AG genotypes in the Delta and Omicron BA.5; nevertheless, there was no association between rs1800896 polymorphism with the Alpha variant (Abbood et al., 2023). Furthermore, Karcioglu Batur and Hekim (2021) searched the literature for polymorphisms of the prevalence of COVID-19, and the mortality rates in 23 countries revealed that there was no significant correlation between the prevalence (per million), mortality rates (per million), and the frequencies of polymorphisms found in IL-6 and IL-6R genes, but significant positive correlation between the frequency of the AG genotype of IL-10 (rs1800896) and the prevalence of COVID-19 was recorded on December 6, 2020 (Karcioglu Batur and Hekim, 2021).
In conclusion, the C allele of IL-6 rs1800795 was highly significant in severe when compared with moderate cases and moderately significant in deceased patients when compared with alive cases. The risk of the C allele of IL-10 rs1800896 was significant only in severe cases versus moderate cases with no difference detectable between alive and deceased groups. Limitations of the study included a larger sample size by multicenter studies is needed to validate the results. More funding is also needed to overcome the cost of the study.
Footnotes
Acknowledgments
The authors thank Dr. Dina El-Hammady (native English speaker) for language editing of the article.
Ethical Approval and Consent to Participate
The Institutional Review Board of Mansoura Faculty of Medicine approved this study, and written informed consent was obtained from all patients. All experimental procedure complied with the Declaration of Helsinki.
Data Availability
The datasets used and analyzed during this work are available from the corresponding author upon reasonable request.
Authors Contributions
M.B. and M.N. were involved in study conception and design. M.B. wrote the article. A.G. acquired, analyzed and interpreted the data. M.N., H.Z., and S.A. performed laboratory and molecular genetic study. H.E., A.H., and M.E. contribute in the recruitment of cases and their clinical diagnosis. All authors were involved in the drafting and critical revision of the article. All authors approved the final version of the article.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This research was funded by Mansoura Research Unit-competitive funding projects, Graduate Studies Research and Cultural Affairs, Mansoura University, Egypt.