
Abstract
The current study investigates COVID-19 infection likelihood using data from 5,819 respondents in Vietnam and Indonesia (December 10, 2022, to March 27, 2023) through binary logistic regressions. Descriptive statistics highlight the significance of vaccination status, with almost half of unvaccinated respondents contracting the infection. The second vaccine dose showed the lowest infection percentages, suggesting a potential dose-dependent effect. Those receiving mRNA vaccines consistently had reduced infection likelihood across the first four doses, with an unexpected reversal for the fifth dose. Vaccinated individuals, especially with mRNA vaccines, had faster recovery times, and variability in recovery times and milder symptoms were observed in mRNA vaccine recipients. Regression results from Model 1 reveal a substantial impact of vaccination, with vaccinated respondents having ∼48.1% lower odds than the unvaccinated. Model 2 underscores a dose-dependent protective effect, with each additional dose associated with a notable 6.6% reduction in infection likelihood. Beyond vaccination, gender, family size, marital status, employment, urban residence, and nationality influenced infection likelihood. Males, larger families, single marital status, unemployment, rural residence, and Indonesian nationality increased the likelihood of infection. Surprisingly, respondents with infected family members exhibited a lower infection likelihood, suggesting potential protective measures within households. These findings highlight COVID-19 dynamics, and ongoing research refines comprehension.
Introduction
The COVID-19 pandemic has significantly impacted Southeast Asia, affecting both public health and the economy (Chu et al., 2022 Fraser, 2022, Kretchmer, 2020, Ozili and Arun, 2023, Searight, 2020, Worldometer, 2022e). Southeast Asia comprises a diverse group of countries with varying levels of health care infrastructure and public health resources (Sharma et al., 2021, World Bank, 2022). The region has faced unique challenges during the pandemic, including densely populated urban areas, limited access to vaccines, and varying degrees of public health compliance (Rasul et al., 2021, Wang et al., 2021, Wouters et al., 2021). The economic impact has also been profound, with significant disruptions to trade, tourism, and labor markets, exacerbating existing inequalities and straining health care systems (Chong et al., 2021). Despite extensive vaccination efforts, the region continues to experience high daily death rates, with ∼3,574 deaths per day and transmission rates nearing 120,704 new cases daily (WHO, 2022). Understanding the factors contributing to the COVID-19 infection is crucial for developing effective public health strategies to contain its spread and mitigate the impact of similar viruses in the future.
Numerous studies have evaluated the effectiveness of various COVID-19 vaccines, typically focusing on a two-dose regimen administered at different dosage levels and intervals, addressing a range of viral variants and utilizing clinical observations and randomized trials (Fiolet et al., 2022, Frenck et al., 2021, Polack et al., 2020, Pritchard et al., 2021, Roy et al., 2020, Thompson et al., 2021a, Thompson et al., 2021b). However, many of these studies lack regression analysis results and fail to comprehensively explore the multifaceted factors influencing COVID-19 infection.
This study aims to fill these gaps by examining the influence of vaccination status and dose count on the likelihood of COVID-19 infection in Southeast Asia, a region where health care facilities may be less advanced. Additionally, it investigates the complex relationships between vaccination status, specific vaccine brands, dosage levels, and the likelihood of hospitalization, recovery duration, or symptom severity postinfection. By providing a more detailed understanding of these factors, this research seeks to inform public health strategies and improve the region’s response to current and future pandemics. This study is particularly important because it addresses a critical gap in the existing literature: the specific context of Southeast Asia. By focusing on this region, the study acknowledges the unique epidemiological, socioeconomic, and health care factors that influence COVID-19 transmission and vaccine effectiveness. Understanding these nuances is vital for tailoring public health strategies that are contextually relevant and effective.
Materials and Methods
Research design
The sample size for the present study is determined using the methodology outlined in Lemeshow et al. (1990), Lwanga et al. (1991), and Nakagawa and Cuthill (2007), which takes into account the prevalence rate of COVID-19-infected people as described in Equation 1.
Stratified sampling was chosen for its benefits, as documented in Acharya et al. (2013) and Singh and Masuku (2014). The primary stratification criterion employed was the division into six socioeconomic regions in Vietnam (GSO, n.d.). Likewise, the primary method of categorization used involved the partitioning of Indonesia into seven geographic regions (Wikipedia, 2022b). Secondary stratification criteria included vaccination status, gender, marital status, and residency. Details of the sampled regions are provided in the Supplementary Data S1.
Questionnaires were created using Google Forms, and dissemination occurred through various channels, including email, social media, and messaging apps. The survey spanned from December 10, 2022, to March 27, 2023, with responses collected and stored in Excel format for analysis. Ethical approval was obtained from the Vietnamese Ministry of Health (reference numbers No: 250/QĐ-ĐĐNC/YTDP/2022 and Protocol/ID: 250/06/22) and the Faculty of Medicine, Universitas Sebelas Maret in Indonesia (reference numbers No: 09/UN27.06.11/KEP/EC/2023 and Protocol/ID: 01/02/12/2022/186). Further information can be found in the Supplementary Data S1.
Research methodologies, models, variable description, and expected outcomes
Participants were queried about their COVID-19 infection status, with response options being “yes” (positively tested, coded as one) or “no” (negatively tested, coded as zero). Given the binary nature of the responses, a binary logistic regression model was employed, as outlined by Harrell, Frank and Harrell (2015), King (2008), Tranmer and Elliot (2008), and Wooldridge (2012). The selection of independent variables was informed by prior research.
The demographic attributes of participants in this study include age (expressed in years), gender (1 = male), place of residence (1 = urban), and nationality (1 = Vietnamese, 0 = Indonesian) (Abedi et al., 2021, Brodin, 2021, Clark et al., 2020, Haas et al., 2021, Hall et al., 2022, Liu et al., 2020, Martin et al., 2020). Older individuals may have a better understanding of the virus and the pandemic, potentially lowering their susceptibility to COVID-19, but they may also face increased risk due to comorbidities (CDC, 2023). Similarly, males may have larger social circles and engage in more outings, increasing their infection risk, while females, often responsible for household tasks such as grocery shopping in Asian cultures, may also face elevated risk. Urban residents, living in densely populated areas, may face a higher risk of infection, but they may also have better access to health care resources and information outlets, resulting in a complex interplay of factors influencing infection likelihood.
In this study, participants’ understanding of the virus and the pandemic was assessed using two key measures: their perceived sufficiency of knowledge regarding five protective measures (vaccination, mask usage, disinfection, avoiding gatherings, social distancing, and health reporting), rated as 1 for sufficient, and their perceived sufficiency of knowledge specifically regarding vaccination (Xu et al., 2020). Those who acknowledged the importance of all five protective measures for preventing infection during severe pandemic situations were categorized as having sufficient knowledge. Similarly, participants who recognized vaccination’s importance regardless of factors such as population vaccination rates or variant virulence were considered to possess adequate knowledge. It is expected that individuals with sufficient knowledge of all five protective measures are likely to have a reduced likelihood of COVID-19 infection, as are those with adequate knowledge about vaccination.
In this study, respondents’ potential exposure to the virus was evaluated based on marital status (1 = married/cohabiting) (Liu et al., 2020), family size (measured by household members) (Hall et al., 2022), employment status (1 = employed) (Baker et al., 2020, Koh, 2020), eligibility for vaccine priority (1 = yes) (OCHA, 2021, VNVC, 2021), the presence of comorbidities (1 = yes) (Clark et al., 2020, Hall et al., 2022, Martin et al., 2020), having a family member eligible for vaccine priority (1 = yes), and having a family member with a history of COVID-19 infection (1 = yes). It is expected that married/cohabiting respondents, those in larger households, individuals in vaccine priority groups, those with comorbidities, those with family members in vaccine priority groups, or those with family members who had COVID-19 would likely have an elevated likelihood of contracting COVID-19. Employed individuals may have more interactions, potentially increasing exposure, but they are also more likely to adhere to protective measures. Hence, the impact of employment status on COVID-19 likelihood is anticipated to be multifaceted.
During the study period, various COVID-19 vaccines were distributed and administered in both countries, as documented by sources including the COVID-19 Vaccine Tracker (2022), HCDC (2021), Wikipedia (2022c), and Wikipedia (2022d). Respondents who received COVID-19 vaccinations were assigned a code of 1, while those who had not were designated otherwise (Hall et al., 2022). The study meticulously documented the number of vaccine doses each participant received, with a maximum of five doses recorded at the time of the surveys. Each vaccine dose administered was meticulously documented, with Pfizer and Moderna vaccines classified as mRNA vaccines and others as “Others.” Regression Model 1 examined vaccination status’s impact on COVID-19 infection likelihood, while Model 2 analyzed the effect of vaccine doses. Vaccinated individuals are expected to have a reduced risk of SARS-CoV-2 infection compared with their unvaccinated counterparts. Additionally, those receiving more vaccine doses are anticipated to have a lower likelihood of contracting COVID-19 (Hall et al., 2022, Thompson et al., 2021a).
This study extensively explored the intensity of symptoms exhibited by respondents who tested positive for COVID-19. At the time of the investigation, COVID-19 infections were associated with 11 prevalent symptoms (CDC, 2022b). To assess symptom severity (Haas et al., 2021), a coding scheme was employed: uninfected respondents were designated as 0, those infected but displaying no symptoms were coded as 1, mild symptoms as 2, moderate symptoms as 3, and severe symptoms as 4. Factors such as likelihood of hospitalization (Haas et al., 2021) and duration of positive to negative test results also indicated the extent of the COVID-19 infection. Further details can be found in the Supplementary Data S1. Figure 1 provides a brief overview of these influential factors.

The conceptual framework for estimating the likelihood of COVID-19 infection. Source: Developed by the authors.
Results
Exploring the interconnection of COVID-19 vaccination with the likelihood of infection and severity of infection
Key research questions explored include the following: Are individuals vaccinated against COVID-19 less susceptible to contracting the virus? Does the number of vaccine doses received influence the risk of infection? Additionally, do vaccinated individuals have lower odds of hospitalization compared with those who were unvaccinated? Figure 2 provides valuable insights into these inquiries.
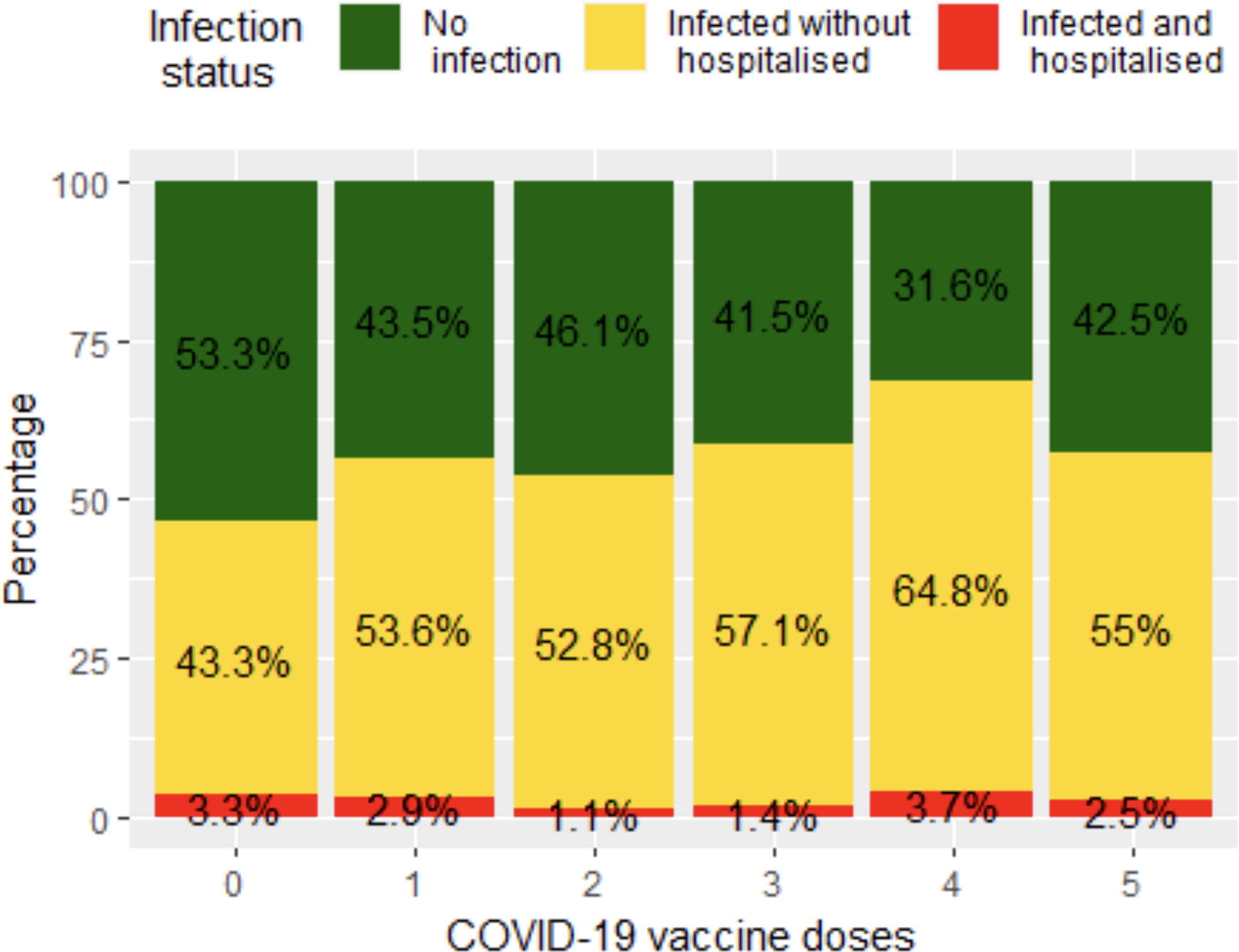
Relationship between COVID-19 vaccine doses and infection and hospitalization status. Source: Illustrated by the authors, using the surveyed data.
Figure 2 reveals nearly half of the unvaccinated respondents contracted the infection. Vaccination status significantly influenced infection rates. The second and third doses had the lowest infection percentages, consistent with Haas et al. (2021) and Thompson et al. (2021a). Specific vaccine brands were not included in this graph.
An intriguing aspect to investigate is whether individuals who received multiple vaccine doses and mRNA vaccines are less susceptible to COVID-19 infection compared with those with fewer doses and other vaccine types. Figure 3 examines if multiple vaccine doses and mRNA vaccines reduce COVID-19 susceptibility. mRNA vaccine recipients had a lower infection risk, consistent with Fiolet et al. (2022) and Haas et al. (2021), particularly for the first four doses. However, a surprising reversal was observed with the fifth dose, necessitating further investigation due to the limited number of respondents receiving it.

Analysis of likelihood of COVID-19 infection in relation to vaccine brands and doses. Source: Illustrated by the authors, using the surveyed data.
Investigating if COVID-19 vaccine recipients have shorter recovery periods than nonrecipients is vital. It is also important to explore recovery duration variations among vaccine brands and doses. In this study, recovery duration measured the transition from positive to negative status, typically 3 days to 3 weeks. Outliers were excluded. Figure 4 shows vaccinated individuals had faster recovery times than unvaccinated. mRNA vaccine recipients had notably shorter recovery times than those with other vaccines. Variability in recovery times was observed across different vaccine doses.
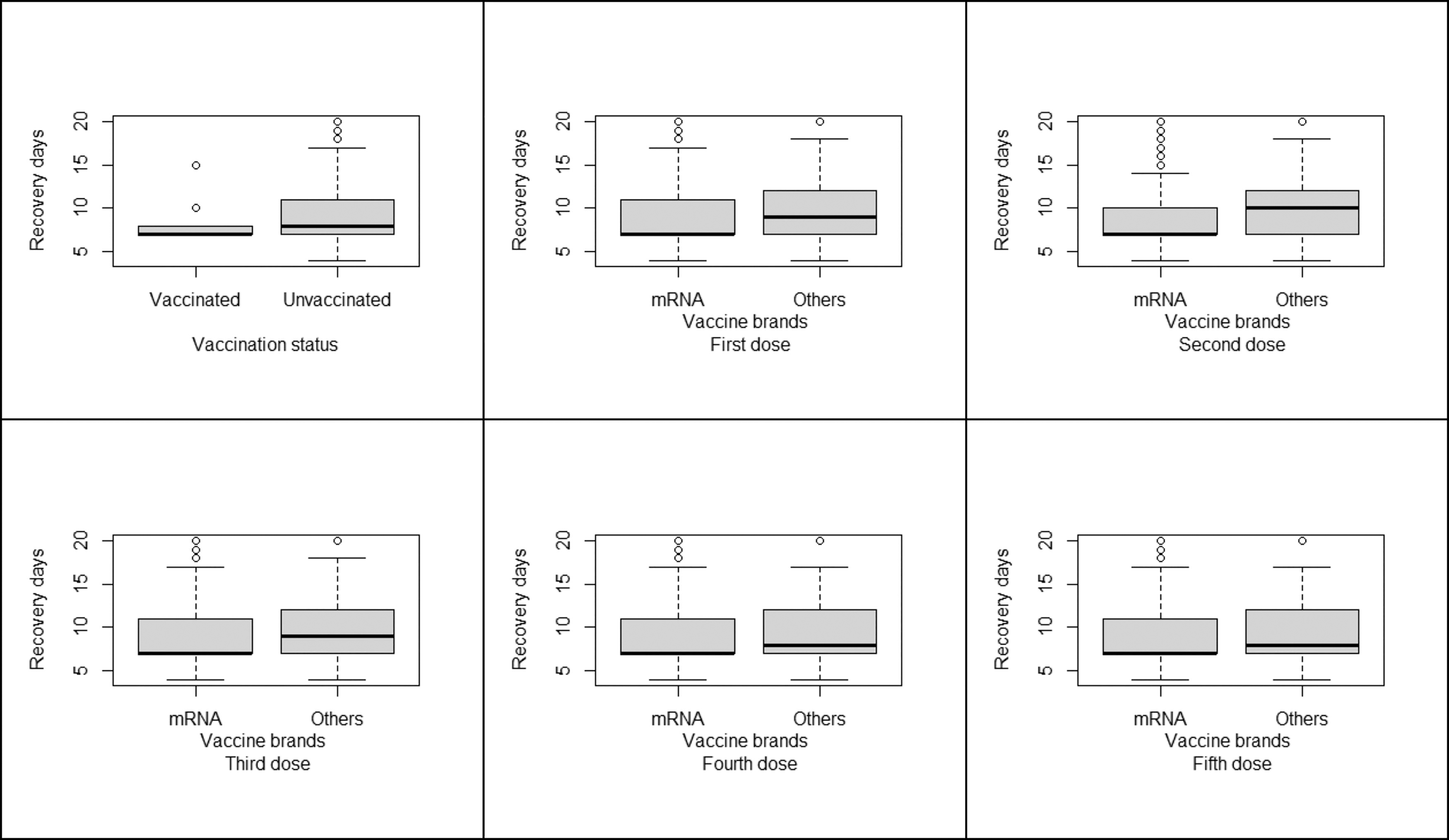
Comparative analysis of recovery duration in relation to COVID-19 vaccination status, vaccine brands, and doses. Source: Illustrated by the authors, using the surveyed data.
Figure 5 shows that the severity of infection-related symptoms appears to be milder in respondents who were vaccinated compared with those who were unvaccinated.
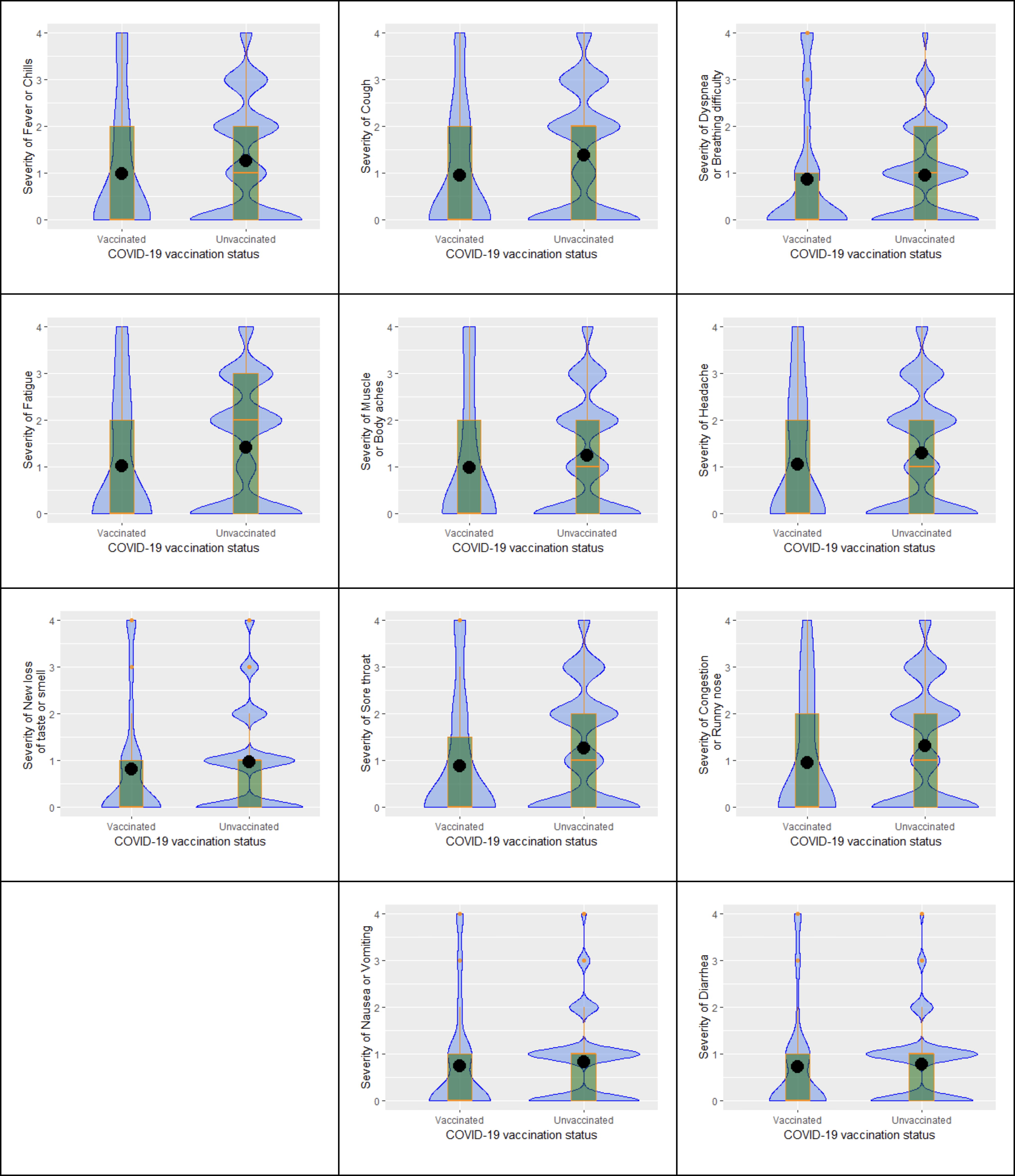
The relationship between COVID-19 vaccination status and the severity of associated infection symptoms. Source: Illustrated by the authors, using the surveyed data.
Assessing COVID-19 infection likelihood in respondents from Vietnam and Indonesia
To ensure the study’s reliability, it is crucial to recognize potential biases and strategies to address them. Endogeneity is a common issue in parametric studies. Techniques such as instrumental variables (IVs) or two-stage least squares (2SLS) help mitigate endogeneity’s impact. However, finding suitable IVs or variables for 2SLS is often challenging (Bascle, 2008, Fingleton and Le Gallo, 2010, Kelejian, 1971, Semadeni et al., 2014, Terza et al., 2008, Ullah et al., 2021). Thus, this study meticulously follows previous research in selecting appropriate independent variables.
Among the 21 factors in the model, the Akaike information criterion (AIC) identified 10 key factors for COVID-19 infection likelihood (Akaike, 1974, Cavanaugh, 1997, Shibata, 1976). The reduced multinomial logistic regression model was thus used as follows:
The AIC-recommended Xi from Equation 3 is detailed in the Supplementary Data. The study examines the impact of vaccination status and dosage on COVID-19 contraction risk using two binary logistic regression models. Results in Table 1 show similar coefficient magnitudes and significance levels in both models.
The Likelihood of COVID-19 Infection among Vietnamese and Indonesian Respondents
Source: Authors’ estimation, using the surveyed data.
B. coefficient (beta); SE, standard error; Sig., significance.
Table 1 shows that male respondents exhibited a higher likelihood of COVID-19 infection. The impact was significant at the 1% level. Particularly, for male respondents in Model 1, the odds of being infected with the SARS-CoV-2 virus are ∼1.326 times or ∼32.6% higher (exp0.282 − 1 = 1.326 − 1) than the odds for their female counterparts when all other variables in the model are held constant. Similarly, for male respondents in Model 2, the odds of being infected with the SARS-CoV-2 virus are ∼1.312 times or ∼31.2% higher (exp0.272 − 1 = 1.312 − 1) than the odds for their female counterparts.
Respondents from larger families had a significantly higher likelihood of COVID-19 infection, with statistical significance at the 1% level. In both Model 1 and Model 2, for each additional person in the family, there was ∼a 6.5% and 6.6% increase in the likelihood of infection, respectively.
Married/cohabited respondents exhibited a significantly lower likelihood of COVID-19 infection compared with those who were single, divorced, widowed, separated, etc., with statistical significance at the 1% level. In both Model 1 and Model 2, individuals who were married or cohabiting showed ∼33.1% and 33.5% lower odds of COVID-19 infection, respectively, compared with the reference group.
Employed respondents had a lower likelihood of COVID-19 infection. The impact was significant at the 1% level. Particularly, for employed individuals (compared with those who were not employed) in Model 1, the odds of being infected with the COVID-19 virus are ∼0.719 times or ∼28.1% lower (1 − exp−0.330 = 1 − 0.719) than the odds for those who were not employed. Similarly, for employed individuals (compared with those who were not employed) in Model 2, the odds of being infected with the COVID-19 virus are ∼0.710 times or ∼29.0% lower (1 − exp−0.343 = 1 − 0.710) than the odds for those who were not employed.
Respondents residing in urban areas showed a significantly lower likelihood of COVID-19 infection compared with those in nonurban areas, with statistical significance at the 1% level. In both Model 1 and Model 2, individuals living in urban areas exhibited ∼22.4% and 22.9% lower odds of SARS-CoV-2 infection, respectively, compared with those in nonurban areas.
Vietnamese respondents exhibited a significantly lower likelihood of COVID-19 infection compared with Indonesians, with statistical significance at the 1% level. In both Model 1 and Model 2, individuals of Vietnamese nationality showed ∼74.1% and 75.6% lower odds of SARS-CoV-2 infection, respectively, compared with those of Indonesian nationality.
The regression analysis reveals a surprising finding: individuals with family members who have contracted COVID-19 exhibit significantly lower odds of infection themselves, with statistical significance at the 1% level. In both Model 1 and Model 2, individuals with infected family members demonstrate ∼56.5% and 56.1% lower odds of contracting the virus, respectively, compared with those without infected relatives. These results suggest a potential protective effect associated with having a family member who has contracted COVID-19, prompting further investigation into familial dynamics and their impact on viral transmission and susceptibility.
Vaccinated respondents in Model 1 had a lower likelihood of COVID-19 infection than their unvaccinated counterparts. The impact was significant at the 10% level. Particularly, for individuals who are vaccinated (compared with those who are not vaccinated), the odds of being infected with the SARS-CoV-2 virus are ∼0.519 times or about 48.1% lower (1 − exp−0.656 = 1 − 0.519) than the odds for the group that is not vaccinated. The results obtained from Model 2 affirm the substantial influence of vaccination status on the likelihood of contracting a COVID-19 infection. Specifically, each additional vaccine dose is associated with a notable reduction in the likelihood of infection by ∼0.066 times, equating to roughly 6.6% lower odds of being infected (1 − exp−0.068 = 1 − 0.934). This reduction is statistically significant at the 1% level, implying a robust and meaningful impact of vaccine doses on lowering the risk of COVID-19 infection.
Unexpectedly, individuals with adequate knowledge of the five protective methods displayed a heightened susceptibility to COVID-19 infection, with statistical significance at the 1% level. Specifically, in both Model 1 and Model 2, individuals with sufficient knowledge experienced ∼a 46.9% and 47.9% increase in the odds of contracting the SARS-CoV-2 virus, respectively, compared with those with insufficient knowledge.
Surprisingly, individuals with ample vaccination knowledge showed increased susceptibility to COVID-19 infection, with statistical significance at the 1% level. In both Model 1 and Model 2, individuals with sufficient vaccination knowledge exhibited ∼a 31.1% and 29.4% increase in the odds of SARS-CoV-2 infection, respectively, compared with those with insufficient knowledge.
Discussion
The regression analysis revealed a higher COVID-19 infection risk among males, significant at the 1% level, consistent with Brodin (2021) and Clark et al.’s (2020) findings, highlighting gender’s potential role in virus susceptibility. This may stem from various factors: gender-specific behaviors and roles impacting exposure rates, with men more involved in higher-risk activities and less compliant with preventive measures. Biological differences may also contribute, as males may have distinct immune responses. Furthermore, men’s health care–seeking behavior, often characterized by delayed medical consultation, could result in higher infection rates due to late diagnosis.
The analysis reveals a significant correlation at the 1% level between larger family size and increased SARS-CoV-2 infection risk, consistent with Martin et al. (2020) and Sá (2020). Larger families, with more interpersonal interactions, heighten the chance of in-house virus spread, facilitated by crowded spaces and shared living conditions. The age range within these families, potentially including more high-risk individuals, such as the elderly or those with preexisting health conditions, may exacerbate transmission. Additionally, behavioral factors, such as compliance with preventive measures, and socioeconomic aspects, such as income, health care access, and education, could influence this trend. Lower socioeconomic status and restricted health care access might exacerbate the situation in larger families.
Married or cohabiting individuals demonstrate a significantly lower SARS-CoV-2 infection risk at the 1% level, consistent with Sá’s (2020) findings. This reduced risk may arise from enhanced adherence to COVID-19 preventive measures, driven by shared responsibilities and a collective household safety approach, encompassing social distancing, mask-wearing, and stringent hygiene practices. Emotional and social support from partners or family members may also influence healthier behavioral choices, thereby decreasing exposure risk. Moreover, the living conditions of married or cohabiting individuals, potentially characterized by smaller, less crowded homes, could contribute to this trend, along with a household age composition featuring fewer high-risk elderly members. Socioeconomic factors such as income, health care access, and education level may intersect with marital status, providing better health care resources and knowledge for effective self-protection.
The analysis identifies a significant 1% level association between employment status and a reduced SARS-CoV-2 infection risk, contrary to Baker et al. (2020) and Koh (2020). This warrants further investigation into the underlying reasons. Possible factors contributing to the lower infection risk among employed individuals include workplace safety measures such as mask-wearing, social distancing, and enhanced hygiene practices. Employment often entails exposure to COVID-19 prevention protocols, potentially lowering the virus exposure risk. The nature of one’s occupation, such as remote work possibilities, impacts this relationship; remote work reduces in-person exposure, whereas physical roles in high-risk settings present different risks. Additionally, socioeconomic factors intersect with employment status, potentially granting better health care access, testing affordability, and stronger adherence to public health guidelines to employed individuals.
Urban residents demonstrate a significantly lower SARS-CoV-2 infection risk at the 1% level, consistent with Abedi et al. (2021). This may be attributed to superior urban health care infrastructure, facilitating early diagnosis, treatment, and effective contact tracing. Increased awareness and public health campaigns in urban areas likely bolster adherence to COVID-19 preventive measures, whereas easier access to testing and vaccination centers encourages proactive health behaviors. Urban living often entails smaller household sizes, potentially reducing intrahome virus transmission compared with more crowded rural settings. Socioeconomic factors such as higher income and education levels in urban areas may also contribute, providing resources for prevention and care.
Vietnamese respondents exhibit a significantly lower SARS-CoV-2 infection risk compared with their Indonesian counterparts, significant at the 1% level. This discrepancy may stem from differences in early pandemic response and management, including varying government policies and public health interventions between Vietnam and Indonesia. Sociocultural and behavioral factors, such as adherence to preventive measures, cultural norms, and community compliance with public health guidelines, could also contribute. Differences in health care infrastructure, testing availability, and health care-seeking behaviors might further influence varying infection rates. Additionally, socioeconomic factors such as income, education, and occupation, differing between the two nationalities, could affect access to prevention resources and health care services.
Respondents with infected family members are significantly less likely to contract the virus themselves, a finding supported by Liu et al. (2020) and Nordström et al. (2021) and statistically significant at the 1% level. This reduced infection likelihood may result from stricter preventive measures adopted by individuals with firsthand virus exposure within their families. Experience with an infected family member can strongly motivate adherence to public health guidelines. Household responses, including isolating the infected individual, improved hygiene, and strict social distancing, can mitigate intrafamily transmission. Socioeconomic and demographic factors, such as household size, income, and health care access, may also influence this relationship, differing between families with and without infected members. The association between having infected family members and reduced personal infection risk is multifaceted and influenced by behavioral, socioeconomic, and household dynamics.
The research highlights the significant protective role of COVID-19 vaccination, evident in both vaccination status (1 = vaccinated) and the number of vaccine doses received. These findings are consistent with prior studies by Hall et al. (2022), Nanduri et al. (2021), Pritchard et al. (2021), and Sá (2020), emphasizing vaccination’s effectiveness in reducing COVID-19 transmission and infection rates. This collective evidence emphasizes the critical importance of widespread vaccination efforts in combating the virus’s spread and mitigating its impact on public health. Furthermore, these findings provide valuable insights for policymakers and health care professionals, guiding the development and implementation of effective pandemic control strategies.
The analysis uncovered a counterintuitive result: greater knowledge of the five protective methods correlates with a heightened SARS-CoV-2 infection risk. This unexpected finding suggests that more informed individuals might engage in higher-risk behaviors such as working in hazardous occupations or frequent travel, or they may be more proactive in seeking COVID-19 testing, resulting in a higher diagnosis rate. Additionally, this knowledgeable group likely includes health care workers or individuals residing in densely populated areas. This intricate interplay of knowledge, behavior, and infection risk, which diverges from Xu et al.’s (2020) findings, indicates diverse social, economic, and individual factors influencing this relationship and necessitates further investigation.
The discovery that well-informed respondents about vaccination had a higher COVID-19 infection rate, significant at the 1% level, prompts diverse interpretations. Knowledgeable individuals may engage in riskier behaviors, feel less vulnerable, or belong to high-exposure occupations such as health care. Their likelihood of seeking testing could also influence infection rates compared with others who might underreport. Unconsidered variables like health status might impact this relationship. This correlation, contrasting with Xu et al. (2020), does not imply causation, necessitating further research, including in-depth interviews, to explore the complexities of behaviors and circumstances contributing to this unexpected result.
Conclusions and Research Limitations
This study analyzed data from 5,819 Vietnamese and Indonesian respondents (December 10, 2022–March 27, 2023) using binary logistic regressions to examine COVID-19 infection likelihood. Descriptive statistics revealed a high infection rate among unvaccinated individuals, emphasizing the importance of vaccination status. The analysis showed a dose-dependent protective effect of vaccines, particularly evident across the first four doses, but reversing at the fifth dose. Vaccinated individuals generally experienced faster recovery and milder symptoms, with mRNA vaccines leading to shorter recovery times. Regression results confirmed significant reduction in infection risk due to vaccination. Specifically, vaccinated individuals exhibit ∼48.1% lower odds of SARS-CoV-2 infection compared with the unvaccinated group, a statistically significant effect at the 10% level. Moreover, each additional vaccine dose is linked to a significant reduction in infection likelihood by ∼6.6%. The impact is significant at the 1% level. Gender, family size, marital status, employment, urbanity, and nationality also significantly influenced infection rates. Notably, respondents with infected family members were less likely to contract the virus, potentially due to preventive behaviors in these households. These findings underscore intricate dynamics involving vaccination, demographic variables, and interpersonal connections in shaping COVID-19 infection rates. The study used a web-based survey, possibly introducing bias through self-reporting, which may lead to discrepancies between reported behaviors and actual actions. In addition, certain significant factors may diverge from initial expectations. These limitations should be considered when interpreting the findings and underscore the necessity of employing complementary methods in future research to mitigate these biases.
Footnotes
Acknowledgments
The authors wish to express their profound appreciation to all respondents who participated in our study. Your willingness to share your time and insights was instrumental in the success of our research. We are particularly grateful to Associate Professor Dr. Son Hong Nghiem at the Australian National University for his invaluable expertise and detailed feedback on our R code analysis. His guidance significantly enriched our analytical processes. Heartfelt thanks are extended to the team of dedicated researchers at Griffith University and Thai Nguyen University of Agriculture and Forestry. Your constructive critiques and thoughtful suggestions played a pivotal role in refining our study, greatly enhancing its overall quality and impact. Special acknowledgment is due to Mr. Ihsan Hanif at the Postgraduate School of Universitas Sebelas Maret. His exceptional skills in translating our questionnaires into Indonesian were crucial in bridging cultural gaps and ensuring the inclusivity of our research. His contributions have been indispensable in adding a rich, cross-cultural dimension to our work. Each one of you has left an indelible mark on this study, and for that, we are endlessly grateful.
Authors’ Contributions
A.H.D.: conceptualization, methodology, software, validation, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, visualization, and project administration. G.T.N.: conceptualization, methodology, and investigation. H.T.V.: conceptualization, methodology, and investigation. L.X.D.: conceptualization, methodology, and investigation. H.T.P.: conceptualization, methodology, and investigation. E.A.: conceptualization, methodology, resources, and investigation.
Data and Material Availability
The datasets produced and analyzed in this study are not publicly accessible due to the sensitive nature of the content, including demographic information and personal opinions. However, detailed data, variable codes, and analytical scripts for STATA, SPSS, and R can be obtained from the corresponding author upon a justified request.
Ethical Statement and Consent Procedures
Ethical Approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Ethical Clearance: The research has received ethical clearance from two authoritative bodies. The Department of Preventive Medicine, Vietnamese Ministry of Health, granted approval (reference number 250/QĐ-ĐĐNC/YTDP/2022, Protocol/ID: 250/06/22), and the Faculty of Medicine at Universitas Sebelas Maret, Indonesia, also endorsed the study (reference number 09/UN27.06.11/KEP/EC/2023, Protocol/ID: 01/02/12/2022/186).
Informed Consent: Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.