
Abstract
BK virus is a childhood virus that can reactivate in immunocompromised individuals, particularly organ transplant recipients, causing transplant rejection due to BK virus-associated nephropathy. The study aimed to assess the prevalence of BK virus infection in kidney transplant recipients, examine the relationship between demographic and laboratory factors and active infection, evaluate the impact of reducing immunosuppressive drug doses on BK virus reactivation, and explore the genotyping of BK virus strains in this population. This cross-sectional study utilized 245 serum samples from kidney transplant recipients. Viral DNA was extracted from these samples, and initially, Nested PCR was employed for screening to ensure accuracy, with primers targeting a segment of the VP1 gene used to detect the BK virus genome. Real-Time PCR was subsequently performed on positive samples to measure viral load more precisely. The prevalence of BK virus infection among kidney transplant recipients was 5.3%. Out of 245 kidney transplant recipients, 13 individuals were diagnosed with active BK virus infection. Genotype I was the most prevalent, accounting for 90% of the cases. The relationship between demographic factors (gender and age) and laboratory parameters (fasting blood glucose, creatinine, hemoglobin, and platelet count) was examined in both kidney transplant recipients with and without active BK virus infection. The results revealed that a reduction in immunosuppressive drug dosages, particularly tacrolimus, was associated with a decrease in BK viral load, potentially contributing to a lower incidence of active BK virus infections. Additionally, hematological analysis showed a significant decrease in hemoglobin levels in kidney transplant recipients with active BK virus infection, accompanied by a significant increase in serum creatinine levels. Balancing immunosuppressive therapy, especially reducing tacrolimus, helps control BK virus reactivation and preserve graft function. Regular monitoring of hematological parameters and viral load is crucial for optimal management in kidney transplant recipients.
Introduction
BK polyomavirus (BKPyV) is a non-enveloped, small, icosahedral, double-stranded DNA virus and a member of the Polyomaviridae family (Demey et al., 2018). The BK virus (BKV) genome encodes three capsid structural proteins—VP1, VP2, and VP3—as well as the Agno protein from the late region, and the large T and small t antigens from the early region. Infections with BKV often occur during childhood; however, individuals with a healthy immune system typically remain asymptomatic and do not experience serious clinical outcomes. Approximately 90% of adults are seropositive for BKPyV. When the immune system is compromised, such as through the use of immunosuppressive drugs, BKV can reactivate and begin shedding in the urine. Reactivation of BKV infection poses a significant issue for kidney transplant recipients (KTRs) (Gonzalez et al., 2015; Kant et al., 2022), as it can lead to BK polyomavirus-associated nephropathy (BKPyVAN). This nephropathy impairs graft function and results in early graft rejection in 1–10% of KTRs (Kant et al., 2022).
Since the discovery of BKV in 1971, no effective prophylaxis or treatment has been developed, and the infection continues to contribute to allograft loss. Consequently, blood and urine screening for KTRs has become a major recommendation. Reduced immunosuppression is currently the only proven method to mitigate the outcomes of this infection (Demey et al., 2018; Myint et al., 2022).
In clinical practice, plasma BKV load has become the primary marker for diagnosing and managing BKV infection in KTRs, as it allows for early detection and preventive interventions, including the reduction of immunosuppression. In contrast, BKV-associated nephropathy (BKVAN) is a histological diagnosis confirmed by an invasive kidney biopsy (Faguer et al., 2007; Hirsch et al., 2005). Recent recommendations emphasize that allograft biopsy should only be performed in cases of acute kidney injury (AKI) with suspected BKV infection. Interventions, such as reducing immunosuppression, should be initiated based on a presumptive diagnosis from BKV plasma load, rather than waiting for graft dysfunction (Bohl and Brennan, 2007; Myint et al., 2022). This approach is crucial in preventing the irreversible damage caused by BKVAN, which may be detected too late if one only waits for a decline in renal function (Faguer et al., 2007).
Studies have shown that identifying BKV genotypes is crucial for the diagnosis and management of BKPyVAN (Pastrana et al., 2013; Sato et al., 2024). Phylogenetic analyses based on VP1 fragment variations show that genotypes I and IV are predominant, while genotypes II and III are rare (5%) (Sawinski and Goral, 2015).
The primary objective of this study was to investigate the prevalence and genotypic distribution of BKV in KTRs, as well as to assess the relationship between BKV infection and clinical parameters, such as serum creatinine and hemoglobin levels. Furthermore, the study aimed to explore the implications of BKV plasma load monitoring for the early diagnosis and management of BKVAN in KTRs, emphasizing the importance of early intervention through reduced immunosuppression to prevent graft dysfunction.
Methods
Study population
In this cross-sectional study, 245 serum samples from KTRs (3 months post-transplantation), who were transplanted at one of three medical centers in Tehran between 2018 and 2019, were analyzed. The study received approval from the ethics committee of Tehran University of Medical Sciences.
The inclusion criteria for the study were adult KTRs (aged 18 years or older) who provided informed consent and had a stable post-transplant follow-up period. The exclusion criteria involved patients with active HHV-8 or CMV infections, a history of prior BKV infection (to avoid confounding the analysis of BKV reactivation and BKVAN), those who had received transplants of organs other than kidneys, and those who had been on pre-transplant dialysis for more than 6 months.
Among 312 KTRs initially screened between 2018 and 2019, a total of 67 patients were excluded due to not meeting the eligibility criteria: 18 had active CMV or HHV-8 infection, 12 had a documented history of prior BKV infection, 20 had received non-renal organ transplants, and 17 had undergone pre-transplant dialysis for more than 6 months. The remaining 245 eligible recipients, who fulfilled all inclusion and exclusion criteria and provided informed consent, were consecutively enrolled and included in the final analysis (Fig. 1).
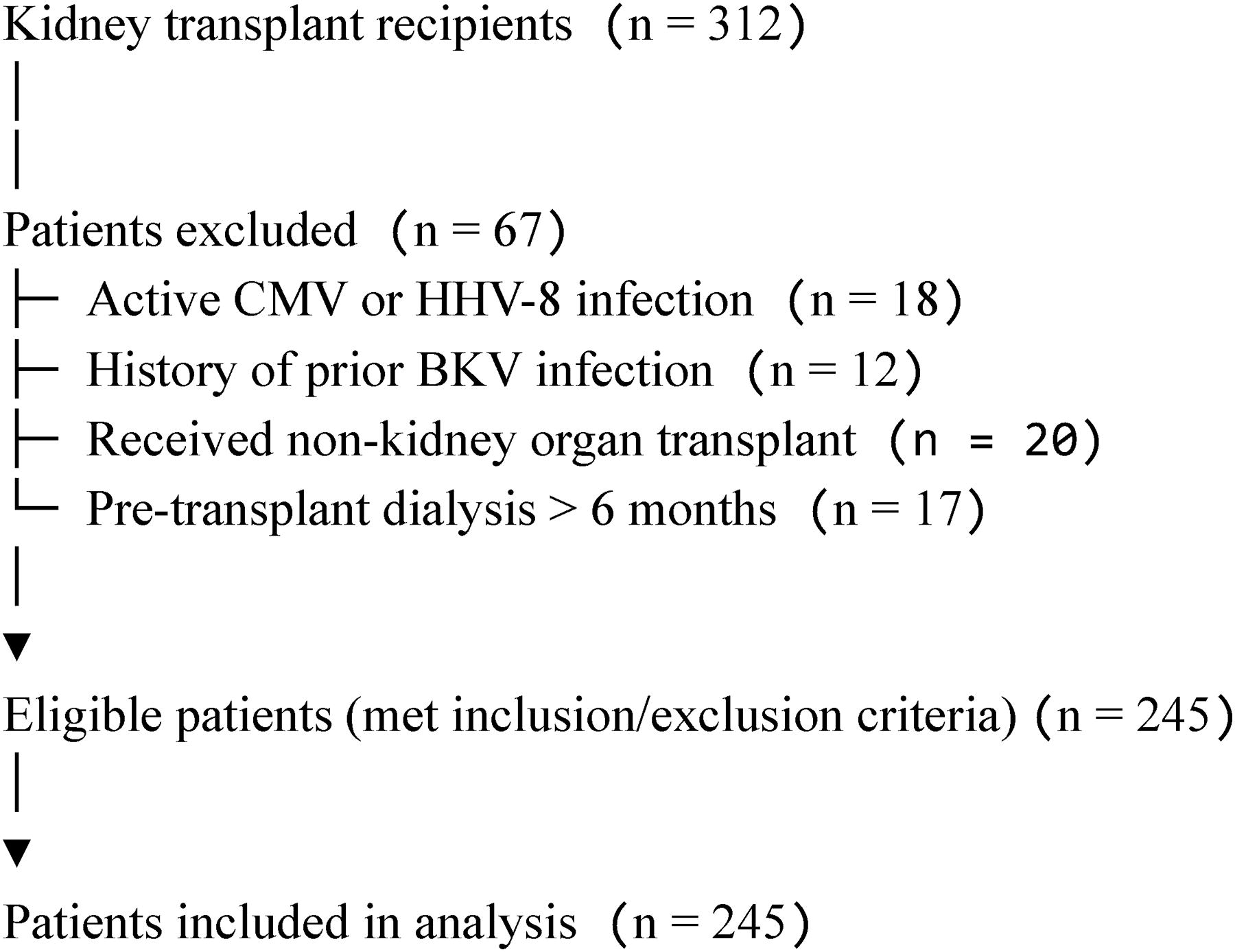
Patient flow diagram.
To minimize confounding, patients with unstable allograft function during the first 3 months post-transplant were excluded, as early graft dysfunction may result from multiple causes other than BKV. Similarly, patients with pre-transplant dialysis duration exceeding 6 months were excluded due to their higher baseline risk for chronic graft pathology. These criteria aimed to ensure a homogenous cohort for accurate assessment of BKV prevalence among stable KTRs.
Diagnostic methods
BKV detection
Plasma samples were first tested for BKV DNA using a nested PCR technique. A total of 245 samples were initially screened using this method. The nested PCR technique is a two-step amplification method, which significantly enhances the sensitivity and specificity of BKV detection, providing a high degree of accuracy even in cases of low viral load (VL).
Viral DNA was extracted from 200 μL of serum using a high-purity viral nucleic acid kit (Roche, Germany) according to the manufacturer’s instructions. Nested PCR was performed to amplify a VP1 fragment. In the first step, external primers (BKV-ext1; 5′-AAGATGGCCCCAACCAAA-3′ and BKV-ext2; 5′-GCATTTCCAAGGGGTCTTC-3′) as shown by Boukoum et al. (2011) in the past, were used to amplify nucleotides 1561–2051 of the VP1 fragment of the BKV genome, with an expected product length of 490 bp. In the subsequent step, internal primers (327-1; 5′-CAAGTGCCAAAACTACTAAT-3′ and 327-2; 5′-TGCATGAAGGTTAAGCATGC-3′) amplified nucleotides 1630–1956 of the VP1 fragment, yielding a 335 bp product (Boukoum et al., 2011). The second fragment was then electrophoresed using a 100-bp DNA ladder (Sinaclon, Iran).
DNA sequencing assay
BKV-positive PCR products were purified using a BigDye sequencing kit, and sequencing was performed directly at Tehran University of Medical Sciences. BKV genotype sequences from this study were deposited under accession numbers MZ386649–MZ386658 at http://www.ncbi.nlm.nih.gov. Reference sequences for alignment were obtained from the same database. A phylogenetic tree was constructed using the maximum-likelihood method, tested with the Bootstrap resampling strategy (1,000 replicates), and analyzed using MEGA X software.
Follow-up of positive cases
After the initial nested PCR, real-time PCR was performed on all positive samples. This step was implemented to monitor VL more precisely and assist nephrologists in follow-up management. By performing real-time PCR on the positive samples, nephrologists were able to facilitate timely interventions, such as adjusting immunosuppression, to prevent BKVAN and avoid graft dysfunction. The addition of real-time PCR improved the clinical decision-making process and made it easier for nephrologists to follow up with patients.
The BKV titer was measured from DNA extracted from plasma samples of KTRs with active BKV infection. The analysis was conducted using the GeneProof BKV PCR Kit and the ABI StepOne Plus Real-Time PCR system, following the manufacturer’s instructions. The mastermix and extracted viral DNA were combined with standard samples and loaded into the device. Thermal cycling conditions and channel settings were adjusted according to the kit’s protocol.
Additionally, for co-infection monitoring, all patients were screened for HHV-8 and CMV DNA using PCR to rule out co-infections that might affect renal function and influence the course of BKV reactivation.
In accordance with current transplant guidelines, management of presumptive BKVAN was based on plasma VL trends rather than histological confirmation. The decision not to perform biopsies was protocol-driven and focused on preemptive management via non-invasive monitoring to reduce allograft injury risk.
Immunosuppression protocol
All KTRs received a standardized immunosuppression regimen to minimize rejection while controlling the risk of BKV reactivation. The protocol included:
Immunosuppressive therapy was adjusted based on clinical and virological markers, including BKV VL. This consistent approach across all patients helped minimize BKV infection and BKVAN.
Immunosuppressive therapy was tailored based on VL and patient response. Tacrolimus trough levels were maintained in the range of 4–7 ng/mL in patients with detectable BKV, compared with 7–10 ng/mL in patients without viremia. MMF was administered at 1–2 g/day, and corticosteroids were tapered to 5 mg/day or discontinued after 3–6 months in stable patients. These dose adjustments were implemented as part of a preemptive strategy in patients with rising BKV loads to mitigate progression to BKVAN.
Statistical analyses
Data were analyzed using GraphPad Prism 9.0.0 statistical software (GraphPad Software, San Diego, CA). To compare quantitative variables, the Mann-Whitney U test or Student’s t-test was applied as appropriate. A p-value of less than 0.05 was considered indicative of statistical significance.
Results
A total of 245 KTRs were enrolled in this cross-sectional study, with a mean age of 37.9 years (ranging from 20 to 78 years). Among the participants, 56.7% were male and 43.3% were female. The demographic and clinical characteristics of the KTRs in this study are summarized in Tables 1 and 2.
Demographic Information, Including Age Groups and Sex, of Kidney Transplant Recipients
Clinical Data, Including Creatinine, Hemoglobin, Fasting Blood Sugar, and Platelet Levels, in Kidney Transplant Recipients
BKV DNA was detected in 13 out of 245 patients, indicating a prevalence of 5.3%. There was no statistically significant association between BKV viremia and sex in KTRs (p-value = 0.666, Mann-Whitney test) (Table 3). Additionally, no significant association was found between BKV infection and age groups (p-value = 0.420, Mann-Whitney test) (Table 4). However, serum creatinine levels were significantly higher in KTR with active BKV infection (p-value = 0.0001, Mann-Whitney test) (Fig. 2).
Determining the Frequency of BK Virus Based on Gender in Kidney Transplant Recipients
BKV, BK virus.
Determining the Frequency of BK Virus Based on Age Groups in Kidney Transplant Recipients
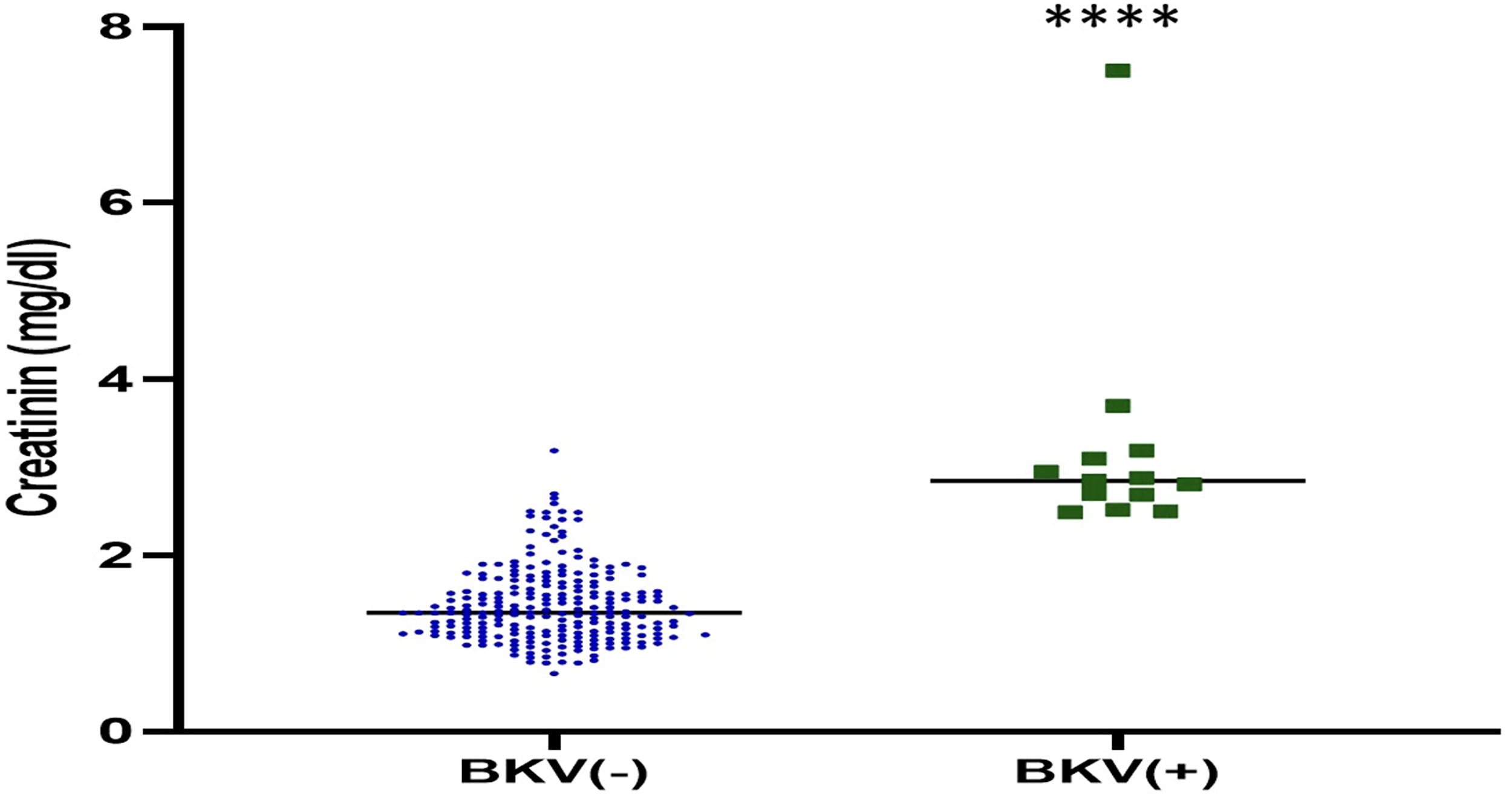
A comparison of creatinine levels between two groups of transplant recipients, those with active BKV and those without BKV. ****p < 0.0001. BKV, BK virus.
Sequencing was performed on 10 out of the 13 positive samples using MEGA software. Phylogenetic analysis revealed that genotype I was the most prevalent among the KTRs in this study, accounting for 9 out of 10 strains, followed by genotype IV (1 out of 10). Genotypes II and III were not detected in this study population (Fig. 3).

Phylogenetic tree of BK polyomavirus base on VP1 gene, which uses the maximum likelihood method based on Kimura’s 2-parameter model and made in Mega X. The sequences in this study are indicated by blue and red circles.
Real-time PCR was utilized to quantify the VL in these 13 KTRs with active BKV infection. The VL data, along with other clinical information such as medical history, type of transplant, and transplant history, are presented in Table 5.
Demographic and Clinical Characteristics of Kidney Transplant Recipients with Active BK Virus Infections
Further analysis was conducted to investigate the relationship between BKV infection and other clinical variables, including hemoglobin, fasting blood sugar (FBS), and platelets. A significant decrease in hemoglobin levels was observed in KTRs with active BKV infection compared with those without active BKV infection (p-value = 0.013, Mann-Whitney test) (Fig. 4). However, no significant association was found between BKV infection and FBS (p-value = 0.927, Mann-Whitney test) (Fig. 5) or platelets (p-value = 0.15, Mann-Whitney test) (Fig. 6).

A comparison of hemoglobin levels between two groups of transplant recipients, those with active BKV and those without BKV. *p < 0.05.
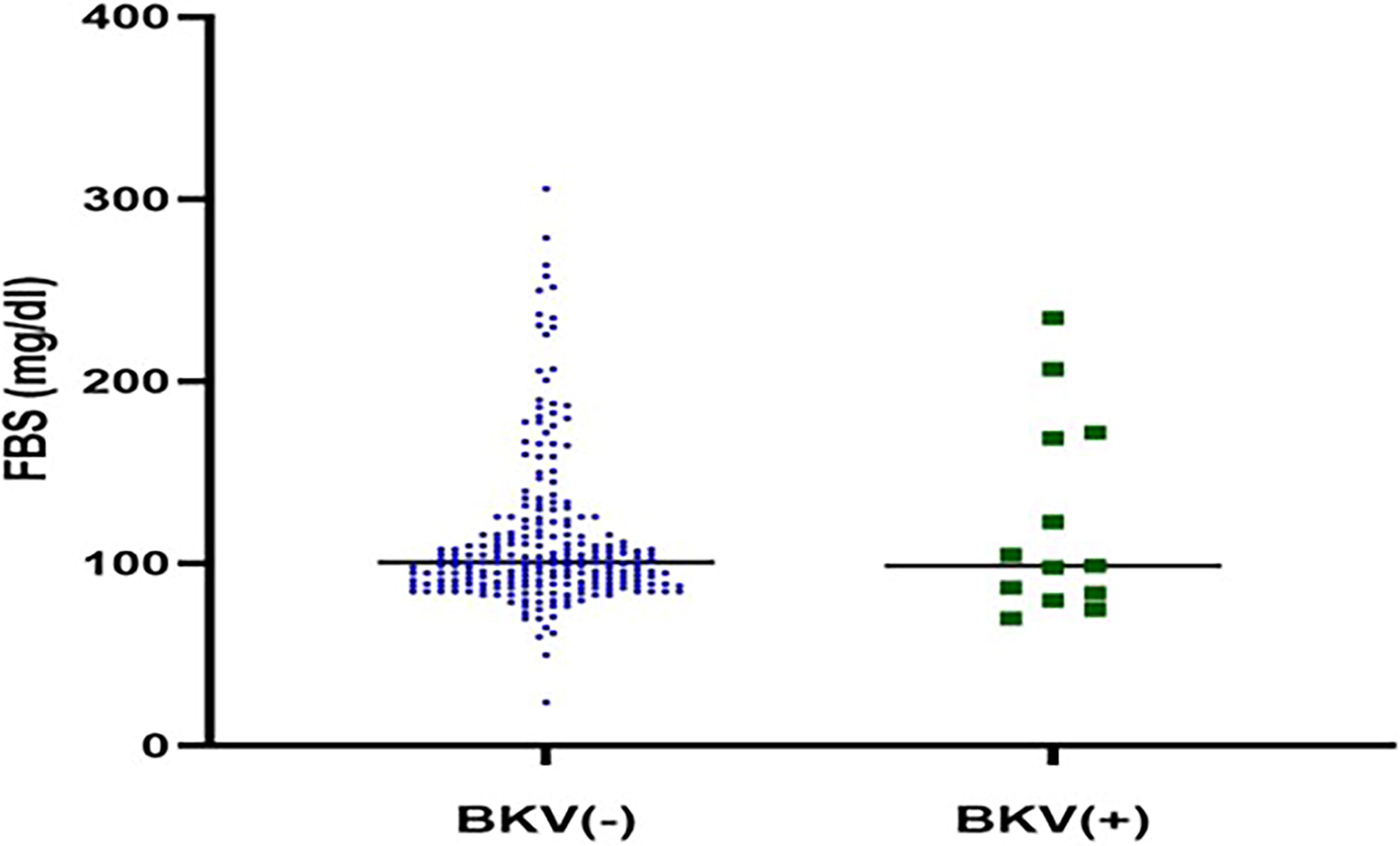
Comparison of FBS levels between two groups of transplant recipients, those with active BKV and those without BKV. FBS, fasting blood sugar.
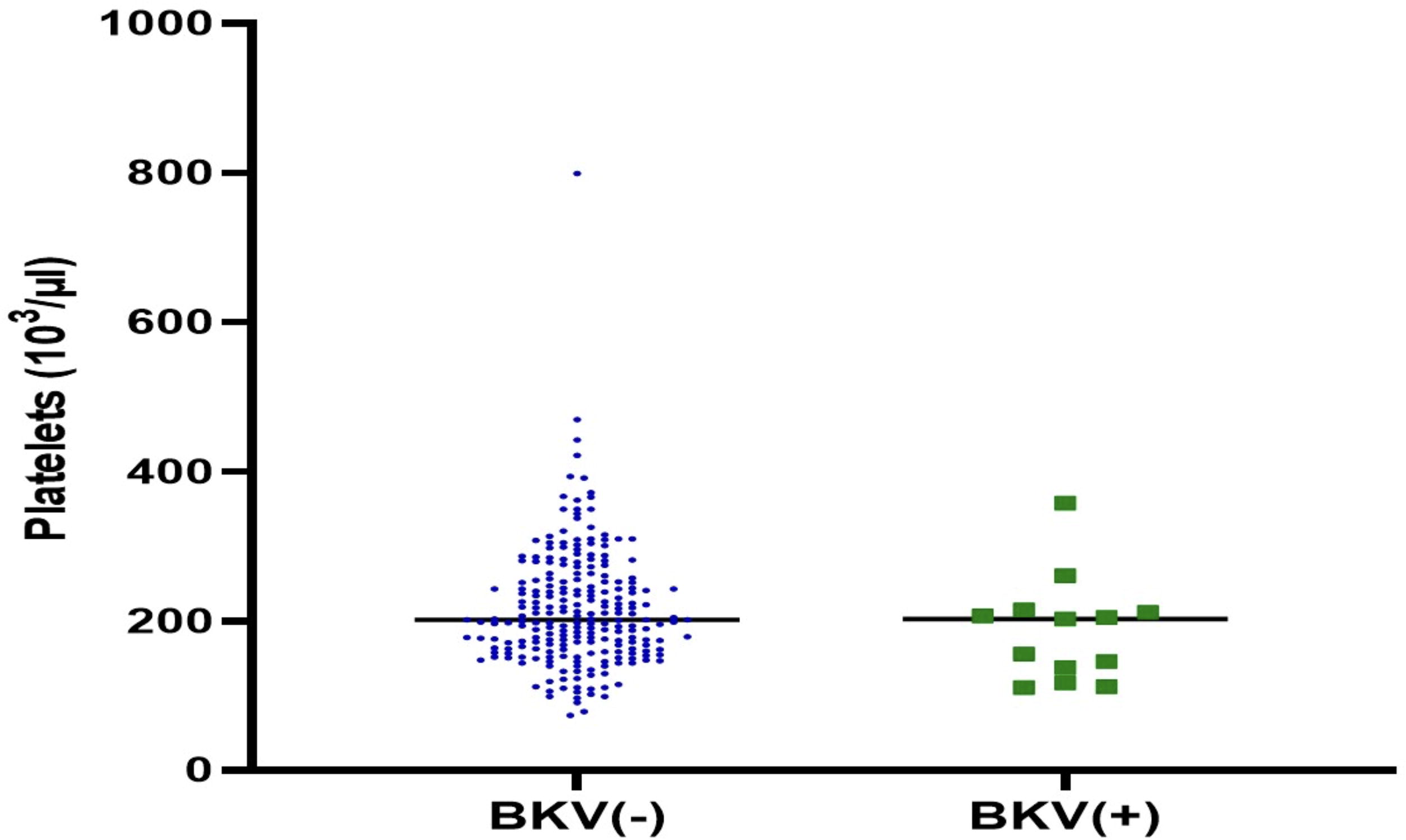
Comparison of platelets levels between two groups of transplant recipients, those with active BKV and those without BKV.
Discussion
In this cross-sectional study, we assessed the prevalence and molecular characterization of BKV in KTRs. BKV infection was found in 13 out of 245 KTRs, resulting in a prevalence of 5.3%. Genotype I was the most prevalent (90%), followed by genotype IV (10%). BKV infection is a major concern after kidney transplantation, as it is a leading cause of BKVAN, which leads to kidney dysfunction in over 60% of patients and can cause graft loss. The incidence of BKVAN ranges from 1% to 10% and is linked to immunosuppressive therapy (Blazquez-Navarro et al., 2018; Hirsch et al., 2005). Early diagnosis is critical, but BKVAN is often detected through elevated serum creatinine levels or biopsy. BKV serum loads up to 10,000 copies are considered indicative of presumptive BKVAN (Egli et al., 2007; Weikert and Blumberg, 2008).
In our study, BKV infection was detected in 5.3% of KTR using nested PCR from serum samples, which is comparable to rates reported by Pourkazemi et al. in Iran (7.3%) (Pourkazemi et al., 2020), Wisconsin, USA (4%) (Vasudev et al., 2005), France (3.6%) (Gras et al., 2023), and Brazil (6.4%) (Pires et al., 2011). This may be linked to reduced immunosuppression in the KTRs in this study. Immunosuppression protocols vary, with lower doses of tacrolimus used in our study (Szumilas et al., 2023). BKVAN symptoms overlap with those of transplant rejection and are differentiated through clinical and morphological assessments. BKVAN is managed by reducing immunosuppression, while preventing transplant rejection requires increasing it. Balancing immunosuppression is crucial to minimize BKV reactivation and prevent transplant rejection, as imbalances in the immune system can harm kidney transplant function (Bohl and Brennan, 2007; Pezeshgi et al., 2012; Shen et al., 2021).
Our study found a lower prevalence of BKV infection in KTRs compared with several other studies. For instance, Cobos et al. (2018) reported a 36.36% BKV infection rate in KTR in Argentina (Cobos et al., 2018), Kaydani et al. (2015) observed a 41.8% rate in Ahvaz, Iran (Kaydani et al., 2015), and Drachenberg et al. (2007) documented a 56.3% infection rate in Maryland, USA (Drachenberg et al., 2007). Managing BKV in KTRs requires a careful balance of immunosuppressive therapy to prevent graft rejection while reducing viral infections. In our study, reducing tacrolimus dosage, along with other immunosuppressants such as MMF and corticosteroids, contributed to a decrease in BKV incidence. Excessive immunosuppression increases the risk of viral reactivation, while insufficient suppression raises the risk of graft rejection. Our findings suggest that reduced immunosuppression played a key role in the lower BKV incidence observed.
In our study, genotype I was the most prevalent among KTRs, consistent with previous global findings. However, the distribution of BKV genotypes varies by region, and certain genotypes, such as genotype IV, may exhibit distinct pathogenic characteristics. While genotype I is commonly associated with BKVAN, genotype IV has been linked to more severe BKVAN in Asian populations, whereas genotype I is more common in Europe and North America (Zhong et al., 2009).
Genotypes II and III, though rare, exhibit differences in replication dynamics and their potential to cause graft dysfunction. Genotype II is less virulent than genotype I, and data on the clinical significance of genotype III remain limited. These variations highlight the importance of genotype-specific surveillance and treatment strategies. Understanding genotype-related differences is crucial for managing BKV infection and BKVAN, as they can influence VL thresholds, immune responses, and graft function, particularly in cases of inappropriate immunosuppression (Cobos et al., 2018; Schwarz et al., 2016). Therefore, precise monitoring of BKV genotypes is essential for refining therapeutic strategies and improving patient outcomes, particularly by optimizing antiviral therapies and maintaining appropriate immunosuppression to prevent graft rejection.
Regarding demographic factors, our study found no significant differences in BKV infection rates across age groups or genders. This finding is consistent with studies by Schwarz et al. (Germany) (Schwarz et al., 2016), Kaneko et al. (Japan) (Kaneko et al., 2005), and Dolei et al. (Italy) (Dolei et al., 2000), which also found age and gender not to be significant risk factors for BKV infection. However, some studies, including Pourkazemi et al. (Iran) (Pourkazemi et al., 2020) and Nampoory et al. (Kuwait) (Nampoory et al., 2005), suggest that demographic factors such as age and male gender might increase the risk of BKV viremia, potentially due to age-related immune system decline.
Elevated serum creatinine levels are a key indicator of kidney dysfunction and are commonly linked to BKV infection. An increase in creatinine of more than 25% from baseline, along with a BKV VL exceeding 104 copies/mL for over 3 weeks, suggests BKVAN. This observation is supported by studies by Schub et al. (Switzerland) (Schaub et al., 2010), Faguer et al. (France) (Faguer et al., 2007), Tremolada et al. (USA) (Tremolada et al., 2010), and Drachenberg et al. (USA) (Drachenberg et al., 2007), which confirm the association between increased serum creatinine levels and BKV infection.
Our study revealed that KTRs with active BKV infection had significantly lower hemoglobin levels compared with those without BKV infection. This reduction in hemoglobin may be attributed to several factors. First, BKV can interfere with bone marrow function, impairing red blood cell production, particularly in immunocompromised individuals (Sharma and Bajwa, 2020b). Second, immunosuppressive drugs, particularly calcineurin inhibitors like tacrolimus, may exacerbate this decline by directly damaging bone marrow erythroid precursors and contributing to anemia of chronic disease. Other immunosuppressants, such as MMF and corticosteroids, can also suppress hematopoiesis, further reducing hemoglobin levels (Sobiak et al., 2013; Yang et al., 2015). Additionally, reactivation of latent viruses such as CMV and EBV can cause bone marrow suppression and worsen anemia, compounding the effects of BKV infection (de Melo Silva et al., 2020; Sharma and Bajwa, 2020a). Studies by He et al. (China) (He et al., 2023), Faguer et al. (France) (Faguer et al., 2007), and our study indicate a significant decrease in hemoglobin levels in KTR with BKV infection compared with those without.
Our study also indicated that no significant differences were observed in FBS levels between KTR with and without active BKV infection. Factors such as variations in immunosuppressive regimens, including lower doses of tacrolimus in our study, could explain this result, as certain immunosuppressive drugs, including corticosteroids and calcineurin inhibitors (such as tacrolimus and cyclosporine), can affect glucose metabolism. Pre-existing diabetes, the duration of immunosuppressive therapy, and comorbidities may also contribute to the variability in FBS levels (Åsberg et al., 2009; Chakkera et al., 2017).
Finally, our study assessed platelet levels in KTR with and without active BKV infection and found no significant differences. This finding is consistent with studies by Wang et al. (China) (Wang et al., 2022) and Errad et al. (USA) (Erard et al., 2004). However, other studies, such as those by Kuten et al. (USA) (Kuten et al., 2014) and Faguer et al. (France) (Faguer et al., 2007), report significant decreases in platelet levels associated with antiviral drugs like Cidofovir and Leflunomide. The absence of a clear association between platelet count and BKV infection may be due to the balanced immunosuppressive regimen used in our study, which reduced the doses of tacrolimus, MMF, and steroids. This approach may have minimized hematological side effects typically seen with more aggressive immunosuppressive therapies. While some studies report a decrease in platelet count due to antiviral therapy or viral reactivations, our findings suggest that platelet count alone is not a reliable marker for BKV infection or monitoring BKVAN. This emphasizes the need for comprehensive diagnostic approaches that include VL monitoring, histopathology, and clinical evaluation (Teachey et al., 2009; Zhang et al., 2022).
This study has limitations, including: (1) a small sample size (245 KTRs), limiting generalizability; (2) being a cross-sectional study, which shows associations rather than causality, necessitating future longitudinal research; (3) data access constraints that hindered a detailed analysis of immunosuppressive regimens and transplant outcomes; and (4) the study’s geographical focus, which may not fully represent global BKV prevalence and genotypic variation.
Furthermore, due to data access limitations, detailed clinical and demographic information for some patients was unavailable, which could have provided a more comprehensive analysis of the relationship between these characteristics and BKV infection. Additionally, kidney biopsies were not performed in this study. This decision was based on our clinical protocol, where the diagnosis and management of BKV infection were primarily guided by plasma VL (measured by PCR) and clinical parameters. According to current guidelines, kidney biopsy is generally reserved for cases with AKI and suspected BKV infection. In our study, management decisions were made based on VL results and adjustments to immunosuppressive therapy to prevent further graft damage, thus obviating the need for biopsy in these cases.
Although a direct statistical correlation between immunosuppressive drug levels and BKV VL was not calculated due to study design limitations, a clinical trend was observed wherein patients with reduced tacrolimus exposure (4–7 ng/mL) exhibited lower VLs compared with those with higher levels. This observation supports existing literature suggesting that viral reactivation is closely linked to immunosuppressive burden. Future prospective studies with drug level monitoring and longitudinal data collection are warranted to further elucidate this relationship.
Conclusion
This study demonstrated a 5.3% prevalence of BKV infection among KTRs, with genotype I being the most predominant. Significant associations were observed between BKV infection and both elevated serum creatinine and reduced hemoglobin levels. Furthermore, a reduction in immunosuppressive therapy, particularly tacrolimus, correlated with lower VLs. These findings suggest that individualized immunosuppressive management and regular VL monitoring are essential for the early detection and control of BKV infection, fully consistent with the study’s predefined aims.
Footnotes
Acknowledgments
The authors are grateful to all the dear patients who patiently participated in this study and also to all those who were with the authors.
Authors’ Contributions
F.R. designed and directed the project. M.G. collected samples and carried out experimental data and wrote the article. M.G. and N.P. performed the analysis. N.P., T.M.-A., M.K., and N.Z.S.-J. helped in preparing the final draft.
Ethics Approval and Consent to Participate
This protocol study was reviewed and approved by the ethics committee of Tehran University of Medical Sciences, and then it was done with the informed consent of all patients participating in this study before the start of sample collection (ethic code number: IR.TUMS.SPH.REC.1399.3897). The study was carried out in compliance with the principles outlined in the Declaration of Helsinki.
Author Disclosure Statement
The authors declared that there was no conflict of interest between authors or between authors and institutions. M.G., N.P., T.M.-A., N.Z.S.-J., and F.R. are from Tehran University of Medical Sciences (Tehran, Iran), and M.K. is from Bushehr University of Medical Sciences (Bushehr, Iran).
Funding Information
This study is a master’s thesis in medical virology that was supported by the Tehran University of Medical Sciences (Grant number: 32875).