
Abstract
Abstract
Women with a history of sexual violence may face obstacles to obtaining preventive health services. Group education models have been used in other settings to improve knowledge and uptake of care. Focus groups were conducted to solicit the concerns and input of the subject population. Interdisciplinary group education sessions (GESs) were designed specifically to address concerns voiced in focus groups. GESs were conducted, addressing mammograms, pelvic examinations, and menopause, and emphasized preventive health education, as well as shared decision-making. GESs were audio recorded and qualitative feedback was collected immediately after each GES. Surveys were administered before and after each GES to evaluate attitude and knowledge change. A total of 18 women attended the focus groups, and 27 women attended at least one GES, with 12 women attending both. GESs were well received, and participants cited the education, group support, and healing dynamic as benefits of participation. Content knowledge improved after all three GESs. Attitude change showed a trend toward improvement, but the sample size was not large enough to detect statistical significance. Group education is an acceptable and feasible model among survivors of sexual violence. GESs improved knowledge among this small group of participants. GESs could be made available in a wide range of topics, as requested by our participants. Larger studies are warranted to examine long-term knowledge and attitude change after GESs.
Introduction
W
A female-only group setting can be a supportive low-stress environment to both gain knowledge and discuss concerns in a nonthreatening context (Grella et al. 1999; Kimerling et al. 2015). Group prenatal care (GPC) is a similar model, in which prenatal care is administered to a group of women as a 90–120-minute educational session, with clinical care administered during the educational visit (Reid 2007). GPC participants gain group support and knowledge from each other (Heberlein et al. 2016; Kennedy et al. 2009). GPC has been found to be effective in achieving different pregnancy outcomes, including improvements in gestational diabetes screening and management, and pregnancy and postpartum weight management (Magriples et al. 2015; Mazzoni et al. 2016). GPC also has a positive impact on psychosocial outcomes for high-stress women during pregnancy and postpartum (Ickovics et al. 2011). In addition, GPC offers camaraderie, community, and improved education (Heberlein et al. 2016) and also increases understanding of medical information and improved self-advocacy (Liu et al. 2017). In addition, GPC for military women helped women feel less alone, but they still voiced a need for more privacy and individual time with the provider (Kennedy et al. 2009). Shared medical visits (SMVs) in primary care have shown improvement in several health outcomes (Geller et al. 2015; Housden et al. 2013; Jaber et al. 2006a, 2006b; Khan et al. 2015; Sabatino et al. 2012). The SMV combines elements of healthcare, such as vital signs, history taking, and physical examination, with educational or discussion formats (Jaber et al. 2006a). SMVs have been shown to improve outcomes in a wide range of conditions, including diabetes, heart disease, and pediatric obesity (Geller et al. 2015; Housden et al. 2013; Yehle et al. 2009).
The purpose of this pilot study was to design and evaluate group education sessions (GESs) for preventive health interventions for women with prior sexual violence. We explored the barriers and needs of the population in a sensitive and nuanced manner and designed the GESs according to qualitative feedback solicited in focus groups.
Materials and Methods
Ethical approval and subject recruitment
This study was approved by the institutional review board of the New York Harbor Healthcare System of the Department of Veterans Affairs. Potential subjects were included if they (1) identified as having an unwanted sexual experience (including military or nonmilitary sexual trauma) in their lifetime; (2) were female veterans enrolled within the VHA; and (3) spoke English. Participants were excluded if they were unwilling or unable to provide informed consent. Subjects were counseled that the focus groups and GESs would not address their specific history of trauma to avoid emotional distress.
Recruitment
We recruited participants for the focus groups and GESs from the Department of Veterans Affairs New York Harbor Healthcare System, which includes both the Manhattan and Brooklyn campuses. Recruitment efforts included the following: flyers at the VA, requests that providers and staff refer patients, discussions about the study with potential participants at a VA Women's Health Day event and at the weekly women veterans-only clubhouse, and snowball sampling (Krueger and Casey 2009). We offered a $10 gift card and a $5 metro card for participation in each session.
Focus groups
Focus groups were conducted to better understand barriers to care faced by women veterans at the VA and how the GESs can help overcome these barriers. Women were eligible to participate in one of two focus groups and any or all GESs.
The focus group guide incorporated open-ended semistructured questions about pelvic examinations, mammograms, and birth control (Supplementary Appendix A; Supplementary Data are available online at www.liebertpub.com/vio). Focus groups were led by an experienced facilitator; two additional research team members observed the groups.
Focus group analysis
Focus groups were audio recorded, transcribed verbatim by a third-party vendor, reviewed for accuracy, and read and reread to identify emerging themes. An initial consensus codebook was created following independent review of a subset of transcripts. Transcripts were analyzed using Applied Thematic Analysis, an inductive approach designed to identify and examine emerging themes from conceptual data (Guest et al. 2012). Each transcript was independently coded, the codebook was modified as new themes emerged, and researchers met to discuss and reconcile discrepancies for each transcript until a final coded transcript was agreed upon. Themes from focus groups were organized and analyzed using descriptive matrix analyses wherein the range of responses related to each theme was visually displayed and codes were condensed into discrete themes (Averill 2002). Nvivo qualitative software, v.8, (NVivo, 2009) was used for data management and retrieval.
Group education sessions
We used focus group findings to design the GES. Interdisciplinary GESs were conducted between August and September 2015 and taught collaboratively by both a gynecologist and a psychologist. The goals of the GES were to (1) provide information, (2) spark discussion, (3) encourage shared decision-making, and (4) empower the women in their healthcare experiences. GESs were created using PowerPoint. The scientific content (e.g., the biological process of menopause) was written in conversational language, and this was reviewed and agreed upon by the study team. The GES emphasized shared decision-making as well as how to handle conflict or difficult situations with a healthcare provider and how to address issues of avoidance of preventive healthcare. Subjects were encouraged to ask questions and to offer their own experiences and opinions. We collected demographic information before each GES. We administered knowledge and subjective preference pre- and post-tests immediately before and after the GES. Subjective preference surveys (Supplementary Appendix B) contained 7–10 questions to elicit the participants' opinions regarding the preventive health topic. Knowledge tests (Supplementary Appendix C) contained six to seven questions assessing the participants' understanding of facts regarding the preventive health activity, commensurate with expected patient-level knowledge. Before initiating each session, we obtained informed consent for participation and for audio recording.
Analysis
GESs were analyzed using the same methods as the focus groups. Seven additional codes were added to the codebook created for the focus groups with a total of 41 codes. There were 699 passages coded across five transcripts. Codes were used on average 17.6 times (range 4–63). Pre- and post-tests from the GESs were analyzed using Stata, v.13.
To increase the validity of the collected and analyzed data, we conducted two external reviews. First, we used member checking, and in October 2015, we invited all participants back to present the focus group findings to ensure they reflected their opinions and beliefs (Guest et al. 2012). Additionally, in October 2015, we presented our findings to VA researchers and clinicians not involved in either data collection or analysis to examine the rigor of the analytic process and probe for potential biases.
Results
Participant demographics
In June 2015, 18 women participated in two focus groups, with nine participants in each group. Between August and September 2015, 27 women participated in the GESs; participation ranged from 9 to 14 women in each session.
Demographics of the focus groups and the three GES participant groups are displayed in Table 1. The mean age of participants in the three groups was similar, with the pelvic examination group at 54.0 years (range 35–63), mammogram group at 51.6 years (range 32–64), and menopause group at 56.3 years (range 41–68). The participants were predominantly single, African American, and most had attended or graduated from college. Almost none were employed. Most self-rated their health as fair or good, with few describing it as very good or excellent.
In the mammogram group, one participant did not fill out a demographic questionnaire, but completed the other assessments. In the menopause group, one participant did not fill out any of the questionnaires/surveys.
GED, General Education Diploma.
Focus groups
Focus groups took an average of 65 min (range 64–66). Many women reported lacking basic information about reproductive health, such as the reason behind specific examinations (e.g., a Pap smear or pelvic examination), how their bodies change over time (e.g., menopause), and expressed a desire for more basic education on women's reproductive health. Quotations and themes from the focus groups that influenced the GES design can be seen in Table 2. Themes include agency, individual empowerment versus systematic change, self-care and triggers, and requests for additional peer support or advocacy.
Agency touched on both military service and perceptions of the medical establishment. Examples include not having control over birth control choices while in the military (Table 2, Comment 1b) and that even when choices are present, they may be accompanied by obstacles (Table 2, Comment 1c). Another participant felt that women in particular are considered secondary to men when in the military, and this leads to being overlooked among the medical community at the VA (Table 2, Comment 1a).
Women debated individual empowerment and systematic change; specifically, whether they should expect the Veteran's Health Administration to provide a certain level of care (Table 2, Comment 2b) or whether they had personal responsibility to advocate for themselves (Table 2, Comment 2a). Additionally, participants emphasized that having individual doctors who are compassionate is an important factor in the expected quality of care (Table 2, Comment 2c). Clinical care can serve as a trigger for emotional distress in the process of obtaining care (Table 2, Comments 3a and 3b), and having peer support would be helpful (Table 2, Comments 4a and 4c). Having a better understanding of the reasons for and process of the gynecologic examination can be helpful (Table 2, Comment 4b).
Group education sessions
We designed the GES based on focus group input. Each GES took an average of 80 min (range 74–86). The original three topics planned for the GES were birth control, pelvic examinations, and mammograms. However, we changed the birth control session to menopause based on focus group feedback.
Overall, women were receptive to the GES and provided valuable insight into the group education model. The three main perceptions about the sessions were (1) the groups improved knowledge, (2) women learned from each other's stories, and (3) group settings can provide healing and a therapeutic place for discussion. Quotations and themes from the qualitative feedback sessions from the three GESs can be seen in Table 3. Themes included improved knowledge, feelings on group participation, and future topics for GESs.
GESs, group education sessions.
Women commented on how much they learned from the sessions and how that knowledge was useful both to themselves and also how they could disseminate knowledge to others (Table 3, Comments 3a–c).
The participants enjoyed learning from each other in the group. Many stated that hearing other women's experiences and stories taught them a great deal and provided insight into their own healthcare (Table 3, Comments 1a and 1c). A sense of camaraderie and connection permeated the groups as women shared stories and discussed their reproductive healthcare experiences (Table 3, Comment 2b and 2d). Participants suggested several topics for future GESs, including aging, heart disease, and diabetes (Table 3, Comments 3b and 3c). In particular, menopause was a popular topic requested (Table 3, Comment 3a) and led to the change of topic for the third GES.
The main critiques were about a lack of outreach to additional women in the area who may benefit from the classes and frustration around the same women attending VA events.
Surveys and knowledge assessment
Attitude change toward each preventive health topic is shown in Figures 1–3. While the samples were too small to comment on statistical significance, we can observe trends among the groups. After the pelvic examination GES (Fig. 1), subjects expressed better receptivity to the importance of Pap smears, early detection of cancer, obtaining a second opinion, and comfort with pelvic examinations. Marked improvement was observed in the numbers of subjects planning to have a mammogram (Fig. 2) in the next year (six before vs. nine after, with one being under 40 years old) and comfort with asking for a second opinion. After the menopause GES (Fig. 3), participants more strongly agreed that menopause is a natural aging process for women and better understood the etiology and typical symptoms of menopause. Subjects also indicated an increased comfort in discussing menopause with family or friends and a better understanding of the pros and cons of hormone replacement therapy. Interestingly, more participants felt that menopause triggers feelings of trauma after the menopause GES compared with before.
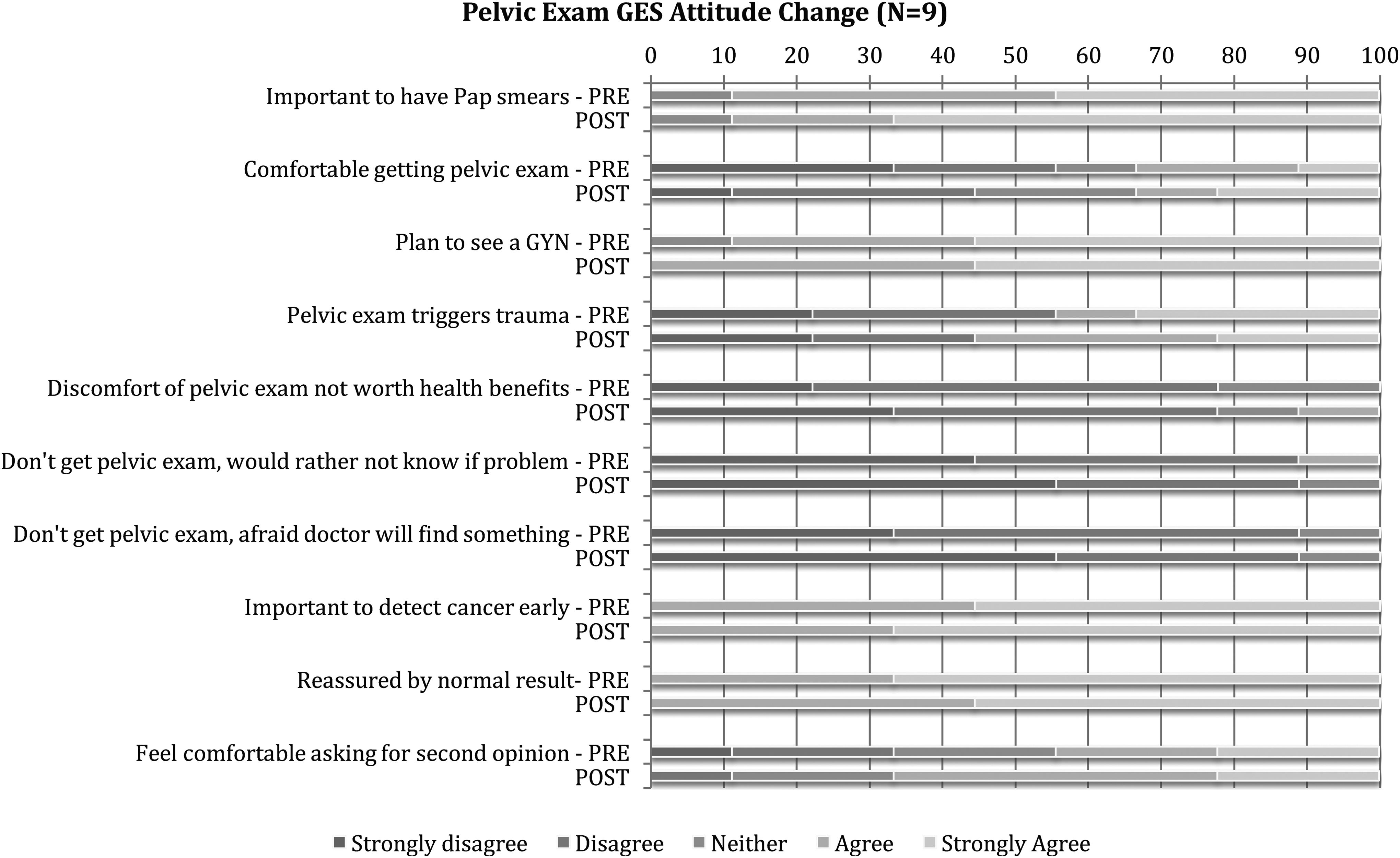
Attitude change after pelvic examination group education session (GES).

Attitude change after mammogram GES.
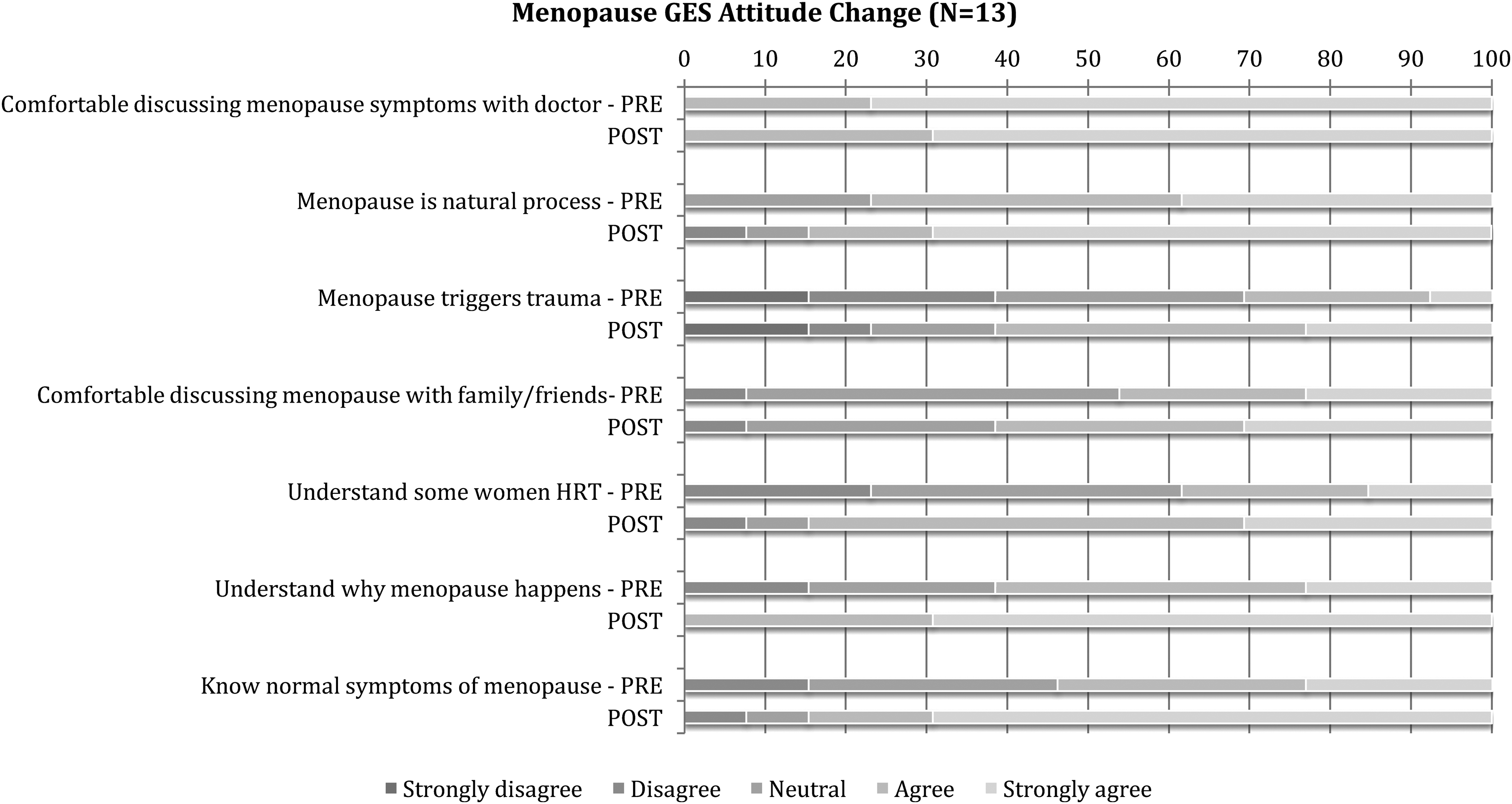
Attitude change after menopause GES.
Knowledge improved significantly with each GES. The pelvic examination GES mean score increased from 50.0% to 80.0% correct (p = 0.002), mammogram GES scores increased from 40.0% to 73.3% correct (p = 0.003), and menopause GES scores increased from 58.3% to 81.7% correct (p = 0.002).
Discussion
This study takes a unique approach in addressing sexual violence survivors' knowledge and attitudes toward reproductive preventive care through group education. In our trauma-informed approach, we sought to incorporate the voices of women veteran survivors of sexual trauma in designing our intervention and solicited feedback from participants for each element of the program. Furthermore, our program highlights the impact of trauma on obtaining preventive care and seeks to explore and ameliorate the challenges faced by survivors. Focus groups revealed a need for increased comfort and an opportunity to learn more about preventive healthcare. In fact, their main concern was increasing outreach efforts to more women veterans.
The intervention was well received and further sessions were requested on subjects, such as mental illness, sex life, heart disease, diabetes, alcohol consumption, diet, bone loss, and dental issues. The GESs improved comfort with sensitive reproductive health topics by encouraging women to consider alternative perspectives on health while engaging in shared decision-making with their providers. Additionally, the GESs substantially improved the participants' knowledge.
One interesting finding was the perception of triggering of each preventive health intervention; after the GES, women were less likely to feel that pelvic examinations triggered trauma, equally likely to feel that mammograms trigger trauma, and more likely to feel that menopause triggered trauma. We interpret these findings to indicate that while pelvic examinations and mammograms are more obvious triggers of trauma, many of the women may have never previously considered how menopause could trigger their trauma, and the GES provided the opportunity to recognize it.
Other studies have supported the use of group education to improve healthcare knowledge, access, or uptake. For example, both a systematic review and a randomized controlled trial found that group education improved uptake in breast cancer screening (Sabatino et al. 2012; Seven et al. 2015). GGPC is a relevant example for our GES model, in that it addresses reproductive health topics, is designed for an all-female audience, and focuses more on education and empowerment than on uptake of specific treatments or health outcomes. One potential disadvantage of GPC is that it requires a major system delivery modification, which can cause logistical challenges and barriers to its full implementation (Novick et al. 2015). Our GES, on the other hand, does not replace any form of medical care; it complements rather than modifies healthcare delivery.
Another model similar to our GES model is the SMV, also sometimes referred to as group medical visit. Both GPC and SMV are modifications to the standard delivery of healthcare. However, some patients may not want to disrupt their individual relationship with their provider, or implementation of group care may involve prohibitive logistical barriers (Heberlein et al. 2016; Jaber et al. 2006a; Novick et al. 2015). In our study, we separated the group education model from provision of care and offered to patients who seek group support and opportunities for additional education.
Our study differed from GPC and SMV, in that our groups are specifically designed for women with a history of trauma. This was addressed in several ways. Rather than repeatedly mentioning trauma specifically throughout the focus groups and GESs, each session was introduced in the context of trauma. Issues related to trauma were addressed, such as power, control, triggering, and respect. The presence of the psychologist helped to frame the trauma context and provide support and direction, remain attuned to signals that might be retriggered, and upon occasion, gently remind participants to not reveal specific traumatic material.
In working with sexual violence survivors, it is important to consider issues of sensitivity and confidentiality. Despite concerns, we did not encounter any such issues in our discussions. Previous studies have supported this finding; while providers are concerned about confidentiality as the most common reason that patients decline SMV participation, in fact, patients selectively chose, or filtered, what medical information they disclosed during a shared visit and expressed few concerns about confidentiality (Wong et al. 2015). The communal experience allowed them to learn from one another, and participants found the format to be empowering, motivating, and supportive (Wong et al. 2015). Patients with diabetes found that patients describe seeing their peers as change agents through support, role modeling, and encouraging accountability (Thompson et al. 2014).
Strengths of our study include its diverse subject population, its study design utilizing both focus groups and surveys, the standardized format of evaluation of all GESs, and the specific tailoring of groups to sexual violence survivors. To our knowledge, no other study has been published evaluating the utility and feasibility of a group educational model in this population. The study design allows us to obtain a quantitative evaluation combined with qualitative feedback, providing more detail and depth to the specific reactions and thoughts of participants, which can often be lost in quantitative-only assessment. Furthermore, GESs were designed only after obtaining direct input from the subject population in the form of focus groups, allowing the content, structure, and presentation style to be better designed and modified for the target group.
This study has several limitations. First, this was a pilot study and therefore our sample size was small. While we were pleased to find a statistically significant knowledge increase after each GES, we would still caution that our findings should be replicated and confirmed in larger samples. However, our study does demonstrate that GES is a feasible and acceptable model for imparting health knowledge and increasing engagement among women veterans, even with backgrounds that may be traditionally alienating and present an obstacle to obtaining care. Second, we did not assess knowledge retention in our subjects. Therefore, while subjects' knowledge increased significantly immediately after the session, we do not know whether this knowledge increase was retained over time, nor how it affected their health behavior. The demographics of our participants differ somewhat from the demographics of the overall female veteran population. Similarities include age (median 49.2 years in the female veteran population) and education level distribution (NCVAS 2016). However, our study population differs from the larger female veteran population, in that the majority of female veterans are white, while most of our participants were black or Latina, and higher proportion of our veterans were single compared with national data (NCVAS 2016). Last, our groups included women who volunteered to attend and therefore a selection bias cannot be avoided; women who are either too traumatized to attend such sessions or are unable to attend due to work, childcare, or other obstacles are difficult to capture in this type of intervention. Nonetheless, these GESs proved to be popular among women who attended, and more sessions were requested.
Conclusions
Women who have experienced sexual violence face many obstacles to obtaining preventive reproductive healthcare, and education can help to improve women's knowledge and acceptance of preventive health interventions. Group education is acceptable to sexual violence survivors and improves knowledge and attitude about preventive health. We anticipate that this intervention would be well received by the VHA given its commitment to women, survivors of sexual trauma, and quality care. Specifically, the Veterans Administration Center for Innovation (VACI) seeks to identify new approaches to urgent problems faced by veterans with a veteran-centered approach. Further research to verify these findings should concentrate on creating groups on more topics with higher numbers of women and evaluating knowledge and attitude improvement, including knowledge retention and provider training on trauma-informed care, as well as improvements in health outcomes. Health facilities seeking to improve opportunities for patient knowledge could consider creating group education programs.
Footnotes
Acknowledgments
This study was funded by the Reproductive Health Office of the Department of Veterans Affairs. The authors would like to acknowledge the New York Harbor Veterans Administration Women's Research Group, which contributed to the grant application, study design, and implementation, and the study participants who gave their time and effort to this study.
Author Disclosure Statement
This study was funded by the Reproductive Health Office of the Department of Veterans Affairs. No competing financial interests exist for any of the authors of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.