
Abstract
Abstract
More than 1 in 10 females (13%) reported being a victim of sexual assault in the 2012 Mortality, Morbidity, and Service Utilization Survey conducted in Haiti. This study aimed to describe the characteristics of sexual assault and its psychological consequences among female victims of sexual assault (patients) who presented to the Group for the Study of Kaposi's Sarcoma and Opportunistic Infections (GHESKIO) clinic in Port-au-Prince, Haiti, and determine which characteristics impact seeking medical evaluation or follow-up care. We conducted comparisons of the characteristics of sexual assault and psychological impact among female patients in Haiti by age stratification using chi-square or analysis of variance tests. Logistic regressions were used to assess the determinants of receiving medical evaluation within 72 h or returning for follow-up. A total of 4092 female patients presented from January 2006 to December 2015. Patients aged ≤10 years had significantly higher rates of assault by known assailants and a single assailant (p < 0.001). A total of 2650 (64.8%) patients reported at least one psychological condition, and 2458 patients (60.1%) returned within 6 months for follow-up. The adjusted odds ratio of returning for follow-up among patients exhibiting a psychological condition at first visit was 0.20 (0.17–0.24; p < 0.001), indicating that patients exhibiting a psychological condition were 80% less likely to return for follow-up. There are significant differences in sexual assault characteristics between child and adult patients. Psychological assessments could help predict the likelihood of return for follow-up. Health care workers should be trained to recognize psychological trauma as a risk factor for loss to follow-up.
Introduction
Sexual assault is a complex worldwide problem (WHO 2013) with medical, psychological, and legal components. In Haiti, approximately one in eight females (13%) reported being a victim of sexual violence in the 2012 Mortality, Morbidity, and Service Utilization Survey conducted by the Haitian Ministry of Health in a nationally representative sample of women aged 15–49 years (DHS 2013). Over 35,000 women and girls are estimated to have been victims of sexual violence in Port-au-Prince from 2004 to 2006; half of them were <18 years (Kolbe and Hutson 2006). The Haitians who are victims of sexual assault face unique challenges given the social and economic conditions. Nearly 50% of the households live in extreme poverty, 42% of the population do not have access to improved water sources, the illiteracy rate is 40%, and almost one-half of school-aged youth are not in school (Justesen et al. 2007; UNDP 2008). Women in Haiti face the dual challenges of oppressive poverty and gender inequality, such as economic dependency, which is associated with an increase in vulnerability to sexual violence (Deschamps et al. 2016; Fawzi et al. 2005).
The long-term physical and mental health impact of sexual assault is significant and depends on cultural factors (Lefley et al. 1993), individual responses to trauma (Combs et al. 2014), and access to care (Campbell 2008; Martin et al. 2007). Females who experience an assault have an increased risk of depression or anxiety (Koss et al. 1991), sexually transmitted diseases (Jenny et al. 1990), and pregnancy (Holmes et al. 1996; Mulugeta et al. 1998). Guidelines for care of females who experience a sexual assault universally focus on the prevention of HIV, sexually transmitted infections (STIs), and unwanted pregnancy (Callender and Dartnall 2011); however, resource constraints limit focus on psychological trauma. To reduce the risk of pregnancy and HIV infection, medical treatment should be received within 72 h of the assault (CDC 2015). To reduce the risk of psychological trauma, early intervention is important, but the specific timing remains unsettled particularly in sexual assault (Dworkin and Schumacher 2016; Hantman and Farchi 2015).
Low rates of reporting and a lack of follow-up care are major barriers to improving patient outcomes. Among victims of reported assaults in the United States, only an estimated 26–35% receive medical care after an assault (Resnick et al. 2000; Tjaden and Thoennes 2000). Although follow-up care is nearly universally recommended, the rate of patients returning for follow-up care is low globally (31–57%), especially for psychological care (Holmes et al. 1998; Martin et al. 2007). In the United States and Canada, psychiatric or mental health diagnoses have been associated with lower rates of follow-up (Ackerman et al. 2006; Darnell et al. 2015; Herbert et al. 1992); however, few studies have assessed which demographic, psychological, or assault characteristics are associated with returning for follow-up to provide more targeted programs (Forneris et al. 2013; Kazlauskas 2017; Qi et al. 2016).
The characteristics of an assault can vary significantly based on the age of the victim. Adolescent females (<20 years) are reported to be less likely to sustain physical injuries and more likely to know their assailant and to delay medical care (Muram et al. 1995; Peipert and Domagalski 1994). A 2-year longitudinal National Women's Study in the United States has shown that nearly 90% of females who experienced sexual assault as a child or adolescent never received a medical evaluation for the assault, much less psychological care (Hanson et al. 2001).
Limited literature is available on the characteristics, psychological outcomes, and follow-up care associated with sexual assault in Haiti. The objective of our study was twofold: (1) to describe the characteristics and psychological consequences of sexual assault among female victims who presented to Haitian Group for the Study of Kaposi's Sarcoma and Opportunistic Infections (GHESKIO) in Port-au-Prince, Haiti, and (2) to identify the predictors of a return for medical evaluation within 72 h or the use of follow-up services among females who were sexually assaulted.
Materials and Methods
Study setting and population
Founded in Port-au-Prince in 1982, GHESKIO provides free comprehensive services for HIV/AIDS and associated diseases. In 2000, GHESKIO opened a clinic to provide care for patients who are victims of sexual assault.
We conducted a retrospective analysis of the medical records of the 4092 female patients who received care in the GHESKIO sexual assault clinic from January 2006 to December 2015. We also included data on psychological outcomes for the patients who received care after the Psychosocial Evaluation and Follow-up Care of Victims of Sexual Assault questionnaire was introduced in 2005.
Upon presentation to GHESKIO, patients met with a psychologist, who provided counseling and also orally administered a standardized questionnaire that included sociodemographic variables, characteristics of the assault, and psychological outcomes. Based on the psychologist's evaluation, individual or couple counseling was offered.
With the patient's consent, a gynecologist then conducted a complete physical examination, including a genital examination, and recorded findings on a standardized sexual assault chart. All patients were offered HIV, syphilis, and pregnancy testing. If the patient reported that the assault occurred within the past 72 h, postexposure prophylaxis (PEP) for HIV was provided, emergency contraception was offered to reduce the risk of pregnancy, and medications were administered to empirically treat STIs (syphilis, gonorrhea, chlamydia, chancroid, and trichomoniasis), according to WHO (2007) and Ministry of Health guidelines. Each patient was scheduled for weekly follow-up appointments for the first month, with repeat HIV testing at 6 months.
Study measures
Sexual assault was defined as attempted or completed penetration of the patient's vagina or anus by penis, mouth, fingers, or other object, or of the patient's mouth by penis. Assault characteristics included the patient's relationship to the assailant, the location of the assault (Carrefour, Delmas, outside Part-au-Prince, Plaine, Port-au-Prince, Petion-ville, and unknown), the number of assailants, and coercion method. The relationship to the assailant was categorized as “known” or “unknown.” Known assailants included acquaintances, spouses/partners, parents, parent's partners, or other relatives, but not all patients were willing to divulge the identity of the assailant. Types of coercion used by the assailant included physical restraint, physical force or threat of physical force, use of weapons, drugs, and “other.” We defined attendance at follow-up care as at least one return visit to the sexual assault clinic.
The Psychosocial Evaluation and Follow-up Care of Victims of Sexual Assault questionnaire, used to assess the psychosocial variables, was orally administered by the psychologist; it evaluated and documented the background characteristics of the victim; the context of the rape; symptoms indicative of depression and posttraumatic stress disorder over time; emotional affect of the victim over time during psychological interviews; the victim's family's reaction over time to the rape; and the victim's partner's reaction over time. Questions required open-ended responses, yes/no answers, or multiple choice responses.
Data analysis
Demographic, clinical, and psychological data were deidentified and analyzed with R software. Patients were stratified by age (≤10, 11–18, 19–24, >24 years) to distinguish prepubescent children (<10) from adolescents below the age of consent (<18) and from mature victims (>24) for descriptive analyses (Tjaden and Thoennes 1998). Assault characteristics and psychological outcomes were compared using analysis of variance tests for continuous variables and chi-square tests or Fisher exact tests, as appropriate, for categorical variables.
Binary logistic regressions were performed to determine the key predictors of receiving a medical evaluation within 72 h of the assault and returning for a follow-up visit within 6 months. The association between the predictor variable and the dependent variable is displayed in odds ratios (ORs) or adjusted odds ratio (aOR) in the adjusted analyses. Covariates were included in the models if deemed to be of clinical relevance according to medical input from GHESKIO clinicians, magnitude of effect, or statistical significance (p < 0.05). Covariates include age stratification (categorical: ≤10, 11–18, 19–24, or >24 years), income (binary: >75 vs. ≤75 USD), education (binary: secondary or more vs. less than secondary), knowledge of the aggressor (binary: known vs. unknown aggressor), use or threatened physical violence (binary: yes vs. no), multiple assailants (binary: multiple assailants vs. single assailant), any prior sexual contact (binary: yes vs. no), year of assault (continuous), and the presence of any reported psychological symptoms at the first visit (binary: yes vs. no).
Results
Patient characteristics
Among the 4092 patients, the median age was 19 years (interquartile range [IQR] = 15–25); 355 (9%) were ≤10 years, 1601 (39%) were 11–18 years, 1086 (27%) were 19–24 years, and 1050 (26%) were ≥25 years (Table 1). The majority of patients were single (83%), had an income <75 USD per year (95%), and self-referred to the clinic (64%), although the characteristics of the assault varied by age.
Demographic Characteristics of Female Victims of Sexual Assault
Gourdes (GDS) converted to USD based on 67 GDS = 1 USD.
IQR, interquartile range; SD, standard deviation.
Patients <18 years of age were less educated, more likely to be single, and less likely to be sexually experienced. A significantly higher proportion of adolescents (<18 years) were assaulted by an acquaintance, but a lower proportion were assaulted by multiple assailants (Fig. 1). Children (≤10 years) had the highest proportion of assaults by known assailants (93% vs. 36%; p < 0.001) and the lowest proportion of assaults by multiple assailants (7% vs. 38%; p < 0.001). Adult patients (>18 years) experienced a higher proportion of physical violence or threat of physical violence during the assault, although physical violence or threat of physical violence was reported by the vast majority of patients (94%), regardless of age.
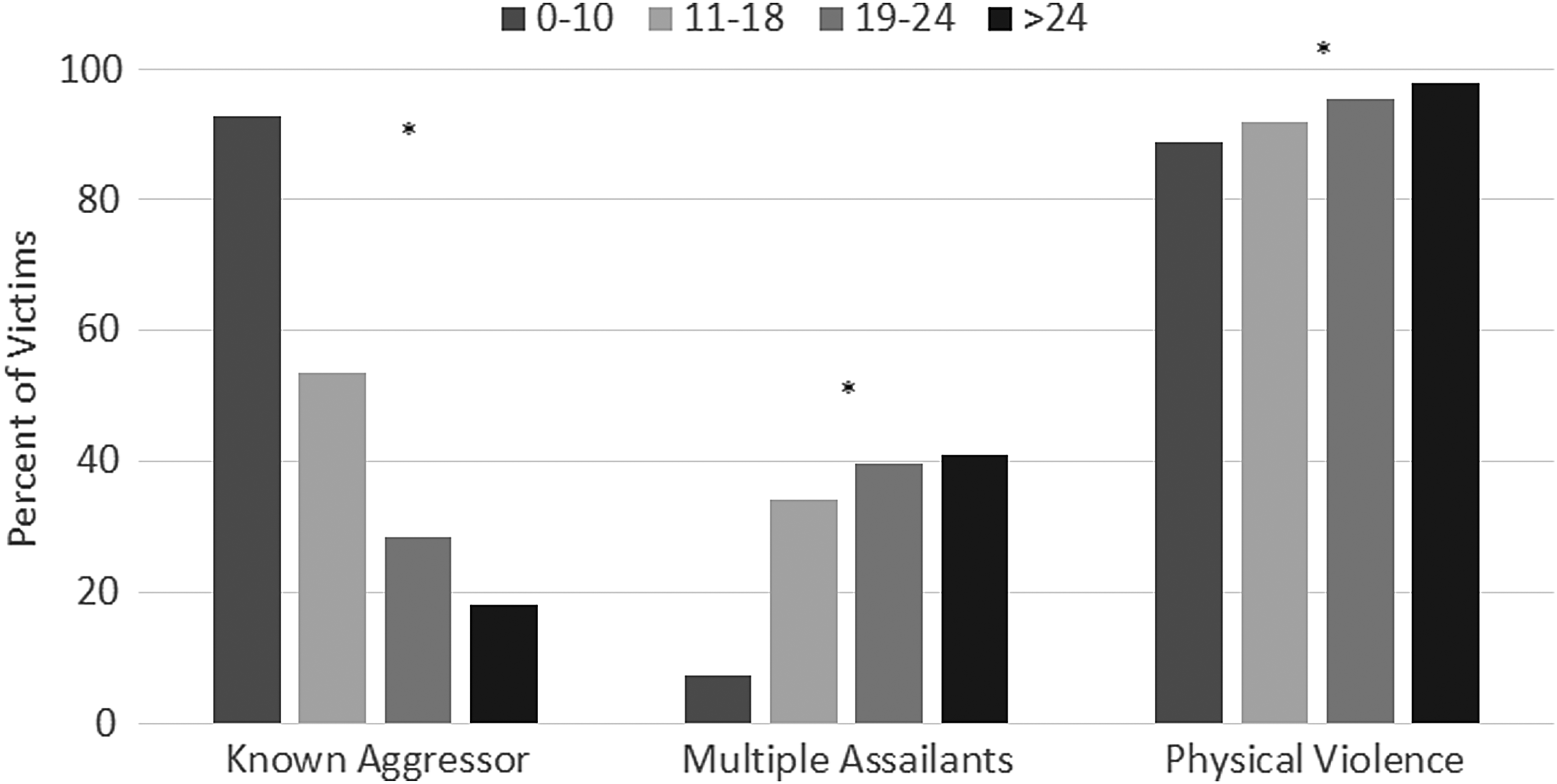
Characteristics of sexual assault by age of victim. *Represents p-value < 0.05.
Psychological characteristics
A total of 2650 (65%) patients reported at least one psychological condition (Table 2). Only 20% of children <10 years reported any symptom, compared with 51% in those >10 years (p < 0.001). Among those older than 10 years, the most common psychological symptoms were flat affect (33%), characterized by a lack of emotional response to the assault, fear (31%), flashbacks (22%), appetite disturbances (20%), and sleep disturbances (18%). The most common psychological symptoms were similar for children <10 years, but at much lower rates: flat affect (10%), appetite disturbance (7%), sleep disturbance (6%), flashbacks (5%), and somatization (4%). Only 1205 (31%) patients >10 years returned for three or more follow-up psychological visits; 70 (20%) patients ≤10 years returned for three or more follow-up psychological visits. Among those patients, the rate of flat affect, sleep disturbance, and appetite disturbance decreased from the first to third visits; however, no change was observed in the rates of fear or flashbacks between visits.
Psychological Characteristics
p-Values were calculated comparing victims ≤18 years with victims >18 years.
Represents p-value < 0.05.
Initial medical evaluation
Among the total cohort, 2840 (69%) received a medical evaluation within 72 h of the assault (Table 3), and of these, 2053 (72%) received emergency contraception and 2672 (94%) received HIV PEP. Emergency contraception and HIV prophylaxis were only offered if the medical evaluation was conducted within 72 h of the assault.
Follow-Up Care Characteristics Among Patients Presenting Within 72 H
p-Values were calculated comparing victims ≤18 years with victims >18 years.
Represents p-value < 0.05.
STI, sexually transmitted infection.
Less than 58% (206) of patients <10 years presented for medical evaluation within 72 h versus 981 (61%), 856 (79%), and 798 (76%) for patients aged 11–18, 19–24, and >24 years, respectively (Fig. 2). In univariable analysis, older age was associated with presentation for care within 72 h after the assault. In adjusted logistic regression analysis, patients aged 11–18 years were the least likely to visit the clinic within 72 h of the assault compared with other age cohorts (OR = 0–10, 1.36; 19–24, 1.68; >24, 1.28; p < 0.05 for all comparisons; Table 4). Higher income (aOR = 1.54; 95% confidence interval [CI] = 1.05–2.31), higher education (aOR = 1.41; 95% CI = 1.21–1.65), physical violence or threat of physical violence at the time of assault (aOR = 1.69; 95% CI = 1.26–2.27), and prior sexual contact (aOR = 1.38; 95% CI = 1.16–1.65) were associated with seeking care within 72 h of the assault. Assault by a known assailant (aOR = 0.65; 95% CI = 0.55–0.76) and multiple assailants (aOR = 0.83; 95% CI = 0.71–0.98) were associated with delays in seeking care.
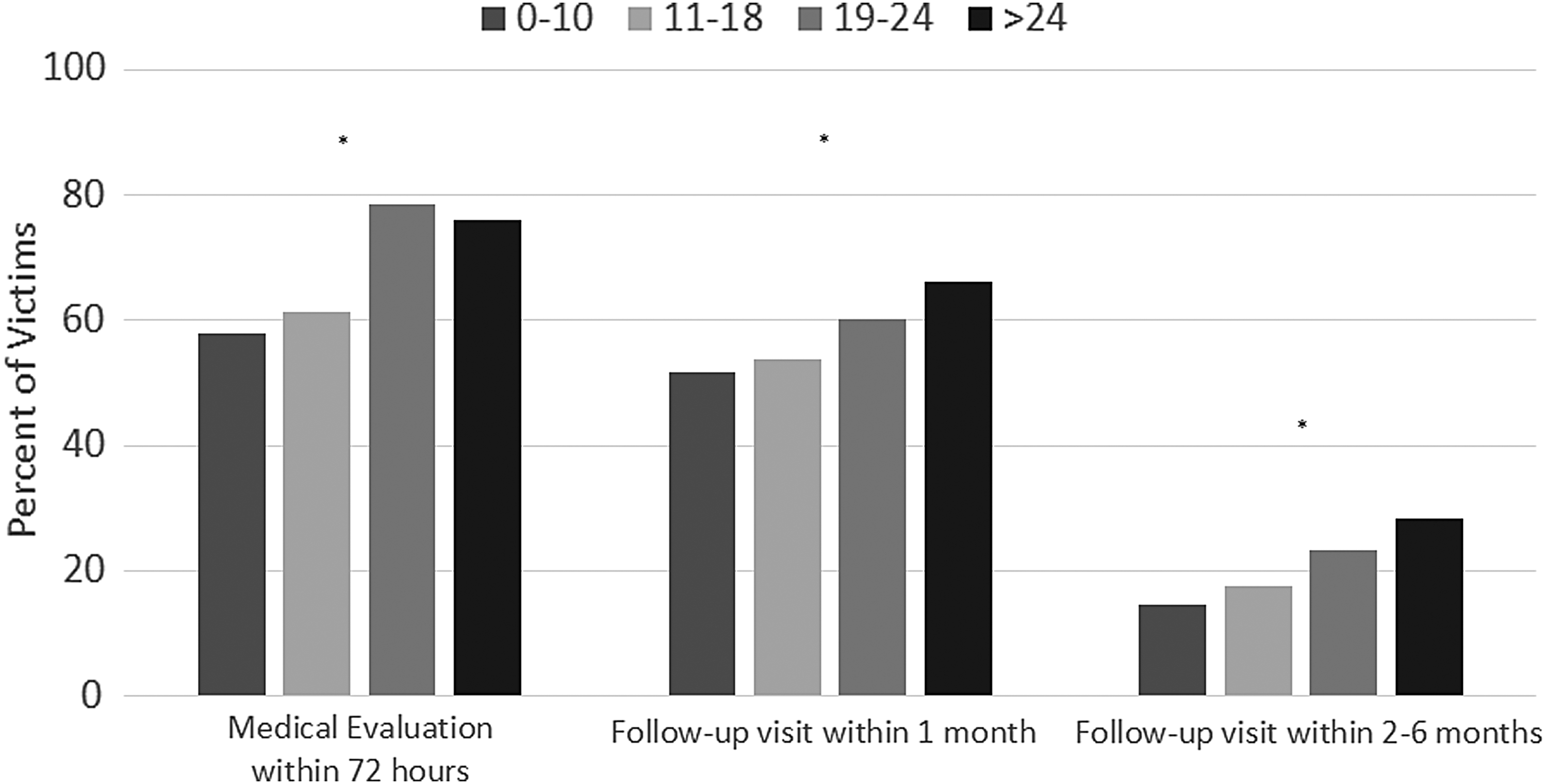
Timing of initial evaluation and rates of retention during follow-up care. *Represents p-value < 0.05.
Regression Results
CI, confidence interval; OR, odds ratio.
Follow-up care
The median number of follow-up medical visits was 2 (IQR = 1–4) and the median number of follow-up psychological visits was 2 (IQR = 1–4). Among all patients, 2396 (59%) returned for medical or psychological evaluation within 1 month. Follow-up rates within 2–6 months after the initial evaluation were considerably lower (22% within 2–6 months vs. 59% within 1 month). Of the patients who returned for a follow-up visit 2–6 months later, 820 patients (93%) had attended a follow-up visit within the first month.
In adjusted logistic regression models, patients >18 years were more likely to return for follow-up within 1 month. Reporting any psychological symptom at the first visit (aOR = 0.20; 95% CI = 0.17–0.24), knowing the aggressor (aOR = 0.82: 95% CI = 0.69–0.97), or having prior sexual contact (aOR = 0.83; 95% CI = 0.67–1.01) reduced the odds of returning for follow-up, while having at least a secondary education increased the odds of returning for follow-up (aOR = 1.40; 95% CI = 1.18–1.67). Similar results were found in the adjusted logistic regression analysis for returning for follow-up within 2–6 months.
Discussion
Our findings indicate that the majority of females who are victims of sexual assault present with both physical and psychological trauma after the assault. The range of patients' age is wide (<1 to 86) with a significant proportion of patients <10 years of age.
Significant differences in the characteristics of the assault were observed across the four age cohorts, consistent with reports from other countries (Muram et al. 1995; Peipert and Domagalski 1994). Adult patients were more likely to be assaulted by multiple assailants, whereas those <18 years of age were more likely to be assaulted by a known aggressor. Even among the adolescent population, children <10 years of age were significantly more likely to be assaulted by an acquaintance and less likely to be assaulted by multiple assailants compared with children 11–18 years old.
Across the entire observed population, 94% of female patients experienced a sexual assault where physical violence was used or threatened, which is a uniquely high rate compared with prior studies. This may not be representative of the larger population of females who were victims of sexual assault in Haiti; physical injuries sustained during the assault may be one of the motivations for presenting to the clinic. A large proportion of the observed assaults (35%) were by multiple assailants. Other countries have reported an estimated 2–28% of sexual assaults occurring with multiple perpetrators, although these types of assaults are expected to be underreported due to social stigma (Dartnall and Jewkes 2013; Vetten and Haffejee 2006). When multiple assailants are involved, however, the assault is reportedly more violent and more likely to involve a weapon (Woodhams and Cooke 2012).
The majority (65%) of patients reported at least one of the assessed psychological conditions. Psychological conditions were less likely to be reported in those <10 years of age. This low frequency of reported psychological symptoms may reflect the lack of specialized tools to assess psychological conditions for that age group. Future research should aim to develop tools that are adapted for younger patients.
Although causality cannot be determined, our findings suggest that several characteristics are associated with seeking care within 72 h. Females who experienced the use or threat of physical violence during the assault were more likely to present within this time window, whereas those who were assaulted by an acquaintance or multiple assailants were less likely to seek early care. Women who were assaulted by an acquaintance may have been less likely to seek early care due to self-blame (Moor and Farchi 2011). Younger patients were also likely to delay presentation to care. This is in line with findings previously reported that adult victims received care closer to the time of the assault (Muram et al. 1995). Minors typically have less agency in their own health care decisions, which may help explain the disparities in follow-up rates among this group. In addition, abusive home environments may further influence a minor's ability to receive care after sexual assault. Further research is needed to fully understand the factors associated with delays in seeking care.
Although the rates of follow-up within 1 month at GHESKIO were generally higher than those reported in the literature (Holmes et al. 1998; Martin et al. 2007), they are still low (59%) and drop significantly for follow-up >1 month after the initial visit. Socioeconomic and environmental factors may impact the rate of follow-up among patients in Haiti. From the adjusted logistic regression analysis, we found that knowing the aggressor reduced the odds of returning for follow-up, whereas being aged ≥18 years and having at least a secondary education increased the odds of returning for follow-up. Perhaps of greatest concern, by far the lowest odds of returning for follow-up care were associated with reporting a psychological symptom during the first medical evaluation. This suggests that patients who may benefit the most from continuing follow-up support are also the least likely to seek it.
The incomplete level of follow-up and the associated underutilization of health services could be due to typical barriers to traditional follow-up services, avoidance behavior and denial, or not understanding the need or benefit of both early medical and psychological intervention and regular follow-up. Avoidance is a core psychological symptom that directly and negatively affects the utilization of health care services since they can be processed as reminders of the trauma (Darnell et al. 2015; Dworkin and Schumacher 2016). Females with poor psychosocial functioning, transient living, and lower socioeconomic class are disproportionally affected by sexual assault (Herbert et al. 1992), which is consistent with the characteristics of the patients in this study (5.2% with income >75 USD per year). These characteristics are barriers to the use of traditional follow-up services. Follow-up may also be associated with the number and severity of trauma symptoms in the posttrauma period, although emerging research points to the potential usefulness of heart rate during acute care as a predictor of negative sequelae, including avoidance (Marsac et al. 2014; McNally et al. 2003; Sareen 2014). Since reporting psychological symptoms is strongly associated with a low likelihood of returning for care, health care workers might use the psychological assessments at the time of initial evaluation to identify patients at higher risk of loss to follow-up. In addition, immediate brief psychological intervention may be critical to provide patients with psychological care before loss to follow-up occurs. We also found that children <10 years of age are unlikely to return for follow-up care. Since children are dependent on parents or guardians, further educational efforts may be needed to explain the relevance of medical and psychological care to the caretakers of children who experience sexual assault.
The main limitation of this retrospective study is the use of clinic registry data that combine provider-recorded medical information and patient self-reported information. Self-reported information, such as psychological symptoms, may be underreported due to societal stigma. It is unclear how many sexual assaults go entirely unreported; therefore, the patients reporting to this clinic may not be a representative sample. Minimal information regarding sexual assault in Haiti has been previously reported. Therefore, this information has important implications for improving services for females who were victims of sexual assault, especially with regard to better adherence to follow-up psychological counseling and medical care.
Medical and psychological care in the aftermath of a sexual assault is critical, and adherence to follow-up treatment is poor. Many patients cannot access or do not recognize the importance of medical, psychological, and legal services after an assault. Innovative programs with community involvement that are culturally adapted to Haiti are needed to prevent sexual assault and provide timely assistance to females who were victims.
Conclusions
Psychological characteristics experienced by victims of sexual assault and sexual assault interventions are understudied in low- and middle-income countries (Bisson et al. 2013; Dworkin and Schumacher 2016). This research shows that the medical and psychological consequences of sexual assault are significant. There are significant differences in sexual assault characteristics between child and adult patients, emphasizing the need for specialized training for health care workers who treat children <10 years of age. A number of patient baseline characteristics, such as psychological conditions during the first visit, education, and age, can serve as important early indicators of likely loss to follow-up for psychological counseling.
Footnotes
Acknowledgment
We thank Dr. Serena P. Koenig for her assistance and careful review of the article.
Author Disclosure Statement
The authors have no competing financial interests.